
Abstract
Background:
Current recommendations on the rhythm control strategy for treatment of atrial fibrillation (AF) are more restrictive than a decade ago. Gender may play a role in decisions on the management of AF, including application of electrical cardioversion.
Methods:
We analyzed clinical characteristics by gender in patients participating in the observational survey about stable patients underlying cardioversion in Spain (CARDIOVERSE) study (n=915), a survey of the practice of electrical cardioversion in 67 Spanish hospitals. We compared these data with those from a previous survey of electrical cardioversion in Spain (REVERSE study) performed 8 years previously.
Results:
Patients undergoing electrical cardioversion were mainly men (76%). This finding was observed in all age groups, independently of symptoms. Men were younger (62±10 years vs. 69±9 years; p<0.001), more frequently asymptomatic and had a lower prevalence of hypertension and a lower stroke risk. Among asymptomatic patients, the predominance of men was especially evident in older age groups (<65 years, men 76%, women 24%; ≥65 years, men 92%, women 8% (p<0.001). Compared with the REVERSE study, we observed a decrease in the percentage of women among patients undergoing electrical cardioversion (37% REVERSE vs. 24% CARDIOVERSE; p<0.001), mainly in older than 65 years.
Conclusions:
Our results support the hypothesis that gender is a determinant in decisions on the most appropriate strategy for managing AF. We observed a decrease in the percentage of women undergoing electrical cardioversion during the last decade, especially in older asymptomatic patients.
Introduction
T
Gender differences have been observed in the management of ischemic heart disease, with more conservative management reported in women. 7,8 Previous studies also revealed gender differences in the clinical characteristics of patients with AF and in the management of AF. Thus, women with AF are older, more symptomatic, and seem to be at a higher risk of stroke. 9 –12 Data from the Euro Heart Survey on Atrial Fibrillation suggested less frequent use of rhythm control strategies in women. 13
Patients treated with cardioversion represent persistent AF patients treated with rhythm control strategy. In the present study, we investigated the possible influence of gender in decisions on the treatment of patients with AF during the last decade. We analyzed gender-related clinical characteristics in the observational survey about stable patients underlying cardioversion in Spain (CARDIOVERSE) study, a Spanish survey of patients undergoing electrical cardioversion. We also compared the gender distribution in the CARDIOVERSE study with that of the REVERSE study, 14 a survey of electrical cardioversion in Spain performed 8 years previously.
Methods
The CARDIOVERSE study was designed to monitor the clinical practice of elective electrical cardioversion in Spain by prospectively recording all patients with persistent AF who underwent the procedure between February 1 and June 30, 2012, in 67 Spanish hospitals (Supplementary Appendix S1; Supplementary Data are available online at
We analyzed the clinical characteristics of participants by gender and compared the results with those obtained in the REVERSE study, a survey on electrical cardioversion carried out in 96 Spanish hospitals by our group in between January 1 and June 30, 2004, with the same inclusion criteria. 14,15 One thousand five hundred and fifteen patients were included. In that survey, the one-year follow-up was only applied to patients who did not have structural heart disease.
Statistical analyses
Continuous variables are expressed as mean±standard deviation, and comparisons between groups were made using the t test for independent values. Categorical variables are expressed as percentages and were analyzed using the chi-squared test. Differences were considered statistically significant if p<0.05. The statistical analysis was performed using SPSS statistical software package (version 18).
The study was approved by the institutional review boards (clinical ethics committee) of each participating hospital. Written informed consent was obtained from all the patients who participated in this study.
Results
Patients were predominantly men (76%). Table 1 presents the clinical characteristics of patients segregated by gender. The predominance of men was observed in all age groups, although the percentage of women increased with age (Fig. 1). The percentage of patients who had previously undergone electrical cardioversion was similar for both men and women. Women were older and had a lower prevalence of left ventricular hypertrophy, and left ventricular dysfunction and a higher prevalence of hypertension and risk of stroke by hypertension, age ≥75 years, diabetes mellitus, stroke (CHADS2) and congestive heart failure, hypertension, age ≥75 years, diabetes mellitus, stroke, vascular disease, age 65–74 years, sex category (CHA2DS2VASc) scores. Men were predominant in symptomatic (69%) as well asymptomatic patients (85%). The predominance of men in asymptomatic patients was especially evident in older patients (<65 years, men 76% vs. women 24%; ≥65 years, men 92% vs. women 8%; p<0.001).

Distribution of men and women segregated depending on the age range.
Values represent mean±standard deviation or n (%). AF, atrial fibrillation; BMI, body mass index; BSA, body surface area; CARDIOVERSE, observational survey about stable patients underlying cardioversion in Spain; CHADS2, hypertension, age ≥75 years, diabetes mellitus, stroke; CHA2DS2VASc, congestive heart failure, hypertension, age ≥75 years, diabetes mellitus, stroke, vascular disease, age 65–74 years, sex category; CV, cardioversion; EHRA, European Heart Rhythm Association; HAS-BLED, hypertension, abnormal renal, liver function, bleeding history or predisposition, labile international normalized ratio, elderly, drugs/alcohol concomitantly; LA, left atrium; LVEF, left ventricle ejection fraction; NYHA, New York Heart Association.
With respect to the REVERSE study, we noted a decrease in the proportion of women undergoing cardioversion (CARDIOVERSE 24% vs. REVERSE 37%; p<0.001) in all age groups. This decrease was more evident in patients >65 years old (Fig. 2). Women participating in the REVERSE study had higher left atrial size, higher left ventricular ejection fraction and better functional class (Table 2).
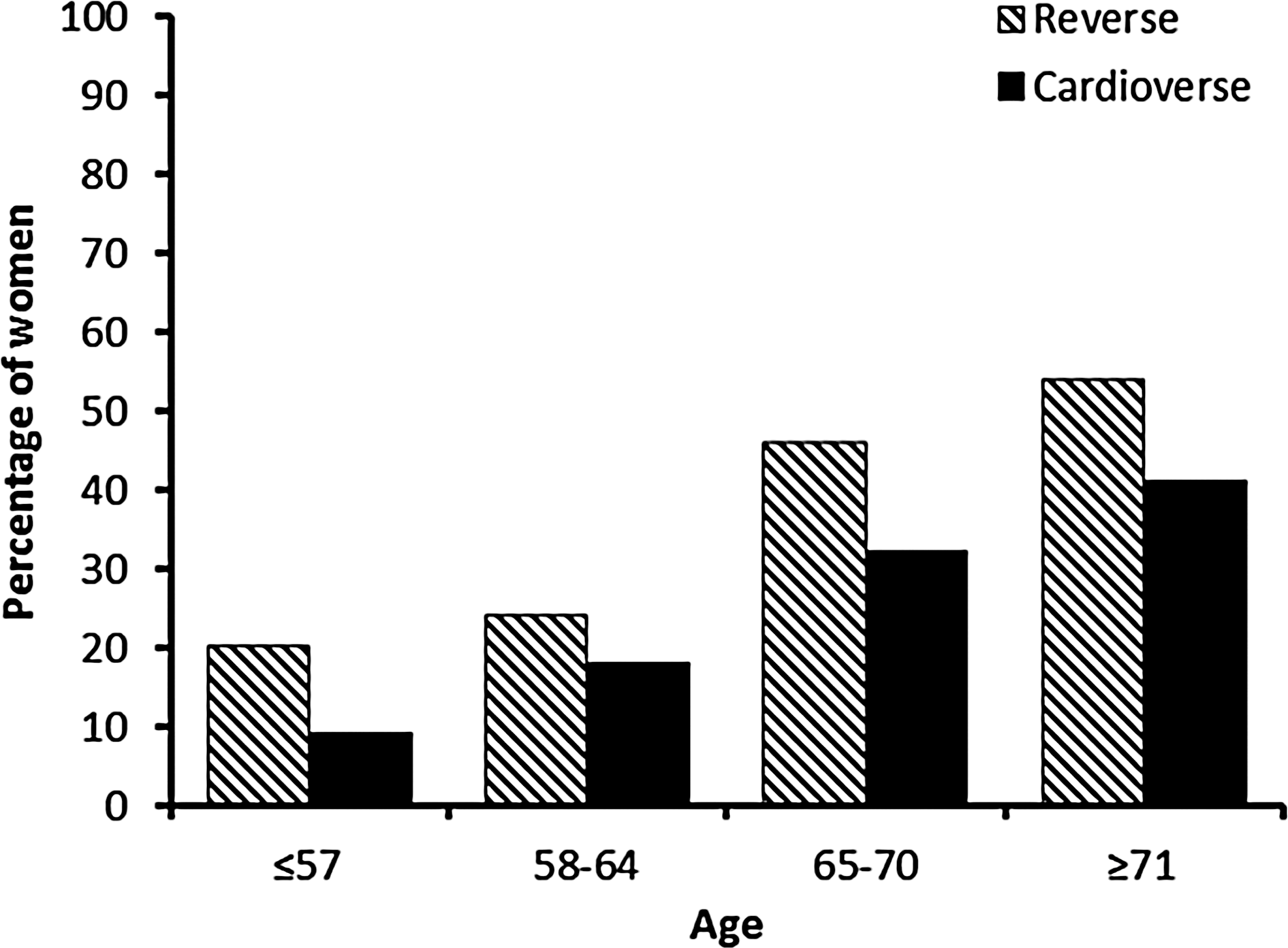
Comparison of the proportion of women between the survey about cardioversion in Spain (REVERSE) and observational survey about stable patients underlying cardioversion in Spain (CARDIOVERSE) studies depending on the age range.
Values represent mean±standard deviation or n (%).
REVERSE, survey about cardioversion in Spain.
We observed in both genders a similar rate of successful electrical cardioversion (men 92% vs. women 94%; p=0.26), maintenance of sinus rhythm at one month (men 58% vs. women 57%; p=0.91) and at one year (men 32% vs. women 29%; p=0.48).
Discussion
Fewer women than men underwent electrical cardioversion. This difference was observed in all the age groups and was independent of the presence of AF symptoms. The greatest difference was in asymptomatic patients in the oldest quartile. In the last decade, fewer women underwent electrical cardioversion, especially in the oldest age group. Our results suggest that electrical cardioversion is underused in women and that gender is taken into account when deciding on the AF strategy to be applied.
Current guidelines recommend stricter criteria for the rhythm control strategy and suggest using electrical cardioversion less frequently. Patients undergoing electrical cardioversion today are more symptomatic and with a higher cardiovascular disease burden. 6 We have observed similar findings in women, comparing their clinical characteristics at REVERSE and CARDIOVERSE studies. It is difficult to speculate about the reasons for variations in use of electrical cardioversion depending on gender. Differences could be due, in part, to a lower prevalence of symptomatic women in the population. However, epidemiological data on patients recently diagnosed with AF showed that women were more likely to have symptomatic AF than men. 9 In addition, the percentage of men was higher in both symptomatic patients and in asymptomatic patients, and men predominated in all the age groups. The poorer prognosis of women treated with a rhythm control strategy described in the RACE study could have some influence on the decrease in the percentage of women undergoing electrical cardioversion in the last decade. 16 Moreover, a higher risk of complications has been described in women undergoing AF ablation 17,18 a technique also implicated in the rhythm control strategy. We cannot conclude that the lower use of electrical cardioversion in women was based solely on the cardiologist decision. In the usual discussion with the patient about the different treatment options, perhaps women are less predisposed to be treated with rhythm control strategy. Further studies are needed to explore the possible gender differences in the perceived risk of cardioversion and stroke.
The main limitation of our study was that we analyzed a group of patients undergoing electrical cardioversion but not the management of patients diagnosed with AF in the population. Previous European epidemiological studies showed an increasing prevalence of AF with aging and higher AF prevalence and incidence in men than in women, 9,18 although the total number of women with AF was higher due to the predominance of women in the oldest age groups. Recent data about the prevalence of AF in Spain show a similar overall prevalence in men and women, 20 although this differed depending on the age group analyzed, with the percentage of women increasing steeply after 60 years. Taking into account the percentage of women in the different ranges of age analyzed in that study, our data clearly suggest a lower use of electrical cardioversion in all the range of age in women. We have observed in women undergoing electrical cardioversion an increased risk of stroke risk evidenced by higher CHADS2/CHA2DS2VASc scores. This was due to a higher prevalence of hypertension and heart failure, but mainly to their older age, as seen in the increased prevalence of women when the age range increased. In treating AF, one of the ways to prevent stroke could be to prevent AF. Women are at higher risk of stroke, but perhaps are not treated as aggressively to achieve and maintain sinus rhythm, which could help to decrease stroke risk. The ongoing EAST study may clarify whether a strict rhythm control strategy can reduce the incidence of stroke. 21
In conclusion, our results support the hypothesis that gender is a determinant in decisions on the most appropriate strategy for managing AF, independently of other clinical factors. We observed a decrease in the percentage of women undergoing electrical cardioversion during the last decade, especially in older asymptomatic patients.
Footnotes
Acknowledgments
This study was funded by Bayer Health Care Spain.
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.