
Abstract
Background:
The available evidence about the effect of gender and/or sex on mortality differences is contradictory. Our aim is to assess the impact of gender on the access to reperfusion therapy in patients with acute coronary syndrome with ST-segment elevation (STEMI), and secondly, to analyze the effect of delay on the differences with regard to hospital mortality.
Methods:
A retrospective cohort study was conducted among consecutive patients with STEMI included in the ARIAM-SEMICYUC registry (2010–2013).
Results:
A total of 4816 patients were included (22.09% women). Women were older, presented with longer patient delay (90 vs. 75 minutes, p=0.0066), higher risk profile (GRACE>140: 75.1% vs. 56.05%, p<0.0001), and received less reperfusion therapy (68.8% vs. 74.7%, p<0.0001) with longer total reperfusion time (307 vs. 240 minutes, p<0.0001). Women received less thrombolysis (24.53% vs. 29.98%, p<0.0001) and longer door-to-needle time (85 vs. 70 minutes, p 0.0023). We found no differences regarding primary percutaneous coronary intervention or door-to-balloon time. Women also had higher hospital mortality (crude odds ratio 2.54, 95% confidence interval 1.99–3.26, p<0.0001), which persisted after controlling the effect of patient delay, age, risk (GRACE), and reperfusion (adjusted odds ratio 1.43, 95% confidence interval 1.0–2.06, p=0.0492). Using TIMI or Killip risk scores as risk estimates yielded nonsignificant results.
Conclusions:
Compared with men, women with STEMI have worse access to reperfusion and higher hospital mortality. The impact of the differences in accessibility on mortality gap remains uncertain.
Introduction
M
The available evidence about the effect of gender and/or sex on mortality differences is contradictory. 7,8 This may be due to the weight attributable to biological differences, age, 8,9 different clinical presentation, 10 or inequity problems due to underutilization of evidence-based treatments. 4,5,11 Women also show consistently longer delay before reperfusion therapy. 12 It is not known exactly whether this is a question of sex or gender. The term “sex” includes features biologically determined by genotype. The term “gender” refers to social roles (the network of attitudes, values, and behaviors that differentiates men from women). Without ignoring the biological differences, the gender approach allows us to propose the research questions in terms of disparity or inequality.
These differences in the prognosis of acute coronary syndrome according to sex/gender have been observed in Western countries 13 including Spain. 14 This study tries to quantify differences in accessibility to the Spanish health system among women with STEMI compared with males and to analyze the effect of the delay and its determinants on the differences in mortality.
Methods
Study population and data collection
We conducted a retrospective cohort analysis based on the ARIAM-SEMICYUC registry (in-hospital, national level) of consecutive patients over 18 years of age with suspected STEMI, admitted within 48 hours of the episode to coronary or intensive care units in Spain during the period 2010–2013. The study is presented following the STROBE (STrengthening the Reporting of OBservational studies in Epidemiology) recommendations. 15
The registry involves 60 public and private hospitals in Spain. Each year over a period of 3 months, the participating centers anonymously communicate patient data. Data are entered in the registry through a Web application.
The follow-up period extended until hospital discharge. The data are kept anonymous, and the database is built with Web technology adjusted to the rules of data protection in Spain.
Definitions and study variables
The exposure variable considered was gender. The endpoints of the study were total reperfusion time—as a proxy to accessibility—and hospital mortality. Other response variables considered were reperfusion therapy, delay intervals (patient delay and health system delay) and both percutaneous (primary percutaneous coronary intervention [PCI]) and pharmacological (thrombolysis) coronary reperfusion. Patient delay was considered as the time between onset of symptoms and first medical contact (FMC). System delay was considered as the interval from the FMC to the onset of reperfusion therapy. The total reperfusion time was defined as the period between the onset of symptoms and the passage of the guide to the culprit lesion or the time of administration of thrombolysis. 16 This period was right-censored to 720 minutes (12 hours).
The potential confounding variables were age; patient history (angina, recent severe angina, previous myocardial infarction, known coronary artery disease, history of bleeding, stroke, chronic obstructive pulmonary disease, heart failure, peripheral artery disease and chronic renal failure); coronary risk factors (smoking, hypertension, family history, dyslipidemia, diabetes mellitus, and obesity); the characteristics of the episode, both electrocardiographic and clinical; initial severity scores (thrombolysis in myocardial infarction [TIMI], Killip, and Global Registry of Acute Coronary Events [GRACE] scores); and CRUSADE hemorrhagic score. Definitions and encoding of the registry variables are available on the SEMICYUC website (
Statistical methods
Categorical variables were summarized as proportions and continuous variables as medians with interquartile range. The association between categorical variables was tested by chi-square test. Nonparametric tests (the Mann-Whitney U test for two groups or the Kruskal-Wallis test for three or more groups) were applied to evaluate differences for continuous variables. For ordinal variables we used a chi-square test for linear trend. For access time analysis we used the Wilcoxon test, which gives more weight to early differences in time than the log rank test. Survival analyses (Kaplan-Meier) were used to compare total reperfusion time between men and women.
To analyze the association between hospital mortality and gender, we designed a causal model using logistic regression to control the effect of patient delay and other potentially involved variables, such as age, reperfusion, and the severity of patients on admission (GRACE score). Among the risk scores, we chose GRACE as a determinant of risk because it is derived from a large unbiased multinational registry to predict in-hospital patient mortality. In clinical practice, GRACE risk score provides a good ability to assess the risk for death. The components of the GRACE risk score are age, heart rate, systolic blood pressure, Killip class, cardiac arrest, ST-segment deviation, serum creatinine, and initial cardiac biomarker status. Sex was considered in the development of this score and was not a statistically significant predictor associated with hospital mortality. 19
On the other hand, TIMI risk score is derived from databases from clinical trials, which tend to exclude high-risk patients. Furthermore, the determinants of mortality were developed in populations treated with thrombolysis, 18 so TIMI was not considered fully representative of the clinical spectrum of patients in daily practice, reperfused mainly by primary PCI. An additional reason for not choosing a risk score based on data from clinical trials is the underrepresentation of women in clinical trials. 20
In order to test the diagnostic accuracy of the scores in our cohort, we calculated receiver operating characteristic (ROC) curves and area under the ROC curve (AUC).
The statistical tests were two-sided, with a significance level (type 1 error) of 5%.
All analyses were performed with the use of the StatsDirect medical statistics software, version 2.8.0 (Cheshire, UK).
Results
A total of 4816 patients with acute coronary syndrome with ST elevation (STEMI) were included. Of these, 1064 patients (22.1%) were women. Demographic and cardiovascular risk profiles are shown in Table 1. Women with STEMI were older (74 vs. 62 years, p<0.0001), with more comorbidity: hypertension (67.2% vs. 50.2%, p<0.0001), diabetes (25.6% vs. 20.8%, p=0.0033), and obesity with body mass index >30 (25.2% vs. 21.4%, p=0.0124). They also had more history of congestive heart failure than did men with STEMI (3.2% vs. 1.5%, p=0.0003).
Values are numbers (percentage) unless stated otherwise.
COPD, chronic obstructive pulmonary disease; IQR, interquartile range; MI, myocardial infarction.
With regard to the characteristics of the episode (Table 2), women with STEMI had more painless or atypical symptoms (14.2% vs. 11.8%, p=0.035), less obvious electrocardiographic changes (23.3% vs. 19 7%, p=0.036), and greater ischemic and hemorrhagic risk (measured by the GRACE and CRUSADE scores).
Values are numbers (percentages).
Delays are presented in minutes, as medians and interquartile ranges (IQR).
CRUSADE, Can Rapid risk stratification of Unstable angina patients Suppress ADverse outcomes with Early implementation of the American College of Cardiology/American Heart Association guidelines; ECG, electrocardiogram; FMC, first medical contact; GRACE, Global Registry of Acute Coronary Events; KK, Killip-Kimball; LBBB, left bundle branch block; PCI, percutaneous coronary intervention; TIMI, thrombolysis in myocardial infarction.
No differences were found in terms of access to health care. However, once the system was contacted, transport resources mobilized for women were not as often fully equipped ambulances with personnel trained to perform and interpret a 12-lead electrocardiogram (34.7% vs. 38.4%, p<0.0001) as they were for men (Table 2).
Despite having a greater risk of the episode, women experienced a longer delay from the onset of symptoms to FMC (90 vs. 75 minutes, p=0.0066), especially those who contacted the health care system through the hospital emergency department (120 vs. 107 minutes, p=0.0371) or primary care emergency department (104 minutes vs. 77 minutes, p=0.0028).
Adjunctive antiplatelet therapy (acetylsalicylic acid and thienopyridines) was administered equally to men and women in both primary care and hospital emergency departments (Table 3).
Values are given as numbers (percentage).
Includes reperfusion treated patients in the first 12 hours, either by thrombolysis or primary PCI.
ASA, acetylsalicylic acid; ED, emergency department.
The overall percentage of reperfusion-treated patients (Table 3) was significantly lower among women (68.8% vs. 74.7%, p<0.0001). With regard to the methods of reperfusion, women received less thrombolysis (24.5% vs. 29.9%, p<0.0001) with a longer door-to-needle time (85 vs. 70 minutes, p=0.0023). However, no differences were observed regarding reperfusion by primary PCI (44.22% vs. 44.69%) (Table 3). In total reperfusion time (considered as time from the onset of symptoms to reperfusion treatment) was longer in women (347 vs. 255 minutes, p<0.0001), as shown in Figure 1, with a hazard ratio (HR) of 0.79 (95% confidence interval [CI] 0.73–0,87, p<0.0001).
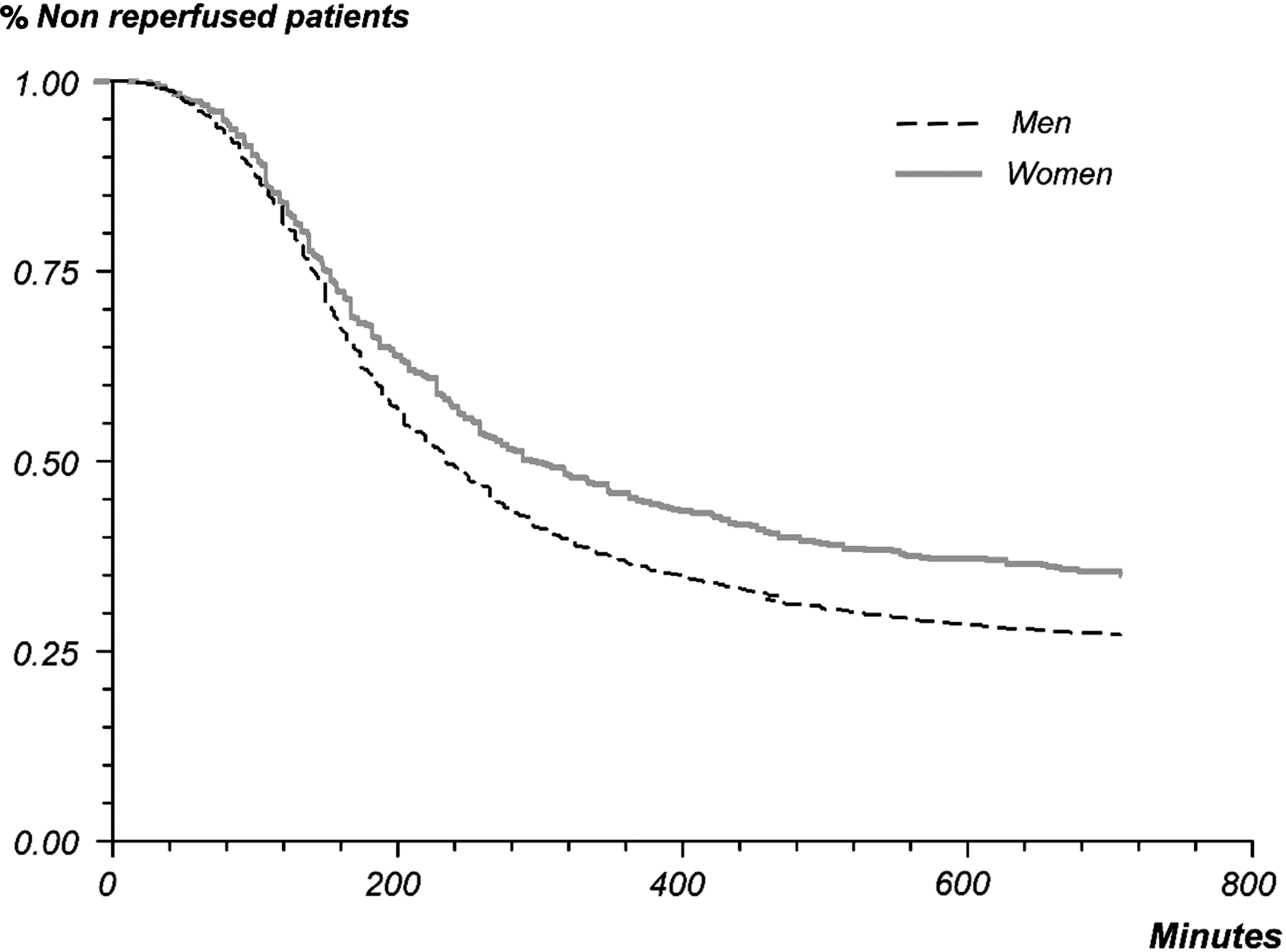
Time from symptoms to reperfusion therapy: Survival analysis.
Considering both methods separately, no differences were found in symptoms-to-balloon delay (HR 0.94 95% CI 0.84–1.06, p=0.3455) between men and women treated by PCI. However, differences remain for thrombolytic therapy (symptoms-to-needle delay) (HR 0.70, 95% CI 0.61–0.80, p<0.0001).
Women had higher mortality at discharge (13.8% vs. 5.9%, p<0.0001) (Table 3). Excess in-hospital mortality of women with STEMI (crude odds ratio [OR] 2.54, 95% CI 1.99–3.26, p<0.0001) was adjusted by controlling the effect of age, severity, patient delay, and reperfusion therapy (considering the effect of thrombolysis and PCI independently) as is shown in Table 4. After controlling the effect of patient delay, age, both different methods of reperfusion therapy, and the risk of the episode, we found no significant changes in the association between in-hospital mortality and gender (adjusted OR 1.43, 95% CI 1.00–2.06, p=0.049). As the inferior limit of 95% CI was close to the limit of significance, we performed sensitivity analyses using TIMI and Killip risk scores as predictors of risk. Differences in hospital mortality were no longer observed, neither using TIMI risk score (adjusted OR 1.09, 95% CI 0.77 −1.54, p=0.626) nor Killip risk score (adjusted OR 1.37; 95% CI 0.89–2.10).
Every single confounder is presented adjusted to the rest of variables included.
CI, confidence interval; OR, odds ratio.
Discussion
This study analyzes the differences in access to reperfusion treatment for women in Spain and the impact of these differences on hospital mortality. As found in other published studies, 4,13,21 women with STEMI in this study had worse access to reperfusion therapy than did men, mainly due to patient delay. Women were treated for reperfusion less and later. No differences were detected regarding system delay, except among thrombolyzed patients. This increased patient delay in women can be interpreted as a problem of disparity 22 related to gender due to biological, social, behavioral, cognitive, and emotional factors 23 rather than a problem of resource allocation, with some exceptions such as mobilization of fully equipped ambulances after the first contact.
This study highlights the different behavior of the two methods of reperfusion therapy with respect to gender. The probability of a woman being treated with thrombolysis is 30% less than for a man (HR 0.70, 95% CI 0.61–0.80, p<0.0001), whereas no differences were found in the reperfusion treatment by primary PCI (HR 0.94, 95% CI 0.84–1.06, p=0.3455). In this regard, our results differ from other publications, showing identical difficulties of access for women for both methods of reperfusion treatment. 4,13,21 This finding, which merits further investigation, may be due to differences in both clinical and electrocardiographic presentation, more subtle in women, as well as increased baseline bleeding risk. In any case, this appears to be associated with gender disparity more than inequity in resource use, since such differences have not been observed to primary PCI.
In our model, the higher baseline risk, older age, longer patient delay, and the lower rate of reperfusion treatment compared with males contribute in part to this excess mortality, but gender remains an independent factor associated with hospital mortality, regardless of the method of reperfusion considered, when GRACE risk scores were used. The results of the analysis were different when the baseline severity was controlled by GRACE instead of when TIMI or Killip were used. Therefore, despite the GRACE risk score showing the greatest AUC (Table 5), these results should be viewed with caution.
AUC, Area under receiver operating characteristic (ROC) curve.
No independent association between patient delay, total delay before reperfusion, and hospital mortality was found (adjusted OR 1.00, 95% CI 0.99–1.00, p=0.3846). This may be due, at least in part, to the fact that because of the effectiveness of the primary PCI (which in this study is the method of reperfusion used in almost half of patients), it is less time dependent than thrombolysis. 24 –27
Some limitations of our study merit emphasis. Our adjusted analysis does not consider the possible underutilization of other evidence-based therapies (such beta blockers or statins) that may impact on results. 4 Additional gender-related confounders as comorbidities and other clinical, social, behavioral, cognitive, and emotional conditions not included in our model can also influence our results. This study also lacks information about population dispersion. Another important limitation is that our analysis is based on a single registry and is not a population-based study, so we have no data for those patients who fail to contact the health care system, who would be the most serious cases and die before the first medical contact. 28,29 Despite this, the ARIAM-SEMICYUC registry provides a representative, unselected spectrum of patients seen in clinical practice in Spain. 30
Conclusions
Spanish women with STEMI have worse access to reperfusion therapy, presenting with longer delay to the first medical contact. They also have a lower probability of thrombolysis and increased door-to-needle delay (but not door-to-balloon delay). This may be related to the type of clinical and electrocardiographic presentation of women, as well as having an increased risk of bleeding. Therefore, more studies are needed to clarify this aspect. Hospital mortality differences after adjusting for age, patient delay, reperfusion, and severity are probably due to factors intrinsically related to the female sex. The impact of the differences in accessibility on mortality gap remains uncertain. It is important to approach this issue through educational initiatives aimed at women to encourage early access to the health system.
Footnotes
Acknowledgments
We are grateful to all the investigators of the ARIAM-SEMICYUC registry (see Supplementary Appendix S1; Supplementary Data are available online at
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.