
Abstract
Background:
Polycystic ovary syndrome (PCOS) affects 6%–21% of women. PCOS is the primary cause of anovulatory infertility, with major health and economic costs, yet we are unaware of any community-based, natural history studies on fertility and fertility treatments published to date. We aim to compare infertility, fertility treatment use, and relationship to body mass index (BMI) in women reporting PCOS to women not reporting PCOS in a community-based population.
Methods:
This is a cross-sectional analysis of a longitudinal cohort study, the Australian Longitudinal Study on Women's Health (ALSWH). For the ALSWH, women from the general community were randomly selected from the national public insurance database. Mailed survey data were collected at multiple time points. At survey 4, there were 9145 respondents aged 28–33 years. Of 8612 women with known PCOS status, 478 women reported having PCOS. Information regarding fertility status was available for 4856 women. This was the subgroup used in this analysis. The main outcomes measures are self-reported PCOS status, BMI, infertility, and use of fertility therapies including ovulation induction and in vitro fertilization (IVF). Logistic regression was used to examine factors associated with infertility and use of fertility treatment.
Results:
Self-reported PCOS prevalence was 5.8% (95% confidence interval [CI]: 5.3%–6.4%). Infertility was noted by 72% of 309 women reporting PCOS, compared with 16% of 4547 women not reporting PCOS (p<0.001). Infertility was 15-fold higher in women reporting PCOS (adjusted odds ratio 14.9, 95% CI 10.9–20.3), independent of BMI. Of women reporting infertility, there was greater use of fertility hormone treatment, (62%, n=116 vs. 33%, n=162, p<0.001) in women reporting PCOS; however, IVF use was similar.
Conclusions:
In this community-based cohort of women, infertility and use of fertility hormone treatment was significantly higher in women reporting PCOS. Considering the prevalence of PCOS and the health and economic burden of infertility, strategies to optimize fertility are important.
Introduction
P
Women with PCOS have higher rates of obesity and central adiposity compared to women without PCOS. 12,13 A recent systematic review and meta-analysis of 21 studies reported a pooled prevalence of 61% (range between 6% and 100%) for overweight or obesity in women with PCOS compared with controls, with considerable heterogeneity between studies. 14 Both the prevalence and clinical expression of PCOS are strongly influenced by weight. 13 –17 Obesity exacerbates the reproductive and metabolic features of PCOS, 18,19 worsens infertility independent of PCOS 20 –22 and decreases response to assisted reproductive technology (ART). 23 There are limited data exploring the impact of body mass index (BMI) on fertility in community-recruited PCOS populations. Therefore, it is important to explore the interaction between PCOS, BMI, and fertility and treatment outcomes.
While infertility is well described in PCOS, we were unable to find any published data examining the natural history data on infertility prevalence or on use of fertility treatment in PCOS in community-based Caucasian populations. Most infertility and PCOS data is based on selected populations managed in hospital or fertility clinics. A study by Wild et al. retrospectively followed a cohort of 786 women from the United Kingdom with PCOS diagnosed over 30 years ago. The women with PCOS were identified from hospital records and compared with 1060 women without PCOS. In this selected population, using macroscopic or microscopic evidence of polycystic ovaries with or without ovarian dysfunction, 66% of women reported infertility, 24% had ovulation induction with clomiphene citrate, and 17.5% had persisting involuntary infertility, compared with 6%, 1%, and 1.3% of those without PCOS. 24 BMI three decades ago was lower overall and there was no analysis of an interaction between PCOS, BMI, and infertility in the study. 24
A recent Swedish birth register analysis reported on pregnancy outcomes in singleton pregnancies in women with PCOS, noting increased nulliparity compared with women without PCOS, despite higher maternal age and increased use of ART (13.7% compared with 1.5% of women without PCOS). 25 There is limited data on the natural history of fertility in PCOS and the likely health and economic burden of PCOS, infertility, and fertility therapies. Greater insight is needed into the natural history of fertility and the key predictors of infertility, including the impact of BMI and the use of fertility hormones and in-vitro fertilization (IVF) in PCOS.
Using the large, prospective, community-based Australian Longitudinal Study on Women's Health (ALSWH), we aimed to explore self-reported PCOS status, infertility (defined as trying unsuccessfully for 12 or more months to become pregnant), use of fertility hormones, and IVF and to examine the relationships between infertility, PCOS status, and BMI.
Methods
The ALSWH collected mailed survey data from three age cohorts of Australian women in 1996 and subsequently on five separate occasions. The ALSWH primary aims were to examine the relationships between biological, psychological, social, lifestyle factors, women's physical and mental health, and their use of and satisfaction with health care services.
26,27
Women were randomly selected from the national health insurance scheme (Medicare) database, which includes almost all people who are permanent residents of Australia.
27
Women were recruited nationally with intentional oversampling from rural and remote areas.
27
Further details of the methods used by the ALSWH and characteristics of the sample have been reported elsewhere and are available at
For the purposes of this study, data collected from the ALSWH survey 4 in 2006 of women born in 1973–1978 (n=14,779 at survey one, age 18–23) were utilized. With intensive tracking procedures and follow-up, retention of baseline participants was 62% for survey 4 (n=9145). Data were analyzed from respondents to survey 4 (2006), aged 28–33, who responded to the question on PCOS and had fertility data available (n=4856) (Fig. 1). Survey 4 was chosen for this analysis, as this was the first survey where information about PCOS was collected.
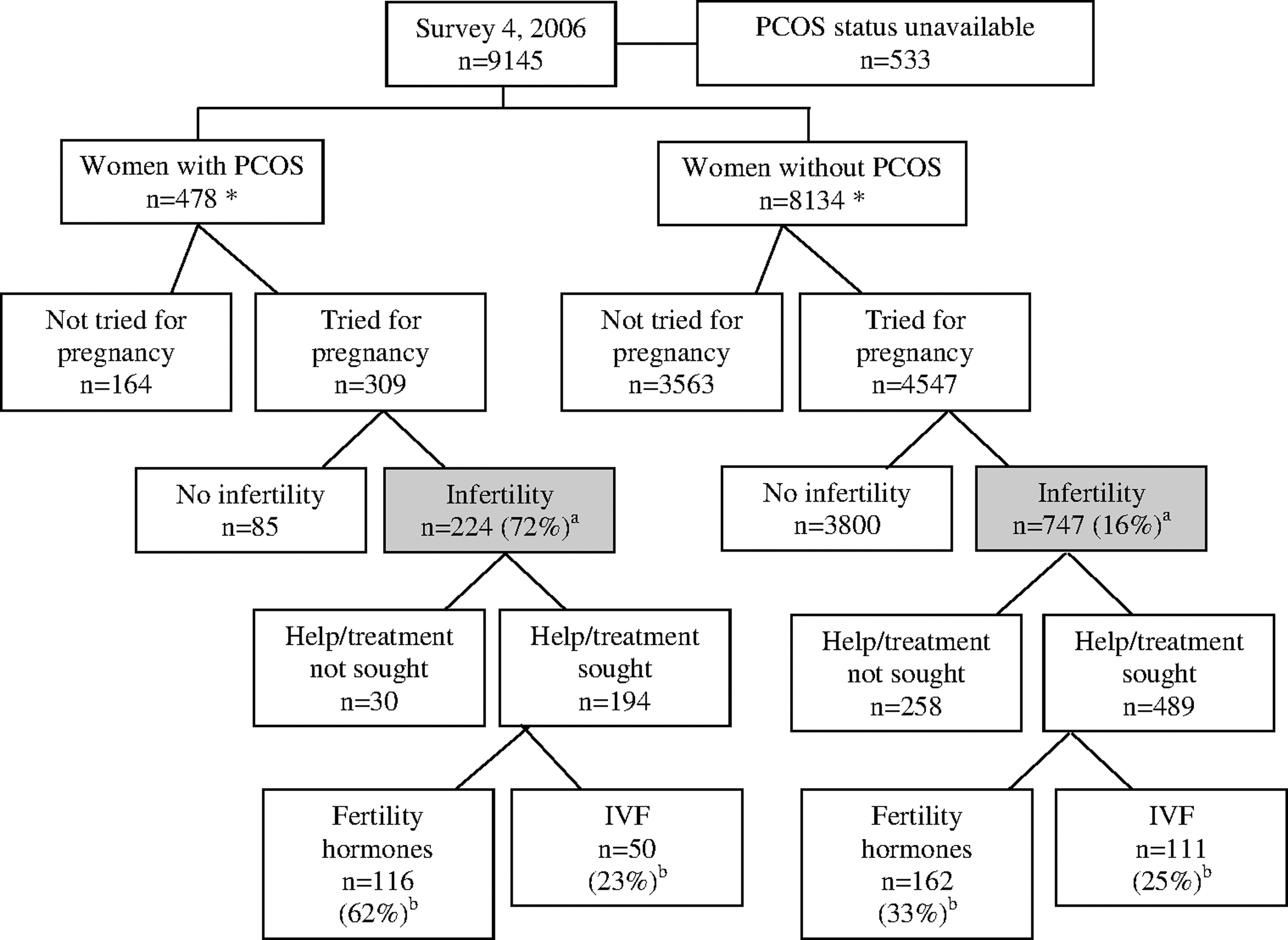
Consort diagram. *No data available regarding fertility status for n=5 women with polycystic ovary syndrome (PCOS) and 24 women without PCOS. aOf women who have tried for pregnancy. bOf women reporting infertility who have sought help or treatment. IVF, in vitro fertilization.
Outcome variables assessed from survey 4
(1) Infertility. Women were asked if they or their partner (current or previous) had ever had problems with fertility (defined as trying unsuccessfully for 12 or more months to become pregnant). Women who chose the response “no, never tried to get pregnant” were classified as having unknown fertility, and the remainder of the women were classified as having known fertility. Of those women who had known fertility, those who chose the response “no, had no problem with fertility” were classified as not experiencing infertility and those who chose the response “yes, but have not sought help/treatment” or the response “yes, and have sought help/treatment” were classified as having experienced infertility.
(2) Fertility treatment. Women were asked if they were currently using or had previously required fertility hormone treatment, which specified the use of the fertility drug Clomid. However, it did not specify the use of other fertility drugs such as metformin or gonadotrophins. Women were also asked if they were currently using or had previously required IVF.
(3) Irregular cycles. Women were asked if they had irregular menstrual cycles in the previous 12 months. Women could respond with one of the following responses: no, rarely, sometimes, or often. Women who gave the response “often” were considered to have irregular menstrual cycles.
Explanatory variables
PCOS
Women were asked if they had been diagnosed or treated for PCOS in the previous 3 years. Individual clinical diagnostic features of PCOS were not included in the surveys, except for menstrual cycle regularity. Self-reported PCOS shows high correlation with irregular cycles in this cohort, as reported previously. 13
BMI
BMI was calculated from self-reported height and weight and classified as healthy weight, BMI <25 kg/m2; overweight, BMI 25.0–29.9 kg/m2; and obese, BMI ≥30 kg/m2 (using the World Health Organization criteria 30 ).
T2DM
Women were asked if they had been diagnosed with or treated for T2DM in the last 3 years. Women were considered to have a history of T2DM if they responded “yes” in survey 4.
Hypertension
Women were asked if they had been diagnosed with or treated for hypertension (outside of pregnancy) in the last 3 years. Women were considered to have a history of hypertension if they responded “yes” in survey 4.
Other explanatory variables
Other variables included education status, main occupation, household income, smoking status, and area of residence (Table 1).
All estimates are adjusted for area of residence to account for over sampling of women from rural and remote areas.
Values are reported as mean±standard error of the mean (SEM) or proportions.
BMI, body mass index; PCOS, polycystic ovary syndrome.
Statistical analysis
Continuous explanatory variables are summarized as means with standard error. Categorical explanatory variables are reported as percentages. Differences in variables at baseline between subgroups of the study population were tested using survey weighted univariable regression or the chi-squared test, as appropriate. Cross tabulation was used to examine the relation between categorical explanatory variables and self-reported PCOS. To assess the relationships between PCOS and BMI on infertility and fertility treatment at survey 4, logistic regression analyses were performed, adjusting for potential confounding covariates including age, T2DM, hypertension, household income, occupation, qualification, and smoking status. The selection of variables was based on identifying all measured clinical variables of known or suspected prognostic importance for the outcome of interest (and/or exhibiting a p value of less than 0.1 on univariate analysis). To further explore these relationships, the interaction between PCOS and BMI (as a continuous measurement) was examined for each outcome of interest. Given the deliberate oversampling from rural and remote areas, all statistical analyses included survey weighting for area of residence. All p values were calculated from two-tailed tests of statistical significance with a type-1 error rate of 5%. All analyses were performed using Stata software version 11.0 (StataCorp).
Ethical approval
The Human Research Ethics Committees of the University of Newcastle and the University of Queensland approved the study methods.
Results
Prevalence of self-reported PCOS and relationship to PCOS symptoms from survey 4
At survey 4, as previously reported, 478 of the 8612 women in this cohort reported a history of PCOS, with a prevalence of 5.8% (95% confidence interval [95% CI]: 5.3%–6.4%). 13 Accuracy of self-reported PCOS status was supported by the close relationship between irregular menstrual cycles and PCOS status (11-fold likelihood of PCOS) in women who were not pregnant or on the oral contraceptive pill as we have previously published from this cohort. 13
Demographic data across a cross-sectional cohort
In the subgroup of women with known fertility, there were no significant differences between women who reported PCOS and those who did not report PCOS with regard to the main demographic variables (Table 1). Overall, the mean BMI was significantly higher in women reporting PCOS as we have previously published from this cohort (Table 1). 13
Fertility status
Analysis of fertility status was completed for the subgroup of 4856 who had previously attempted to conceive and hence were deemed to have “known fertility status” (Fig. 1 and Fig. 2A). A greater proportion of women reporting PCOS had tried to conceive (64%, n=309) compared with those not reporting PCOS (54%, n=4547) (p<0.001) (Fig. 2A). Overall, of those who had tried to conceive, 20% of women reported infertility. Women reporting PCOS were more likely to report infertility (72%, n=224) compared to women not reporting PCOS (16%, n=747) (p<0.001) (Fig. 2B). Of the 513 women reporting “often having irregular cycles,” the prevalence of infertility was greater in women with PCOS who reported “often having irregular cycles” (79%, n=104/130) compared to women without PCOS (34%, n=124/383) (p<0.001).

Fertility status, infertility, fertility hormone use, and IVF use by PCOS status and body mass index (BMI) category.
Fertility treatments use
Among the 971 women reporting infertility, women reporting PCOS were more likely to have sought help or treatment (87%, n=194) compared to women not reporting PCOS (66%, n=489) (p<0.001) (Fig. 1). Of the women with PCOS reporting infertility who sought help or treatment, more women with PCOS (65%, n=123) reported use of fertility treatment including ovulation induction or IVF compared to women without PCOS (42%, n=202) (p<0.001). Specifically, of the women reporting infertility, seeking help or treatment, women reporting PCOS were more likely to report use of fertility hormones (62%, n=116) compared with women not reporting PCOS (33%, n=162), (p<0.001). IVF use was not different between women with (25%, n=50) and without PCOS (23%, n=111), (p=0.73) (Fig. 2C).
Relationship between PCOS, BMI, infertility, and fertility treatment
Among women who had known fertility status, mean BMI was significantly higher in women reporting PCOS (27.9±0.4 kg/m2 compared with 25.1±0.1 kg/m2 in women not reporting PCOS, p<0.001) (Table 1). Both infertility and fertility hormone use were higher in the PCOS group within each BMI category (healthy weight, overweight, and obese) (Fig. 2D, E). However, use of IVF was similar between the PCOS and non-PCOS groups within each BMI category (Fig. 2F).
Contribution of PCOS to infertility treatment burden
Overall, of the 325 women reporting a history of infertility and use of fertility treatment, 123 women reported PCOS (40%). The majority of women with and without PCOS who reported infertility reported having one or more live born children by survey 4 (60%, n=135/224 and 61%, n=472/746 respectively, p=0.78). Of these, more women with PCOS (63%, n=81) reported fertility treatment use compared to women without PCOS (27%, n=124) (p<0.001).
Multivariable analyses of factors associated with infertility and use of fertility treatment
Multivariable analysis of factors associated with infertility was completed for the subgroup of 4856 who had previously attempted to conceive and hence were deemed to have “known fertility status” (Figs. 1, 2A). PCOS was associated with infertility when adjusted for the other covariates (adjusted odds ratio [OR] 14.9, 95% CI 10.9–20.3) (Table 2). BMI was not associated with infertility overall when adjusted for the other covariates (adjusted OR 1.01, 95% CI 0.99–1.03) or when examining within BMI categories (Table 2). There was no significant interaction between PCOS and BMI observed for this outcome (p=0.34).
Analysis included survey weighting for area of residence given deliberate oversampling of women from rural and remote areas.
Association of explanatory variables to outcome variable derived from odds ratio and 95% confidence interval (95% CI).
Reference category.
The results presented for the categorical variable for BMI are from a separate analysis that did not include BMI as a continuous variable but included all the other variables presented above.
IVF, in vitro fertilization.
Multivariable analysis of factors associated with fertility hormone use was completed for the subgroup who reported infertility. PCOS and BMI were both associated with the use of fertility hormones (adjusted OR 5.3, 95% CI 3.6–7.7 and adjusted OR 0.96, 95% CI 0.94–0.99 respectively). BMI was associated with reduced use of fertility hormones in the obese group (adjusted OR 0.4, 95% CI 0.3–0.7) (Table 2). There was no significant interaction between PCOS and BMI observed for fertility hormone use (p=0.44).
Multivariable analysis of factors associated with IVF use was completed for the subgroup who reported infertility. PCOS and BMI were both associated with the use of IVF (adjusted OR 2.0, 95% CI 1.2–3.2 and adjusted OR 0.9, 95% CI 0.9–0.97). BMI was associated with reduced use of IVF in the obese group (adjusted OR 0.4, 95% CI 0.2-–-0.7) (Table 2). There was no significant interaction between PCOS and BMI observed for IVF use (p=0.41).
The above multivariable regression analysis was repeated using “often having irregular cycles” as an explanatory variable, rather than reported PCOS status. Results were similar (data not shown). Again, there was no interaction with irregular cycles and BMI in this analysis.
Discussion
The current study examines the natural reproductive history of women reporting PCOS compared to women not reporting PCOS in a large community-based cohort of women aged 28–33 years. The study focuses on infertility and use of fertility treatments. Just over half of all women had tried to conceive, although this was more frequent in women with PCOS (64% vs. 54%, p<0.001). The overall proportion of women who had tried to conceive and reported infertility was high at 20%, and PCOS was associated with a 15-fold increased risk of infertility, independent of BMI. Of those who were infertile, more women with PCOS sought help or treatment for infertility (87% vs. 66%) and of these, women with PCOS were more likely to undergo fertility hormone treatment (62% vs. 33%), but not IVF. Despite only 5.8% of women having PCOS, they comprised a significant proportion (40%) of all women who received infertility treatment, indicating infertility treatment is a high burden for these women.
We were unable to find any large community-based studies exploring awareness, prevalence, and treatment of infertility in PCOS, despite infertility being a known clinical complication of PCOS. There are two studies that report on hospital-based recruits 24,31 compared with community controls and one based on a birth register. 25 A long-term follow-up of a selected cohort of women with PCOS identified retrospectively from hospital records three decades ago was based primarily on ovarian histology with or without ovarian dysfunction and did not use hyperandrogenism. 24 Similar to our study, more women with PCOS had infertility at baseline (66%) 24 compared with community controls. This cohort was not representative of modern PCOS diagnostic criteria or current BMI, and ART was inferior and access more limited for this historic population. 24
Another long-term follow-up in a selective hospital group of Swedish women compared 91 women with PCOS to 87 population-based controls. 31 Most women with PCOS had attempted to conceive (91.2%), had sought help for infertility (75.9%), and reported having treatment (67.5%). 31 More recently, a Swedish birth register analysis assessing singleton pregnancy outcomes noted increased use of ART in women with PCOS than in women without PCOS (13.7% vs. 1.5%). 25 In this context, we advance knowledge with a community-based study of young women who are representative of current trends in BMI and ART use. Here, 72% of women with PCOS reported infertility, the majority of whom sought medical advice. This attests to the high public health burden and cost associated with PCOS.
Oligo- or anovulation may be experienced by up to 70% to 80% of women with PCOS, 6 and PCOS is the leading cause of anovulatory infertility. 32 BMI is higher in women with PCOS 13 and is a known independent risk factor for infertility. 20 –22 However, the prevalence and the impact of BMI on infertility in a community-recruited population of women with PCOS remains unclear, as most related studies have been conducted in selected clinic populations. It has been previously estimated that 50% of women diagnosed with PCOS will actively seek help or treatment related to infertility, but again, data is limited. 33 The rate of use of fertility treatments is high in Australia, with the number of ART cycles initiated in Australia and New Zealand in 2009 increasing by 48% from 2005; 34 however, the proportion of these that have PCOS is unknown. International data suggest that PCOS accounts for 17% of couples attending infertility units in Poland based on self-reported data on questionnaire from those presenting at an infertility center. 35 In the current large community-based study, 40% of all women reporting a history of infertility and use of fertility treatment had a history of PCOS. These data suggest that PCOS strongly contributes to overall use of costly fertility treatment and presents a considerable health and economic burden.
In the current study, BMI was associated with infertility on univariable regression; however, BMI was not associated with infertility in our multivariable regression model, which included PCOS. PCOS had a strong independent association with infertility that overwhelmed any impact of BMI, and there was no interaction between PCOS and BMI. This is not consistent with current understanding that higher BMI per se is a key cause of infertility. 20 –22 We have previously shown that insulin resistance underpins PCOS independent of obesity and that lean women with PCOS have equivalent insulin resistance to obese non-PCOS women. 36 Here we hypothesize that this insulin resistance drives infertility in PCOS independent of BMI. It is important to note that weight loss in overweight women with PCOS has been shown to increase fertility and remains recommended first line treatment for infertility in this group. 37,38 The mean BMI in the cohort here who reported infertility was 27.9±0.4 kg/m2 compared with 25.1±0.1 kg/m2 in the cohort who did not report infertility. The current study had less than 20% of those with known fertility who were obese with a BMI greater than 30, and this may partly account for the lack of observed association found between BMI and infertility. Finally, BMI was associated with less use of fertility treatments in obese women. Although there are no regulations governing fertility treatment (ovulation induction or IVF) in women with BMI >35kg/m2 in Australia, there are current clinical guidelines suggesting that a BMI ≥35 should be considered a contraindication to fertility treatment, and our findings suggest that clinical practice may be consistent with these guidelines. 38,39
Limitations of this study include the inability to determine timing of PCOS diagnosis and infertility. The PCOS phenotype of each woman is not known, and therefore the exact relationship of specific PCOS features to infertility or fertility treatment is not known. We acknowledge that women presenting with infertility are more likely to be screened for and diagnosed with PCOS. It is not possible to know from this data whether women were diagnosed with PCOS as they had difficulty trying to conceive or whether they were previously diagnosed with PCOS. If the former applies, there is some potential for selection bias, as women with a history of infertility are more likely to be investigated for and diagnosed with PCOS. This data is self-reported, although this is generic in large prospective community-based cohort studies over multiple time points and self-reported PCOS correlated with irregular menstrual cycles and prevalence rates were consistent with Australian community-based PCOS prevalence rates. 1 Furthermore, recent analyses from this observational study have contributed to the growing body of evidence suggesting that such biases are insufficient to preclude meaningful longitudinal analyses. 28 Finally, BMI from survey 4 has been used for analysis but may not correspond to the BMI at the time when a woman had infertility. However, in this population, women with PCOS have higher weight than those not reporting PCOS across the 14 years of the study follow-up, as published previously. 13
The strengths of the current study include the provision of data from a large, unselected community community-based cohort of young women with high baseline and ongoing participation rates; the use of prospective data with limited information bias; and a focus on diagnosed PCOS, with all women captured irrespective of fertility, pregnancy, or birth outcomes. A comparison of baseline survey participants to women in the same age range from the 1996 Australian census showed that the ALSWH participants were representative of the general population. 27
In this community-based, unselected population, we found that women with PCOS were more likely to have tried to conceive, to report infertility and report use of fertility hormone treatment. PCOS appears to be the primary determinant of infertility, irrespective of BMI. Strategies aimed at optimizing fertility in women with PCOS are important, especially given the significant health and economic burden related to infertility and fertility treatment use. Educating women about potential fertility challenges is vital so that women can make informed decisions regarding family planning, earlier family initiation, and engagement in healthy lifestyle practices.
Footnotes
Acknowledgments
The research on which this paper is based was conducted as part of the Australian Longitudinal Study on Women's Health undertaken by The University of Newcastle and The University of Queensland. We are grateful to the Australian Government Department of Health and Ageing for funding and to the women who provided the survey data.
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors. Dr. Joham is an National Health and Medical Research Council (NHMRC) postgraduate scholarship holder, Prof. Teede and Dr. Boyle are NHMRC postdoctoral research fellows, and Associate Prof. Zoungas is a National Heart Foundation (NHF) postdoctoral research fellow. The Australian Longitudinal Study on Women's Health is funded by the Australian Government Department of Health and Ageing.
Author Disclosure Statement
No competing financial interests exist.