
Abstract
Background:
Tobacco use is a major risk factor for cardiovascular disease (CVD) and is the leading preventable cause of death, disease, and disability in the United States. The CDC's Well-Integrated Screening and Evaluation for Women Across the Nation (WISEWOMAN) program addresses the heart health of low-income under- or uninsured women between the ages of 40 and 64 years. This article discusses WISEWOMAN's key approaches to smoking cessation and their impact on WISEWOMAN participants' cardiovascular health.
Methods:
A longitudinal retrospective analysis was conducted using data from 21 funded CDC programs from July 2008 to June 2013. Data were collected on 149,767 women to assess CVD risk, smoking status, and utilization of programs related to tobacco cessation.
Results:
The overall prevalence of smoking among the WISEWOMAN population during this period was 28%. Increases in referrals to tobacco quitlines, tobacco-cessation counseling, lifestyle interventions, and other community-based tobacco-cessation programs contributed to a 15% smoking-cessation rate among smokers who returned for a rescreening assessment over the 5-year program period.
Conclusion:
The WISEWOMAN program has observed a smoking-cessation rate of 15% over the 5-year program period. WISEWOMAN's key approaches include continuous technical assistance that highlights quitline referrals, motivational interviewing done by program staff, and professional-development strategies for WISEWOMAN healthcare providers. WISEWOMAN will continue its programmatic emphasis on smoking cessation by partnering with state tobacco-cessation programs to work toward a lower smoking-prevalence rate among program participants.
Introduction
I
The CDC's Well-Integrated Screening and Evaluation for Women Across the Nation (WISEWOMAN) program addresses the heart health of women who are under- or uninsured and low income, with a priority population between the ages of 40 and 64 years. 5 Eligible women must be enrolled in the National Breast and Cervical Cancer Early Detection Program (NBCCEDP), which is administered by CDC and provides cancer-screening services. The WISEWOMAN program funded 19 state health departments and 2 Alaska Native organizations between 2008 and 2013. The WISEWOMAN programs provide cardiovascular health screenings, lifestyle interventions (LSIs), and community-based resources to enrolled women. The program focuses on the reduction and prevention of five major risk factors for heart disease: hypertension (high blood pressure), diabetes, high cholesterol, overweight/obesity, and smoking. Women enrolled in WISEWOMAN have greater health disparities resulting from minority racial and ethnic group membership, low socioeconomic status, and limited access to healthcare services. 6 –11
Between July 1, 2008, and June 30, 2013, WISEWOMAN provided 217,415 CVD screenings to 149,767 low-income women, 44% of whom were members of racial and ethnic minorities. Approximately 90% of WISEWOMAN participants have at least one of the five major risk factors for CVD. 5
Cigarette smoking and exposure to secondhand smoke are major risk factors for CVD. 12–13 Cigarette smoking causes more than 151,000 deaths from cardiovascular diseases each year. 13 The national prevalence of smoking among women is 15.8%. 14 The overall smoking prevalence among WISEWOMAN participants is 28%, which is much higher than the national average.
Proven strategies to help people quit smoking include advice to quit from healthcare providers; individual, group, and telephone counseling; and seven FDA-approved cessation medications. 15 Over the past 10 years, telephone quitlines providing counseling services to smokers who wish to quit have been established in all 50 states, the District of Columbia, Puerto Rico, and Guam. 16 Quitlines increase quit rates, have broad reach, and are effective with diverse populations. 15 Quitlines provide callers with a range of services, including counseling, practical information on how to quit, referral to other cessation resources, mailed self-help materials, and, in many cases, free or discounted cessation medication. 17 Most state quitlines have implemented a fax-referral system. 18 In this model, after advising a smoker to quit and assessing the smoker's readiness to quit, the healthcare provider faxes a referral form to the quitline if the smoker is interested in quitting and agrees to be referred. Counselors at the quitline will then contact the smoker to begin cessation services. Such fax-referral systems have proved effective in providing services to smokers who want to quit. 19 In addition, some state quitlines, are beginning to explore e-referrals, in which a provider refers a patient to the quitline electronically from the patient's electronic health records, 19–20 along with the CDC's compilations of current best practices for comprehensive tobacco control programs. 21
A complementary evidence-based strategy is for tobacco-control programs to work with healthcare providers to increase the advice to smokers to quit. 15 The 5-As framework (ask, advise, assess, assist and arrange) gives healthcare providers an opportunity to affect the outcome at each clinical encounter—whether through assessing a smoker's willingness to make a quit attempt, encouraging a quit attempt, offering assistance with quitting, assisting with problem solving, or, at the very least, providing motivation to quit. 15
WISEWOMAN program activities
Between 2008 and 2013, the WISEWOMAN program's emphasis on reducing smoking and secondhand exposure increased. Program guidance for smoking cessation stressed quitline referrals and feedback to WISEWOMAN programs on the smoking status of women who participated. Technical assistance to funded programs on smoking cessation was two-pronged. First, WISEWOMAN program staff was advised to include tobacco-use cessation in motivational interviewing with each woman who smoked. Second, professional development was conducted for healthcare providers so that the 5-As framework (ask about tobacco use, advise to quit, assess willingness to make a quit attempt, assist in quit attempt, and arrange follow-up) was used with all patients at every clinic visit. Assistance in quit attempts included linkages to quitlines and referrals to appropriate community cessation services. Community referrals to appropriate cessation services are an integral part of the program. In addition, LSIs provide cessation counseling as part of the intervention curriculum as mentioned in CDC's WISEWOMAN program guidance and resource document.
WISEWOMAN program examples
State program
The Pennsylvania WISEWOMAN (PAWW) program is an example of a systematic public health approach to decrease tobacco use among PAWW clients and the larger community population. Funded in 2008, PAWW reported a smoking prevalence of 25% at baseline screening in a small number of clinics in limited geographic areas. At this early point in the program, no participants were referred to the state quitline, and only 4% were linked to community-based tobacco-cessation resources. In the following 24 to 36 months, the program expanded its reach to new clinics, service providers, and geographic areas in the state. From July 1, 2012, to June 30, 2013, the program documented a smoking rate of 34% among participants across the statewide program. To reduce this high prevalence rate, the program worked more aggressively with clinicians. A key goal was to increase referrals to tobacco-cessation support services in community-based organizations and through the state quitline. Clinicians in the healthcare system were identified as those most likely to make referrals to cessation services. The program worked with the Pennsylvania Department of Health Tobacco Prevention and Control Division (TPC) and the Pennsylvania Free Quitline Fax to Quit Program to train clinicians on tobacco-cessation services available to all clinic patients, including WISEWOMAN participants. As a result of this partnership, provider knowledge of available cessation resources and referral procedures increased. The training program was piloted in two clinics before statewide implementation.
The two pilot clinics were located in western Pennsylvania. At each clinic, every staff person—from the front-desk clerk to the clinic manager who interacted with clients—participated in the training. As a result, all clinic staff had a uniform understanding of the referral process and the ability to explain the services offered to a client. The on-line training took approximately 45 minutes to 1 hour to complete, covering current guidelines for and implementation of smoking-cessation interventions, the complexity of smoking behavior, nicotine addiction, brief intervention strategies using the 5-As framework, a summary of appropriate cessation pharmacotherapy, and Fax to Quit Program procedures and reporting. 15 Members of the clinic staff were asked to commit to system changes, such as including patient Fax to Quit forms in standard operating procedures and providing ongoing training for new employees. Program monitoring and evaluation were important parts of the program and included confirmation of Fax to Quit Program referrals through reports and followup assessments. Following the pilot, the program recruited 680 professionals statewide to receive the on-line Fax to Quit Program training (Table 1). These professionals provided healthcare services to women enrolled in NBCCEDP and in the WISEWOMAN program. These healthcare providers also served primarily low-income, disadvantaged people who were not enrolled in NBCCEDP and WISEWOMAN; the referral procedures were implemented for all clinic clients. The program continued to work with TPC to promote additional cessation services and training opportunities. By June 2013, 91% of PAWW smokers were referred to cessation programs, including the state quitline, through the Fax to Quit Program referral process.
Tribal program
The Southeast Alaska Regional Health Consortium (SEARHC) is a comprehensive healthcare services organization that serves Alaska Natives and other racial and ethnic groups living in southeast Alaska. The SEARHC WISEWOMAN (SEARHC WW) program has been funded since 1999, with approximately 68% of participants self-identifying as non-Hispanic American Indian/Alaskan Native women. Remaining participants identify as white, non-Hispanic black, and Asian/Pacific Islanders.
SEARHC Health System changes were implemented at numerous clinics serving WISEWOMAN participants. Unlike many state-funded programs, SEARHC noted that, at baseline screening, few participants accepted the offer to receive counseling services through the proactive Alaska (AK) Quitline. Most tobacco users in the program were Alaska Natives, who are most comfortable with in-person services delivery. To address this cultural norm, SEARHC had three certified tobacco-cessation counselors who offered counseling services throughout the region; two of the counselors were based in the largest communities in southeast Alaska. FDA-approved cessation medications were provided by healthcare professionals to all SEARHC WW smokers, as appropriate. Forty-six percent of SEARHC WW smokers received one-on-one counseling services medication therapy, as appropriate.
Since 2000, the SEARHC WW and the SEARHC Women's Health (SEARHC WH) program have worked closely with community partners and other programs supported by SEARHC to implement environmental approaches to reduce tobacco use and eliminate exposure to secondhand smoke. These environmental approaches included increased tobacco pricing, smoke-free ordinances and regulations, voluntary smoke-free businesses, smoke-free tribal facilities, and communication campaigns. Community partners and SEARHC worked together, and tobacco taxes were raised in the two largest service areas: Juneau in 2003 and Sitka in 2005. The tax in Juneau was increased in 2009 from $0.30 a pack to $1. 22–23 The tax revenue in Sitka was dedicated to funding the community hospital, and a portion was used for community-based tobacco-cessation services that are available to all tobacco users in the community, including women enrolled in WISEWOMAN.
In partnership with the SEARHC Tobacco and Diabetes programs, SEARHC WW and SEARHC WH conducted a social-marketing project targeting women ages 25–64. Begun in 2008 and continuing for 3 years, the social-marketing campaign used a phased approach. At different times during the 3 years, various media strategies and outlets were used. Ads were placed on the radio and in print publications. Postcards with tobacco-free messages were mailed to women. Monthly “Tips to Quit” flyers were also mailed. Ads were placed in theaters before the feature films. Flyers and posters with tobacco-free messages were placed in clinics and public areas in the communities. Finally, earned-media strategies were used, resulting in additional attention to health issues in print and broadcast media. Earned-media stories included profiles of women who quit smoking and the resulting health benefits they enjoyed. The 3-year media campaign coincided with the first 3 years of the WISEWOMAN funding period. Beginning in 2009, smoke-free housing policies were promoted in Juneau, Sitka, and Petersburg.
The synergy of environmental and health systems approaches contributes to changing social norms and creating a supportive environment for smokers who quit. SEARHC's Behavior Risk Factor Survey was conducted in the service area; using those data, they found a significant decrease in the number of Alaska Native/American Indians smokers from 37% in 2005 to 24% in 2011. Data from the SEARHC WW program reflected this trend. Of participants who received cessation counseling, 25% reported not smoking at a clinic rescreening visit at least 12 months later. In contrast, of participants who did not receive counseling to quit, 15% reported not smoking at their last rescreening visit.
Materials and Methods
WISEWOMAN program activities ultimately have an impact on the women served. When examining aggregate data for all 21 funded WISEWOMAN programs, national trends emerge. These data depict a population group that is at risk for cardiovascular disease as a result of smoking and exposure to secondhand smoke. The data also show reductions in the smoking prevalence among WISEWOMAN participants.
The WISEWOMAN program collected cardiovascular health-screening data from 19 state health departments and 2 tribal organizations in Alaska from July 1, 2008, to June 30, 2013. This analysis contains longitudinal data gathered on the 149,767 women screened in the program. The variables of interest are smoking status (smoker or nonsmoker), race/ethnicity (non-Hispanic white, non-Hispanic black, Hispanic, non-Hispanic Asian/Pacific Islander, and non-Hispanic American Indian/Alaskan Native), age (younger than 40, 40–49, 50–64, 65 and older), blood pressure (systolic blood pressure ≥140 mmHg and/or diastolic blood pressure ≥90 mmHg), blood cholesterol (total cholesterol ≥240 mg/dL), blood glucose (≥125 mg/dL) or glycated hemoglobin (A1c) (≥6.5%), body mass index (BMI) (≥25), quitline referrals (yes or no), tobacco counseling LSIs (yes or no), and tobacco-cessation community-based resources (yes or no). All analyses were performed using SAS Version 9.3 software (Cary, NC). Odds ratios (OR) using logistic regression models were used to determine differences in CVD risk factors between smokers and nonsmokers and what attributes increased the likelihood that a woman would quit smoking. All adjusted ORs are reported with a 95% confidence interval (CI). For all final analyses, a forward-selection approach was adopted that includes the most significant variables (p<0.05). To increase the statistical power and reliability of estimates, this article aggregates 5 years of data for the WISEWOMAN program.
Results
Demographic variables
The 149,767 participants screened received 217,415 screenings from July 1, 2008, to June 30, 2013; 44% were racial and ethnic minorities. Education levels varied within the program; the majority of participants (68%) had received either a high school (or equivalent) or some college (or higher) education. Ninety-six percent of participants were in the priority population age range of 40–64 years (Figs. 1 –3). The prevalence of CVD risk factors for these women is as follows: 40% were hypertensive, 31% had high cholesterol levels, 17% were diabetic, and 76% were overweight or obese (Table 2).
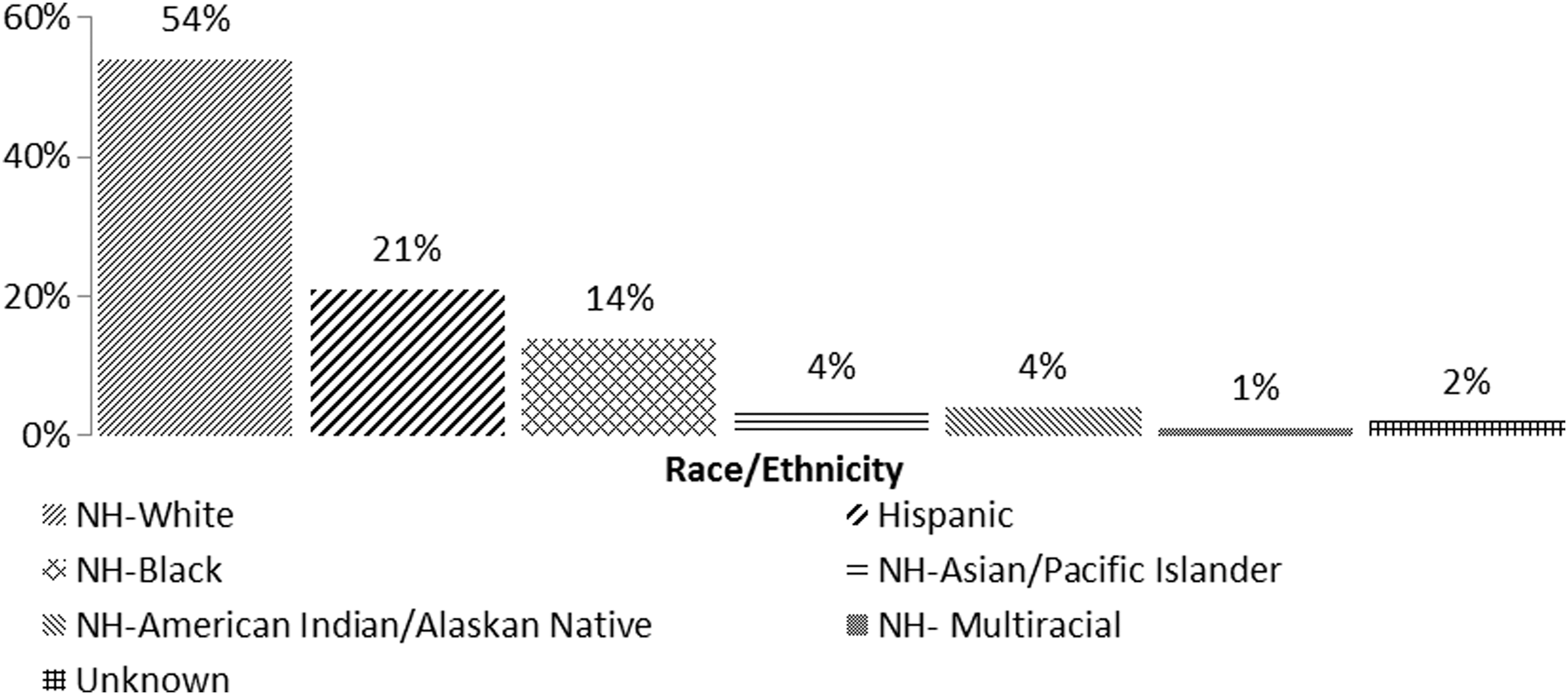
Racial and ethnic profile of WISEWOMAN participants: June 1, 2008, through July 30, 2013.
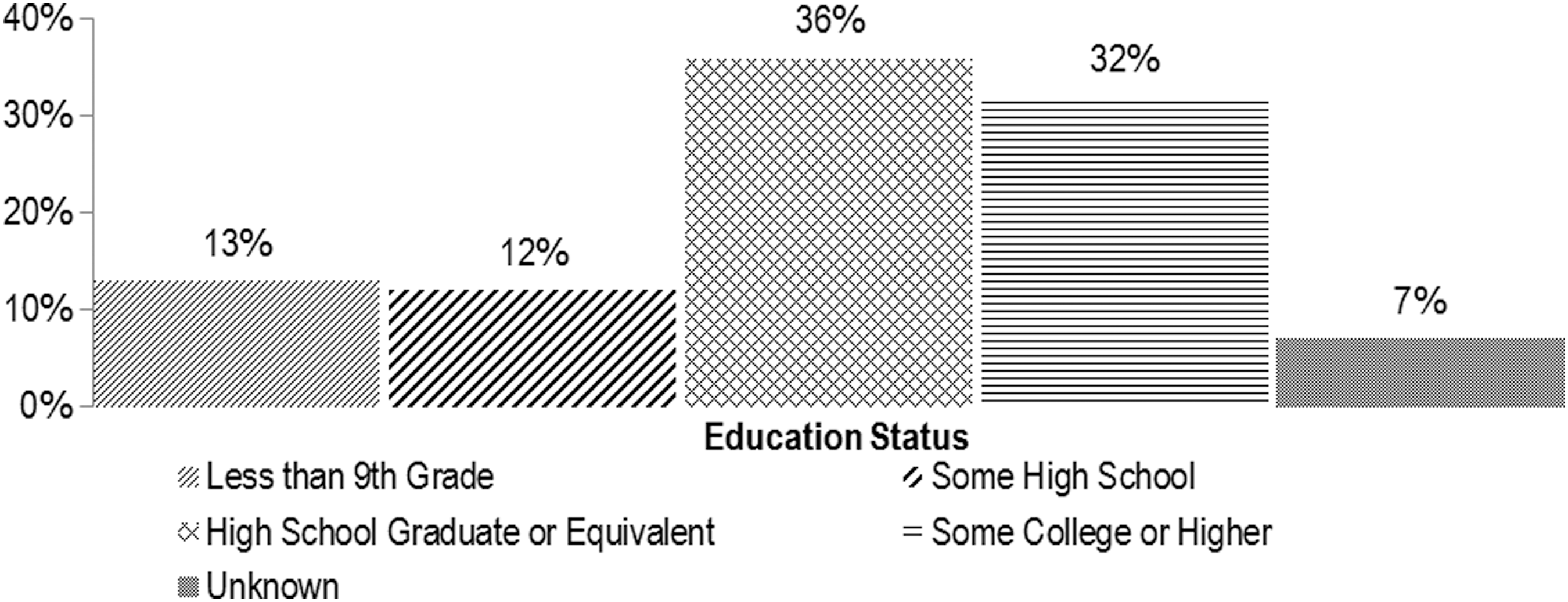
Education profile of WISEWOMAN participants: June 1, 2008, through July 30, 2013.
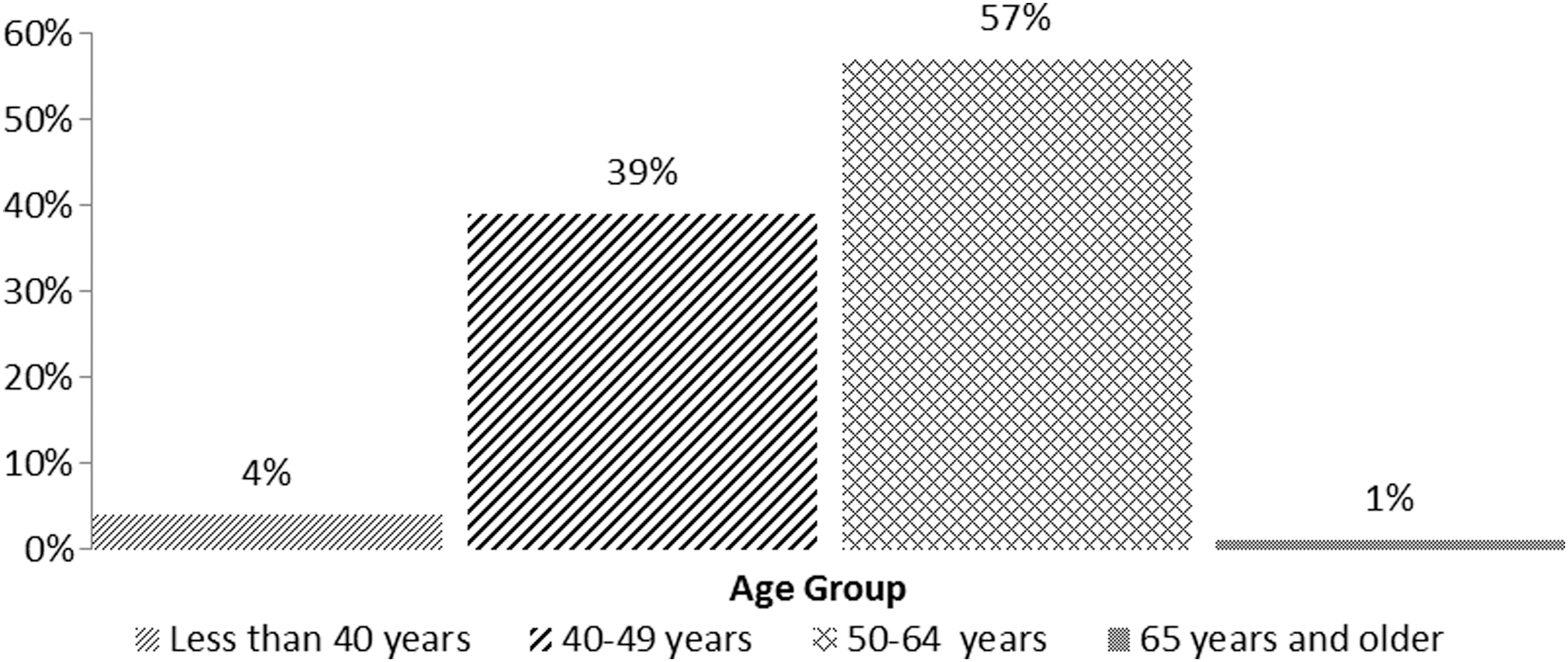
Age distribution of WISEWOMAN participants: June 1, 2008, through July 30, 2013 <1%.
Missing and excluded values were not included in this table.
Hypertension: normal blood pressure, average SBP <120 mm Hg and average DBP <80 mmHg; prehypertension, average SBP 120–139 mmHg or average DBP 80–89 mmHg; hypertension, average SBP ≥140 mmHg or average DBP ≥90 mmHg or taking medication for high blood pressure.
Cholesterol: normal total cholesterol (fasting/nonfasting), <200 mg/dL; borderline high cholesterol, total cholesterol (fasting/nonfasting) 200–239 mg/dL; high cholesterol, total cholesterol (fasting/nonfasting) ≥240 mg/dL or taking medication for high cholesterol.
Diabetes: normal glucose, fasting glucose <100 mg/dL, nonfasting glucose <140 mg/dL, or A1c <5.7%; prediabetes, fasting glucose 100–125 mg/dL or nonfasting glucose 140–199 mg/dL or A1c ≥5.7%; diabetes, fasting glucose >125 mg/dL, nonfasting glucose>199 mg/dL, A1c ≥6.5%, history of diabetes, or taking medication for diabetes.
Smoking: participant reports smoking every day or some days.
Secondhand smoke:
Body mass index: normal, <24; overweight, 25–30; obese, ≥30.
Alc, glycated hemoglobin; DBP, diastolic blood pressure; SBP, systolic blood pressure.
The overall prevalence of smoking among the WISEWOMAN population was 28%. When stratified by race, non-Hispanic American Indian/Alaskan Natives had the highest prevalence of smoking at 42%, with non-Hispanic whites following at 35% and non-Hispanic blacks at 27%. Hispanics and non-Hispanic Asian and Pacific Islanders had the lowest smoking prevalence at 9% and 4%, respectively.
Smoking prevalence among WISEWOMAN participants varied by education status and age group, as well as location. Among those with some high school education, 36% were smokers, whereas 26% of women with some college education were smokers. When participants were stratified by age, the prevalence of smoking decreased as women aged. Thirty-two percent of women 40–49 years old were smokers, compared to 24% of women 50–64 years old. As expected, the prevalence of smoking also varied markedly from program to program. West Virginia had the highest prevalence of smokers at 43%; Utah and California had the lowest, with 8% and 7%, respectively. Among WISEWOMAN participants who smoked, 38% were hypertensive, 30% had high cholesterol levels, 69% were overweight or obese, and 14% had diabetes. There was a statistically significant difference in BMI among smokers and nonsmokers. Smokers had a decreased likelihood of being obese when compared to nonsmokers (OR=0.59, 95% CI: 0.58–0.61).
Beginning on July 1, 2010, WISEWOMAN added a question about secondhand smoke exposure to the screening assessment. Among all participants, 16% were exposed to secondhand smoke while at home. However, when they were stratified by smoking status, we found that 8% of nonsmokers were exposed to secondhand smoke. WISEWOMAN smokers were at additional risk, as 43% of them were also exposed to secondhand smoke while at home. Also of note is that 75% of these smokers were exposed to secondhand smoke every day.
Program resources
The WISEWOMAN program included quitline linkages, cessation-counseling referrals, and community-based cessation programs. Smoking-cessation interventions included proactive telephone quitline referral. Tobacco-cessation counseling was included as part of LSIs, along with referral to other community-based tobacco-cessation programs. Proactive quitlines provide many services, including individualized tobacco counseling, support for quit attempts, help to prevent relapse, educational materials, and, in some cases, nicotine-replacement therapy or other cessation medications. Counseling, as part of LSIs, includes one-on-one sessions with a tobacco-cessation specialist who provides support for quitting. Community-based tobacco-cessation programs include group classes, such as those offered by the American Cancer Society, American Lung Association, or other community-based organizations.
The impact of WISEWOMAN's increased emphasis on reducing tobacco use among participants is seen by the trend in linkages to quitlines. In the first year of the WISEWOMAN program (July 1, 2008, through June 30, 2009), 32% of screening visits by a current smoker were linked to a quitline (from a total of 8,327 screening visits with current smokers, 2,660 were linked at least once to a quitline). In the fifth year of the program (July 1, 2012, through June 30, 2013), 38% of screening visits by current smokers were linked to a quitline (from a total of 12,170 screening visits with current smokers, 4,620 were linked at least once to a quitline), a rate increase of 6%. Overall, the cumulative referrals to state quitlines from July 1, 2008, through June 30, 2013, were 27,408. Some smokers were linked more than once to a quitline; therefore, 20,100 unique visits by smokers were referred at least once to a quitline, representing approximately 36% of all WISEWOMAN screening visits by smokers (Table 3).
The n for tobacco cessation as part of an LSI is lower, as this service was not fully implemented until the fourth program year, which started on July 1, 2011.
LSI, lifestyle intervention.
Notably, the use of tobacco-cessation counseling greatly increased in the last 2 years of the program after it placed additional emphasis on tobacco cessation. From July 1, 2008, to June 30, 2011, fewer than 3% of all WISEWOMAN participants who smoked received a tobacco-cessation counseling LSI. From July 1, 2011, to June 30, 2012, nearly 37% of smokers received a tobacco-cessation counseling LSI. In the final program year (July 1, 2012, to June 30, 2013), 40% of smokers received a tobacco-cessation counseling LSI.
Since 2008, program procedures have included community-based tobacco-cessation program contacts for WISEWOMAN participants. Although there is significant variation in the availability of such programs, many women have benefited from them. From July 1, 2008, to June 30, 2013, the 15,926 screening visits with current smokers were linked to at least one community-based tobacco-cessation program, or 29% of all smokers in the program (Table 3).
The sustained focus on tobacco cessation over the years has allowed the WISEWOMAN program to observe a 15% smoking-cessation rate among smokers at baseline screening who returned for a rescreening visit. The WISEWOMAN program defined cessation among its participants as those who self-identified as smokers at the baseline screening visit and as nonsmokers at the last rescreening visit. Rescreening visits typically occurred every 12 to 18 months after the baseline screening.
Smoking-cessation rates varied by participants' race and ethnicity. WISEWOMAN Hispanic participants had the highest cessation rate; approximately 34% of Hispanic women who were once smokers quit by their last rescreening visit. On the other hand, non-Hispanic white women had the lowest cessation rate, with only about 13% quitting by their last rescreening visit.
Odds ratios using logistic regression models were used to determine what attributes increased the likelihood that a woman who was a smoker at her baseline clinic screening visit would become a nonsmoker at her last rescreening visit. Race and ethnicity had a statistically significant effect on the odds of quitting smoking. Hispanic women had the greatest odds for becoming nonsmokers at their last rescreening visit (OR=3.32, p<0.0001, 95% CI: 2.80–3.94) when compared to non-Hispanic white women. Other racial and ethnic minorities followed the same trend line when compared to non-Hispanic white women. Non-Hispanic American Indian/Alaskan Natives (OR=1.53, p<0.0001, 95% CI: 1.27–1.85), non-Hispanic blacks (OR=1.36, p=0.0002, 95% CI: 1.16–1.60), and non-Hispanic Asian/Pacific Islanders (OR=3.69, p<0.0001, 95% CI: 1.94–7.00) were more likely to become nonsmokers than were non-Hispanic white women. The CI for non-Hispanic Asian/Pacific Islanders (4%) is wide, which can be explained by the variance in the small sample size of smokers in this group (Table 4).
Reference for race/ethnicity: non-Hispanic white; reference for number of rescreening visits: OR increases per extra visit; reference for age at baseline: a 1-year age increase from one woman compared to another similar woman.
CI, confidence interval; OR, odds ratio.
Age was statistically significant in quitting smoking; older women had a slightly higher OR of becoming nonsmokers (OR=1.01, p=0.0033; 95% CI: 1.00–1.02). Furthermore, there was a statistically significant relationship between the number of rescreening visits and odds of smoking cessation. For every additional rescreening visit a woman attended, her odds of becoming a nonsmoker increased by 1.18 (p=0.0033, 95% CI: 1.06–1.31) (Table 4). This supports program guidance to maintain contact with women and to emphasize the importance of returning for a rescreening.
Discussion
This program update is reflective of a practice program rather than a research program; therefore, we are limited to reporting changes in the population who chose to continue in the program and return for rescreenings. These participants were enrolled in any of the 21 state and tribal WISEWOMAN programs. Therefore, our analyses are limited to the enrolled population. Some of the data collected were self-reported values and were reliant on the accuracy of those responses. This is especially true for smoking status. In addition, data validation was done at the program level, which may have resulted in missing and/or excluded data for which the cause is unknown. Further, as this was a 5-year program, some women may have aged out of or lost eligibility for the program. These situations limited the opportunities to capture rescreening-visit data. Finally, WISEWOMAN participants who quit smoking may have been more highly motivated than other WISEWOMAN participants; thus, the cessation rate may be lower than reported.
Conclusions
In addition to affecting health behavior in individuals, the WISEWOMAN program is an example of the synergy achieved when individual care, clinical processes, and community environmental changes occur. As a result, long-term changes occur in clinical policies and procedures, professional development for healthcare providers, and community norms that affect the larger population served by these healthcare providers.
Final reports from programs indicate successes at many different levels in reducing tobacco use across all 21 programs and over the 5-year funding, with the overall data showing increased quitline referrals and decreased smoking rates among WISEWOMAN participants. The program, based on 5 years of data, has exhibited a 15% smoking-cessation rate among women who were smokers at their baseline visit and quit at their last rescreening visit. The unique combination of direct individual health services and population-based strategies has contributed to this reduction in smoking prevalence and has had a positive impact on women's cardiovascular health over the past 5-year cooperative agreement.
The WISEWOMAN program began a new 4-year funding cycle on July 1, 2013; WISEWOMAN programs will implement a number of program strategies to build on the achievements from prior years. These strategies include gathering information to monitor and evaluate the tobacco use of participants and their exposure to secondhand smoke and developing or enhancing partnerships with state tobacco-control programs to reduce tobacco use and eliminate exposure to secondhand smoke. WISEWOMAN program guidance will continue to address cessation counseling and referral to appropriate cessation resources. In addition, programs will work closely with partners in their state tobacco-control program and at the state quitline to monitor participants' use of quitline services. Programs will continue to refer smokers to the most appropriate cessation services available. Strong emphasis will continue on working closely with healthcare providers to ensure that all clinic patients are referred to smoking-cessation services. WISEWOMAN will continue its successful efforts to reduce smoking rates among program participants and to contribute to the reduction of CVD risk in uninsured and underserved women.
Footnotes
Acknowledgments
We would like to express our appreciation to the WISEWOMAN programs in Pennsylvania and at SEARHC for their assistance in highlighting their program activities.
Author Disclosure Statement
The authors have no conflicts of interest to report.