
Abstract
Background:
Despite increasing numbers in academic medicine, women remain underrepresented in top leadership positions. The objectives of this study were to characterize leadership positions held by department of medicine (DOM) faculty at all ranks at one Academic Health Center and to compare leadership positions held by male and female faculty.
Methods:
This was a cross-sectional survey to collect information on all leadership positions from 16 divisions in the DOM at the Johns Hopkins University School of Medicine in early 2012, including type of position, method used to fill the position, and financial compensation. Chi-square testing was used to compare leadership position characteristics by rank and gender.
Results:
The study included 474 DOM faculty at the rank of instructor or higher; 38% were women. Of the 258 leadership positions identified, 35% were held by women. More leadership positions among assistant professors were held by women compared with men (56% of positions vs. 44%), with women assistant professors more likely to hold a leadership position than men (p=0.03). Numbers of women faculty declined at higher ranks, with leadership positions remaining proportionate to faculty representation. Most division director positions (88%) were held by men, and most leadership positions were compensated (89%) and appointed by the DOM chair or a division director (80%).
Conclusions:
Leadership positions held by women and men were proportionate to faculty representation, although the top leadership positions were held almost exclusively by men. While female assistant professors were more likely to hold leadership positions than male assistant professors, these positions appear to be low status positions and it is not clear that they contribute to professional advancement, as few women hold the rank of full professor. Effective interventions are needed to address the gender disparity in top leadership positions.
Introduction
O
Also of concern is the finding that there are qualitative differences in the types of top leadership positions held by women. White et al. found that women medical school deans are more likely to serve at less research-intensive institutions and spend less time in their posts compared with men. 7 These findings underscore the urgent need to define the scope and underlying causes for gender disparity in leadership positions at AHCs and to identify effective approaches to rectify existing disparities.
Multiple explanations and metaphors have been proposed to explain the stagnant advance of women to top leadership positions. The notion of a “glass ceiling” suggests that women find themselves within sight of top leadership positions only to then face universal but invisible barriers to further advancement. In contrast, the “glass cliff” phenomenon suggests that women leaders are often set up for failure by being appointed to positions with greater risk and because they often have less support from mentors and sponsors. 8 Others have described a “sticky floor” in which women are held back by a series of cumulative disadvantages including less institutional support and resources for research, lack of family friendly policies, first appointment at lower ranks, slower rates of promotion, and overt gender discrimination. 5 Finally, “labyrinth” has been used to describe the myriad twists and turns one must navigate to top leadership positions and how this may negatively impact women more often than men. 9 Recent research has focused on the role of unconscious bias and the impact of gender schemas, in particular around role congruity on perceptions of women as leaders. 10,11
To better understand the state of women's leadership within our own department of medicine (DOM), we performed a survey to determine whether there were gender-based differences in characteristics of leadership positions held by men and women within the DOM at a large AHC, the Johns Hopkins University School of Medicine. We examined leadership position type (division director, clinical program director, research program director, etc.), compensation, and selection process. Based on prior studies that demonstrate that women are more likely to earn lower salaries than men and engage in more administrative activities, 12 –14 we hypothesized that women would hold more uncompensated leadership positions than men. We also hypothesized that most leadership positions would be selected by appointment rather than by a search process.
Materials and Methods
Study design
In 2012, we conducted a cross-sectional survey of all leadership positions in the DOM of the Johns Hopkins University School of Medicine. The Johns Hopkins Medical Institutions Review Board reviewed the study and waived review board approval.
Participants
We queried representatives of 16 of the 19 divisions within the DOM to collect information regarding faculty members holding leadership positions within their division. We did not collect data from three small divisions—each had very few faculty, n=4 or less, for a total of 7 faculty that were excluded.
Data collection
We developed a data abstraction instrument to collect information on leadership positions in each division within the DOM. The study authors prefilled the instrument where leadership positions were publicly available on divisional websites and/or by using a Johns Hopkins referral directory. The remaining information was completed by division directors and their representatives (typically division administrators). Respondents were asked to provide the titles of all leadership positions in their divisions. Data collected included the name of the faculty member holding each leadership position, the selection process used to fill the position, and whether the position was compensated (either receiving % full time equivalent [FTE] support or salary supplement) and the amount of FTE support (as a percentage). Although we did not include a specific definition for “leadership position,” we ascertained the number of women in division director positions (used as an American Association of Medical Colleges benchmark for women's representation in leadership roles) as well as lower level leadership positions to generate a complete picture of the leadership opportunities within each division.
The project was initially presented at a regularly scheduled DOM Leadership meeting by the department chair and two authors (AM and LMSR) to make division directors aware of the survey and to answer any questions division directors had on how to accurately complete the instrument. Division directors were then sent an e-mail from the department chair with an electronic copy of the instrument asking them to complete the instrument and make any corrections to the prefilled information. Multiple email reminders were sent to ensure completion of all instruments. The authors were available to all division directors to assist with completing the instrument. The authors also contacted division directors to clarify any inconsistencies or missing information.
We excluded from our analysis the positions of DOM chair (held by a man) and vice chair (held by a woman) and any leadership positions outside of the DOM that were held by faculty with a primary appointment in the DOM such as School of Medicine Vice Deans. Faculty classified as research associates (N=68) were also excluded because these are not tenure track positions and these faculty members did not hold any leadership positions.
Demographic information for faculty, including gender, rank, age at which current rank was achieved and years at current rank of faculty was provided by the DOM chair's office.
Outcome variables included type of position (e.g., division director, clinical program director, research program director), compensation associated with position (receives % FTE/salary supplement for position: yes or no), and selection process (division director/DOM chair appointment, search process/committee appointment, other).
Data analysis
We generated summary statistics for characteristics of faculty leadership positions. Top level positions (division directors) and compensation were compared by rank and gender using chi-square testing. Data were analyzed using STATA Version 11.
Results
DOM faculty characteristics and leadership
Table 1 compares men and women in the DOM by rank, years at current rank, and age at which faculty achieved their current rank. There were 474 faculty members at the rank of instructor or higher, 181 (38%) were women. More men than women held the rank of associate or full professor (14% of faculty were associate professor men, 9% were associate professor women (p=0.64); 18% of faculty were full professor men; 4% were full professor women (p<0.01). Women associate professors were more likely to be at their current rank for fewer years than men (4 vs. 6 years, p=0.02), and women were younger when they achieved a rank of associate professor compared with men (41 vs. 43 years old, p=0.04).
We received completed instruments from 16 divisions in the DOM. A total of 258 leadership positions were identified in the DOM. Of 474 DOM faculty, 199 (42%) held at least one leadership position. Overall women held leadership positions in proportion to their faculty representation, with 181 women comprising 38% of the faculty and holding 91 of the 258 (35%) leadership positions (Table 2).
Women assistant professors were more likely to hold a leadership position than were men assistant professors. Thirty-five of 93 (38%) of assistant professor women held a position compared with 26/111 (23%) of assistant professor men (p=0.03) (Fig. 1). Men and women at the associate and full professor ranks were equally likely to hold leadership positions.
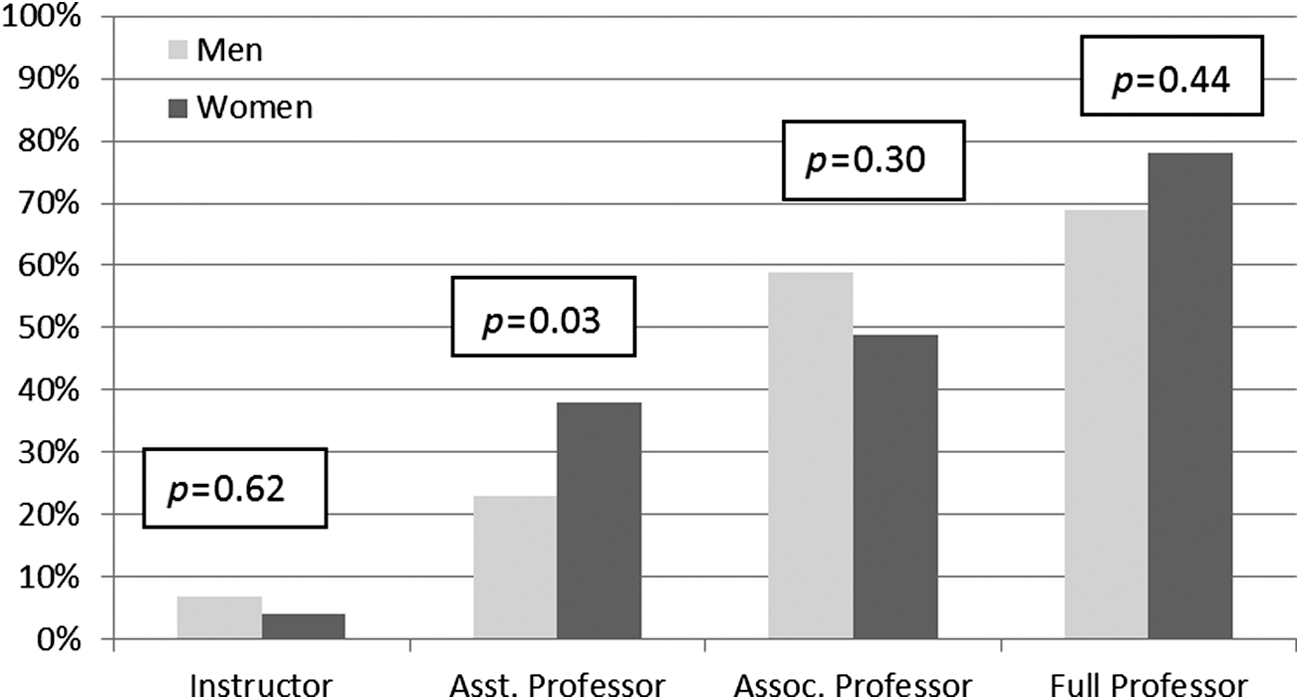
Percentage of faculty members holding leadership role by gender and rank (n=474 faculty).
Table 2 shows summary data regarding the types of leadership positions within the DOM. Most of the leadership positions (43%) were clinical director positions. More division director positions in the DOM were held by men compared with women (88% vs 12%). Other highly visible roles were also predominately held by men (73% of fellowship directors and 68% of clinical directors).
Appointment of and compensation of leadership positions
Most leadership positions (80%) were filled by division director or DOM chair appointment. For division director positions, 32% (6/16) were DOM chair appointments. The remaining positions were selected following a national search. Out of division heads who were the product of a search, 1 out of 10 was female. Out of division heads who were appointed, 1 out of 6 was female.
The majority of leadership positions in the DOM were compensated (89%) by either % FTE or supplement, and there was no difference by gender. Median salary support (% FTE) for leadership positions receiving % FTE was 10%, with an interquartile ratio of 4%–25%, and this did not differ by gender.
Discussion
Based on our survey of all leadership positions within the DOM of a large AHC, we found that the majority of top leadership positions (88% of division directors and 73% of fellowship directors) were held by men. For all leadership positions, women held leadership roles proportionate to their representation within the DOM and assistant professor women were more likely than assistant professor men to hold leadership positions. We hypothesized that women would hold more uncompensated leadership positions than men. We found that the majority of leadership positions received compensation and there were no differences by gender in the receipt of compensation. This finding may be only a partial view of the issue in that we only collected data on percentage of effort associated with a leadership position; we did not collect dollar values for salary supplements related to leadership positions. We also hypothesized that most leadership positions would be selected by appointment rather than by a search. Our data confirmed that the most common selection process for leadership positions was appointment by a division director or DOM chair.
While women faculty in our study hold a proportionate number of leadership positions in the DOM, they are overrepresented among assistant professors with lower level leadership positions and strikingly underrepresented in top DOM leadership positions. This pattern suggests that the “pipeline” theory, which states that once women reach a critical mass in academic medicine they will ascend to top leadership positions, has not borne out. 15 Although women have made up over 40% of medical school classes since 1992 and well over 30% of faculty since 2003 1 (indicating that the pipeline is nearly “full”), few advance to top roles. 16 Our finding that more junior rank women hold leadership positions than do junior rank men in our study adds to the evidence against the argument that women are not interested in leadership. 12,17,18
So why are there so few women found in top leadership positions? The process of leadership position appointment is both complex and critical to ensuring diversity in the top echelons of organizations. Some of our findings may be explained by second generation bias, which suggests that the interplay of existing gender schemas and organizational structures contribute to the lack of gender parity in top leadership. Key to understanding and remedying this is knowing that second generation bias does not result from intentional discrimination against women but rather can be attributed to unconscious biases. 19,20 Unconscious bias results from ingrained social stereotypes that help us interpret and interact with our personal and professional worlds, and that may be in direct conflict to our expressed values and beliefs. It is these social stereotypes that lead us to make unconscious associations and assumptions. For example, unconscious bias might result in the following thought process when considering a faculty person's potential for leadership: top leaders are strong, decisive, risk takers; women are communal, supportive, and nurturing, therefore women do not make good leaders. Role congruity is another form of gender stereotyping that influences the perceptions of how women perform as leaders. For example, when women demonstrate traits typically associated with leadership they are judged more harshly because female traits are viewed as “incongruous” with leadership. 11
Another manner in which unconscious bias and gender schemas may contribute to women not advancing into top leadership positions may be through stereotype threat. Stereotype threat occurs when stereotypic traits of a group are linked to performance outcomes. Group members have been shown to consistently underperform when made aware of this link between specific stereotypes and ability. An example includes the performance of women on assessments of math skill when prior to assessment they are “reminded” that women are not as good at math as men. 21
When gender stereotypes become explicit, such as women are collaborative and men are assertive, and these are then linked to an outcome such as leadership (better leaders are assertive and competitive), it is easy to understand how stereotype threat might affect women's performance. 22 While the potential for stereotype threat to impact many areas of women's advancement in academic medicine exits, our study did not explicitly test for this, and it is an area for future research efforts. There is a large body of compelling evidence from multiple disciplines demonstrating that unconscious bias influences hiring, evaluation, and appointment of leadership positions. 10,23,24 Our study found that the vast majority of leadership positions, with the exception of the division director positions, were made by direct appointment and not by a search committee. While we did not empirically test for the impact of unconscious bias in the appointment of leadership positions in our study, the overwhelming evidence suggesting that unconscious bias plays a role compels us to at the least offer suggestions for mitigating the influence of these hidden biases.
The American Association of Medical Colleges has developed an informative and practical primer on addressing unconscious bias in the search and recruitment process. 25 Evidence based interventions include: increasing the number of women considered for upper level leadership positions (considering a larger number of qualified women may increase the ability of search committee members to “see” women as leaders); creating clear criteria for positions to prevent reviewers from defaulting to candidates who fit the stereotypical “leader” profile; using gender neutral language in role descriptions and evaluation tools (for example, avoiding stereotypical male descriptors such as “independent” or “risk taker” that may lead to automatic, implicit associations with male candidates); developing a consistent, agreed-upon set of questions to ask all candidates; and finally, providing teaching around unconscious bias to raise individual and institutional awareness. 25 Ensuring that top leadership roles are filled using transparent search processes, allowing candidates to self-nominate, and rotating leadership roles using fixed term limits represent other strategies that may enhance diversity in top leadership positions. 26,27 A logical next step for our group is to explore the characteristics of divisions that successfully promote women and to develop “best practices” based on those divisions.
It is clear that not all leadership positions can be appointed by search committees due to cost and practicality. In these situations, visibility and “whom you know” can be critical to advancement. The lack of sponsorship and access to effective networks for women may also influence leadership appointments to their detriment. 24 Even women medical students appear to be explicitly aware of the power of male sponsors and male networks and yet feel cut off from these early on in their medical training. 28 Within our department we are developing an intervention to identify a “sponsor in chief” (someone with influence within the institution and nationally) in each division who would be aware of potential national leadership positions, specifically with the aim of nominating qualified and interested women to these posts (R.B. Levine, personal communication).
Another explanation for the lack of women in top leadership roles may be that the nature of the leadership positions held by junior women may not contribute to career advancement or promotion. This is multifaceted. First, women often accept lower level “helping” or “housekeeping” leadership positions. 29 These roles typically benefit the institution but may not propel women to higher status leadership positions because they do not support the growth of leadership skills or networking opportunities. Examples of these types of positions include grand rounds director, minor course or clinical program director, or director of a Continuing Medical Education (CME) event. The high number of women in these positions could result from unconscious gender bias and may also perpetuate it. 30 Women in these positions may be less likely to be viewed by others as having leadership potential and this view could be internalized resulting in a limited ability of women to build their own leadership identity and goals. 31 Furthermore, gender status beliefs (i.e., the perception that men are more successful leaders than women because they have more control of resources within a society) might lead to the perception that women leaders are less influential than men when holding a similar role 32 and potentially make women less likely to advance to upper-tier roles.
If women do not attain top leadership roles such as division director, they lack the status and influence along with the resources to, for example, hire and retain faculty. This is analogous to “line” and “staff” roles in the business world, where line positions have more power and influence and staff positions are support roles. Gender stereotypes drive women to be identified as caretakers and therefore more likely to be seen as appropriate for staff roles, while men take charge in line positions and have problem-solving roles with more power and influence. 33
Especially important to careers in academic medicine, participation in the often time-consuming activities attached to lower level leadership positions could deter from productivity in terms of publications and grant awards. We found that leadership positions overall were not supported by a large percent effort, making it unlikely that substantial outcome would result based on all the other competing demands of an academic medicine career. Publications and grants are linked to promotion to upper ranks and rank is often associated with leadership. 34 The path to leadership remains a complex one for women. 16,30 Individuals in top leadership positions in academic medicine frequently follow a specific trajectory. Women appear to be derailed more often along this path. For example, many deans have served as department chairs, and department chairs are more likely to have been division directors and accomplished researchers as measured by number of publications in top journals. 16,30 Despite these seemingly clear associations, even when women successfully navigate the initial and intermediate steps, they frequently do not track to top leadership positions. 12,34
Our study has several limitations. First, our data is from a single institution that has previously implemented extensive efforts to retain and promote women, 6 and this may influence our findings compared with other institutions. Second, we did not specifically define “leadership position” in our data collection instrument, which may have allowed for a social response bias and an overreporting of relatively minor positions. Third, data were reported by division directors or their representative administrators and not by individual faculty members, which could lead to missing or incorrect data; however, we did use public sources to prefill our instrument and all division director positions were verified. Fourth, as with all cross-sectional designs we cannot comment on causality. Fifth, we used % FTE to determine compensation. Salary data might have identified gender inequities. Finally, our study did not collect information on faculty aspirations to hold leadership positions.
Conclusion
Although our study identified a significant percentage of women faculty holding leadership positions throughout the DOM, very few were top level, high status positions with significant resources, such as division directors or clinical directors. Division directors can recruit, hire, and retain faculty and allocate resources necessary for faculty success compared with individuals in other lower level roles who do not have such power or influence. Our findings are supported by descriptions of women in leadership at the national level in academic medicine. 1 The pool of potential women leaders represents a tremendous resource to AHCs. Although further studies are needed, our results suggest that alternative approaches to address gender bias, support and promote women, and provide leadership opportunities are urgently needed to ensure diversity at medical schools and AHCs.
Footnotes
Acknowledgments
The authors wish to thank Dr. Myron Weisfeldt, former Chair, Department of Medicine, Johns Hopkins University School of Medicine, and his office staff for support of this project and providing data on DOM faculty.
Author Disclosure Statement
No competing financial interests exist.