
Abstract
Background:
Utilization of breast reconstruction services remains low among women who underwent mastectomy despite the improvement in quality of life associated with this treatment. The objective of this study is to identify the effect of the Women's Health and Cancer Rights Act (WHCRA)—an understudied ongoing federal law that mandated insurance coverage of breast reconstruction following mastectomy beginning in 1999—on use of reconstructive surgery after mastectomy.
Methods:
We use a difference-in-differences (DD) approach to identify the change in breast reconstruction utilization induced by WHCRA by comparing the pre- and post-policy changes in utilization between states that did not have existing laws mandating coverage before the WHCRA (treatment group) and those that had such state laws (control group). The data are from the Surveillance, Epidemiology, and End Results program. The main sample includes 15,737 female patients who were under the age of 64 and underwent mastectomy within 4 months of diagnosis of early stage breast cancer during 1998 and 2000.
Results:
Based on the DD model, the odds of using reconstruction services in the states without preexisting laws increased after the WHCRA by 31% in 1999 and 36% in 2000 (compared with 1998 before the WHCRA). These effects are masked in a simple pre/post model for change in reconstruction across all states. Additional analyses through 2007 indicate that the WHCRA had long-term effects on utilization. Furthermore, analyses by state indicate that most states in the treatment group experienced a significance increase in utilization.
Conclusions:
The use of breast reconstruction after mastectomy significantly increased after the WHCRA. At a minimum, our estimates may be considered the lower bound of the real policy effect.
Introduction
F
Despite their importance, the effects of several federal mandates on health care use and health outcomes remains poorly understood. One such policy is the Women's Health and Cancer Rights Act (WHCRA) passed on October 21, 1998, which mandated that effective January 1, 1999, health insurance providers must cover breast reconstruction after mastectomy, reconstruction and surgery of the other breast for a symmetrical appearance, and care for physical complications and prostheses in all stages of mastectomy. 1 In 2001, additional legislation was passed to enforce penalty for noncompliant insurers. 2 This law was passed to improve access to breast reconstruction among women who underwent mastectomy, a service that has been shown to increase their quality of life. 3 Utilization of breast reconstruction among eligible patients had been historically low—less than 20% of eligible patients—with significant geographic and racial/ethnic disparities in the United States. 4 –6
Although the WHCRA was the first federal level legislation related to insurance coverage of breast reconstruction following mastectomy, a total of 28 state-level legislations had already been passed prior to the WHCRA. 7 Most of these state-level legislations mandated essentially the same or very similar coverage as the WHCRA. Four states mandated coverage over a specific period following mastectomy. For example, Pennsylvania and Tennessee mandated coverage for reconstruction during 6 and 5 years, respectively, after mastectomy. Most of states required insurers to cover at least one of these: prosthetic devices, reconstructive surgery, and restoring symmetry. None of the state laws set coverage limits except for Connecticut. 7
Accurate estimation of the WHCRA's effect is critical for evaluating the effectiveness of this important law in enhancing access to reconstruction services and for determining the need for further interventions. Only one study evaluated the impact of the law on utilization and concluded that the WHCRA did not significantly increase breast reconstruction use. 6 However, this result may have been seriously biased by not accounting for the fact that some states had enacted similar legislations prior to WHCRA as mentioned above. One cannot ignore these state laws when evaluating the effect of WHCRA on breast reconstruction utilization. The WHCRA is expected to enhance breast reconstruction utilization in states that did not have state laws that are comparable to WHCRA, but not in the states that had already mandated similar coverage as the WHCRA. Ignoring these state laws when evaluating the effect of WHCRA nationwide may lead to seriously biased results and wrong conclusions regarding the law's effectiveness.
In this study we take advantage of the variability in the presence of state laws mandating reconstruction benefits in order to identify the WHCRA's effect on use of reconstruction services in the states that did not have the law. Specifically, we use a difference-in-differences (DD) approach to identify the changes in breast reconstruction use over the period before and after the WHCRA became effective between the states that had a state law mandating similar coverage before the WHCRA and those that did not. 8
Methods
To estimate the policy effect on utilization, one cannot simply calculate difference in utilization before and after the policy. This approach may yield biased results due to time-trend effects or other unobserved events that happened during the same time period as the policy. The DD model, an econometric design that is commonly used in the economics literature to estimate policy effects, is particularly appealing in such cases. 8
The basic idea of the DD design is to subtract the outcome change before and after the treatment in a control group that is unaffected by the policy from the outcome change in the treatment group during the same period of time. This removes the biases in the simple pre/post comparison within the treatment group by taking out time trends or other unobserved effects happening at the same time as the policy change that are assumed to affect the control group in the same way as the treatment group. It also removes biases from pertinent differences between the treatment and control groups that affect direct comparisons of pre- or post-policy outcomes as only changes within each group are compared. 14
In our case, as opposed to a traditional DD design that compares a treated group with a nontreated control group, all states were exposed to the WHCRA. However, a group of states had passed state laws mandating the same coverage for breast reconstruction following mastectomy as the WHCRA provision. The WHCRA is expected to have little additional direct impact on the breast reconstruction utilization rates in this group. Therefore, we consider these states as the control group and the other states that had no laws mandating coverage prior to the WHCRA as the treatment group. There may be spillover effects on reconstruction use in the control-group states after the WHCRA was enacted. However as discussed below, this will bias the estimated WHCRA effect downward if anything, which provides a lower-bound estimate of the WHCRA effect.
The estimated WHCRA effect represents the difference in the changes in breast reconstruction use (following mastectomy) before and after the WHCRA between the control states and the treated states. We also adjust for several individual-level demographic and clinical characteristics. The DD model can be estimated by regressing breast reconstruction use on the state control treatment group indicator (state with prior mandatory coverage law versus without), year indicators (for years after versus before the law), interactions between the state control treatment group indicator and year indicators, and other individual-level covariates (X) as shown below.
In this model, the coefficients of the interactions between the treatment group and year indicators δ represent the law's effects in various years after its implementation. Alternatively, one can replace the treatment indicator with state dummies to control for state-level variation. However, including interactions between the state dummies and year indicators may result in collinearity problems in the model. Instead, since the treatment group indicator is a fixed characteristic and we are primarily interested in capturing the average law's effect across the treated states (instead of specifically for each state), we leave the interactions between the treatment group indicator and the year dummies as in equation (1), but replace the main (uninteracted) treatment group with state indicators (states) as shown below.
Similar to equation (1), the coefficients of the treatment group and year indicators represent the policy effects in the DD model. We consider this our preferred specification as it captures baseline differences in reconstruction between the various states, but the results of the interactions are similar to equation (1). Therefore, we only report the regression results of equation (2) [detailed results from equation (1) are available from the authors].
We use 1998 as the pre-WHCRA period and focus on estimating the utilization change in 1999 and 2000. We focus on the first 2 years after implementation in order to reduce the threat of other events and time trends that may confound the law's effect when examining a longer period. However, we show below estimates through 2007. We estimate equation (2) using logistic regression. The dependent variable is the receipt of breast reconstruction within 4 months after diagnosis of breast cancer. 9 The Surveillance, Epidemiology, and End Results (SEER) program dataset does not provide the date of surgery, but only captures surgeries in the initial course of treatment within 4 months after diagnosis. We discuss the implication of this for our estimates below. The independent variables include the state dummy variables, year at diagnosis (indicators for 1999 and 2000 versus 1998), and interactions between year at diagnosis and state treatment group indicator. We also control in X for patient's marital status, race/ethnicity (Hispanic, white, black and other), cancer stage (0, 1 and 2, stage 3 and 4 excluded), radiotherapy treatment, and age at diagnosis. All variables of interest are coded as categorical variables, except for the continuous variable of age at diagnosis. Also, we graphically evaluate the adjusted rate of breast reconstruction use between control and treatment groups over time from 1998 to 2000 based on the logistic regression estimates. First, we calculate the predicted probability of receiving breast reconstruction post mastectomy for each patient. Next, we calculate the adjusted rate of reconstruction as the sum of these predicted probabilities across patients divided by the total number of patients in each year and control/treatment group category.
Study population
Using data from the SEER program, we identify 50,387 females who were diagnosed with breast cancer and underwent mastectomy during 1998 and 2000. Figure 1 provides a flow chart for sample selection. Stage 3 and 4 patients are excluded as they were much less likely to receive reconstruction surgery, and those who did were more likely to consider other factors than coverage when making the decision. Since the WHCRA's provision does not extend to Medicare, which had its own coverage policy for breast reconstruction following mastectomy, we restrict our sample to patients younger than 64 years of age at the time of diagnosis. 16 The SEER program collects data on cancer cases diagnosed in population-based cancer registries that currently represent 28% of the population. 15 We include data from 13 cancer registries in 10 states (California, Connecticut, Georgia, Hawaii, Michigan, Alaska, New Mexico, Washington, Utah, and Iowa) that were continuously collecting data between 1998 and 2000. We exclude registries from three states—Kentucky, Louisiana, and New Jersey—that started data collection in 2000, after the WHCRA. These eligibility criteria exclude 32,290 observations from the sample.
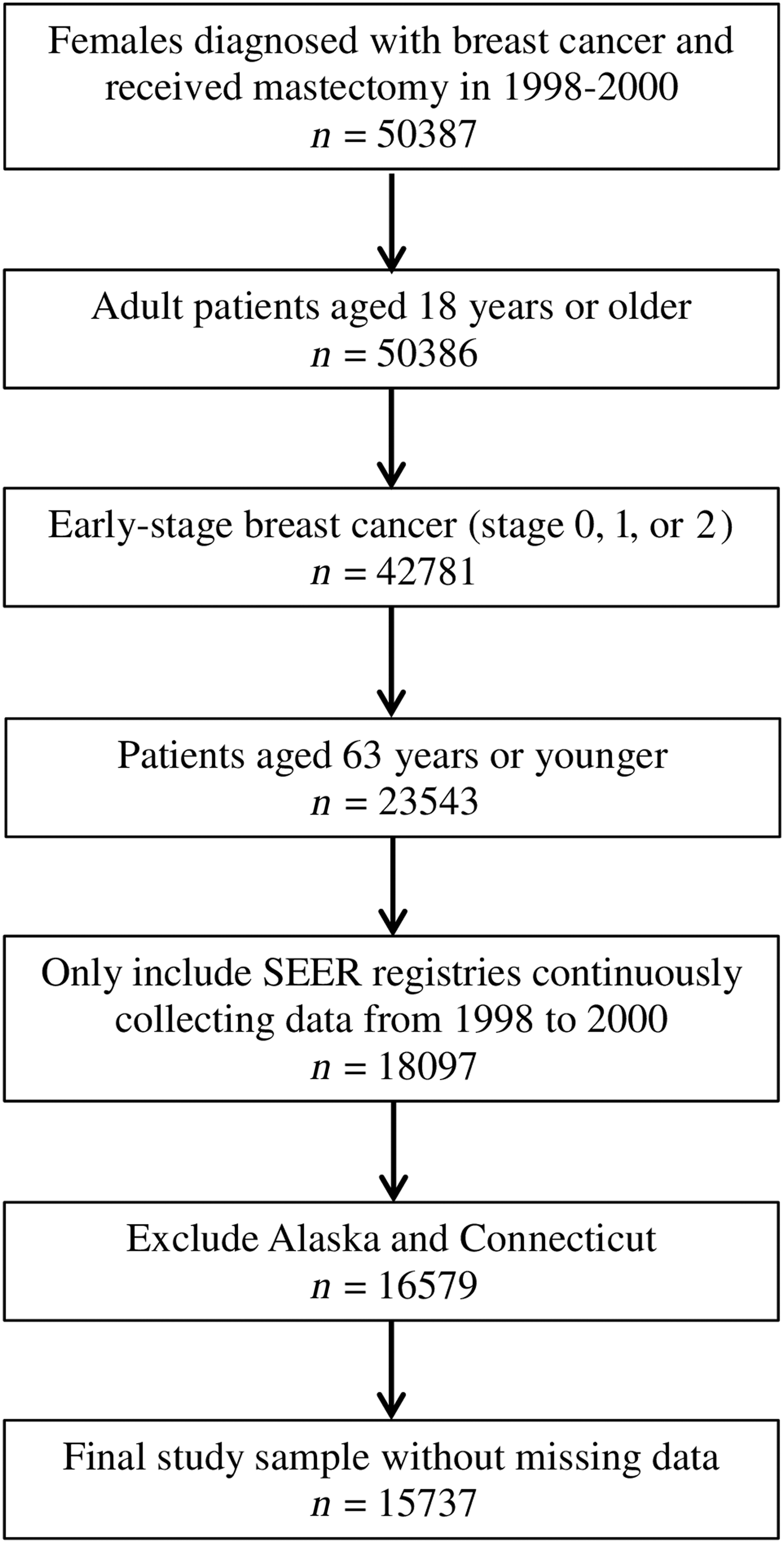
Study sample and eligibility criteria.
Among the states retained in the study sample, California, Michigan, and Washington had passed state legislations essentially mandating similar coverage as WHCRA prior to 1999. 9 The California state law was effective in 1980 and mandated coverage for prosthetic devices and reconstructive surgery after mastectomy, including restoring symmetry for the unaffected breast. 10 The Michigan state law was enacted in 1983 and covered breast cancer rehabilitative services, including reconstructive plastic surgery and physical therapy. 11 The Washington state law was also enacted in 1983 and covered reconstructive breast surgery following mastectomy. 12 The Washington state law was amended in 1986 to mandate coverage for surgery to reestablish symmetry.
The other five states, excluding Connecticut, had no legislation related to breast reconstruction insurance coverage. Connecticut, which is also one of the SEER registries, passed a similar mandatory coverage state law in 1991. 13 However, one significant difference between the Connecticut legislation and the other three SEER state laws is that it specified a minimal yearly benefit of $500 for reconstructive surgery and $300 for prosthesis for each breast removal, while the other state laws specified no limit. So the effectiveness of the 1991 Connecticut state law in enhancing coverage is uncertain. To avoid the potential bias, Connecticut is not included in either the control or treatment group in the main analysis. However, we include Connecticut in the control group in a sensitivity analysis. Additionally, patients in Alaska are also excluded because the SEER recorded extremely low numbers of breast reconstruction cases for Alaska during the study period, which raises a concern over the reporting accuracy of reconstruction surgery in Alaska. Excluding Connecticut and Alaska drops 1,518 observations from the analysis. Our final study sample after all exclusion consists of 15,737 patients.
With the DD approach, we divide the SEER states into two treatment and control groups. The treatment group includes the following states that did not have state-level legislations mandating breast reconstruction coverage prior to WHCRA: Georgia, Hawaii, New Mexico, Utah, and Iowa. The control group includes the following states that had these legislations: California, Michigan, and Washington.
The study was considered non-human subject research by the University of Iowa Institutional Review Board.
Results
Table 1 shows the descriptive statistics of variables used in the analysis. Twenty-nine percent of the patients in the study sample received breast reconstruction. The mean age at diagnosis was 50 years old. Sixty-eight percent of the patients were married at the time of diagnosis. Sixty-nine percent are white, 9% are black, and 13% are of another race. Nineteen percent in our study sample received radiotherapy. In terms of year of diagnosis, our sample is evenly distributed across the 3 years.
Only age at diagnosis is included a continuous variable; other variables are included as categorical.
Denotes SEER registries that are not statewide. In these cases, the areas in the state covered by the registry are in parentheses.
SD, standard deviation; SMSA, standard metropolitan statistical area.
Figure 2 shows the breast reconstruction utilization rates in the treatment and control state groups from 1998 to 2000, adjusted for the measured patient demographic and clinical factors. Utilization rates were very close on average before the WHCRA between states that had coverage laws (28%) and those that did not (29%). This is not necessarily surprising since utilization rates vary between states due to several factors including differences in health care delivery and insurance systems, physician practice patterns, socioeconomic characteristics, and culture. 6,17 These differences could attenuate the average effect of state laws for breast reconstruction coverage on utilization across the states that enacted these laws bringing their average utilization rate prior to the WHCRA closer to that in states without coverage laws. However, average rates also mask state-level differences in utilization prior to the WHCRA within both the treatment and control groups, which are discussed below. More importantly, however, the rates change differently after the WHCRA between the two state groups. Among the states with state laws before WHCRA (California, Michigan, and Washington), the adjusted breast reconstruction rates did not increase substantially from 1998 to 2000. In contrast, among the states without state laws before WHCRA, the adjusted breast reconstruction rates showed an overall upward trend during the three years.
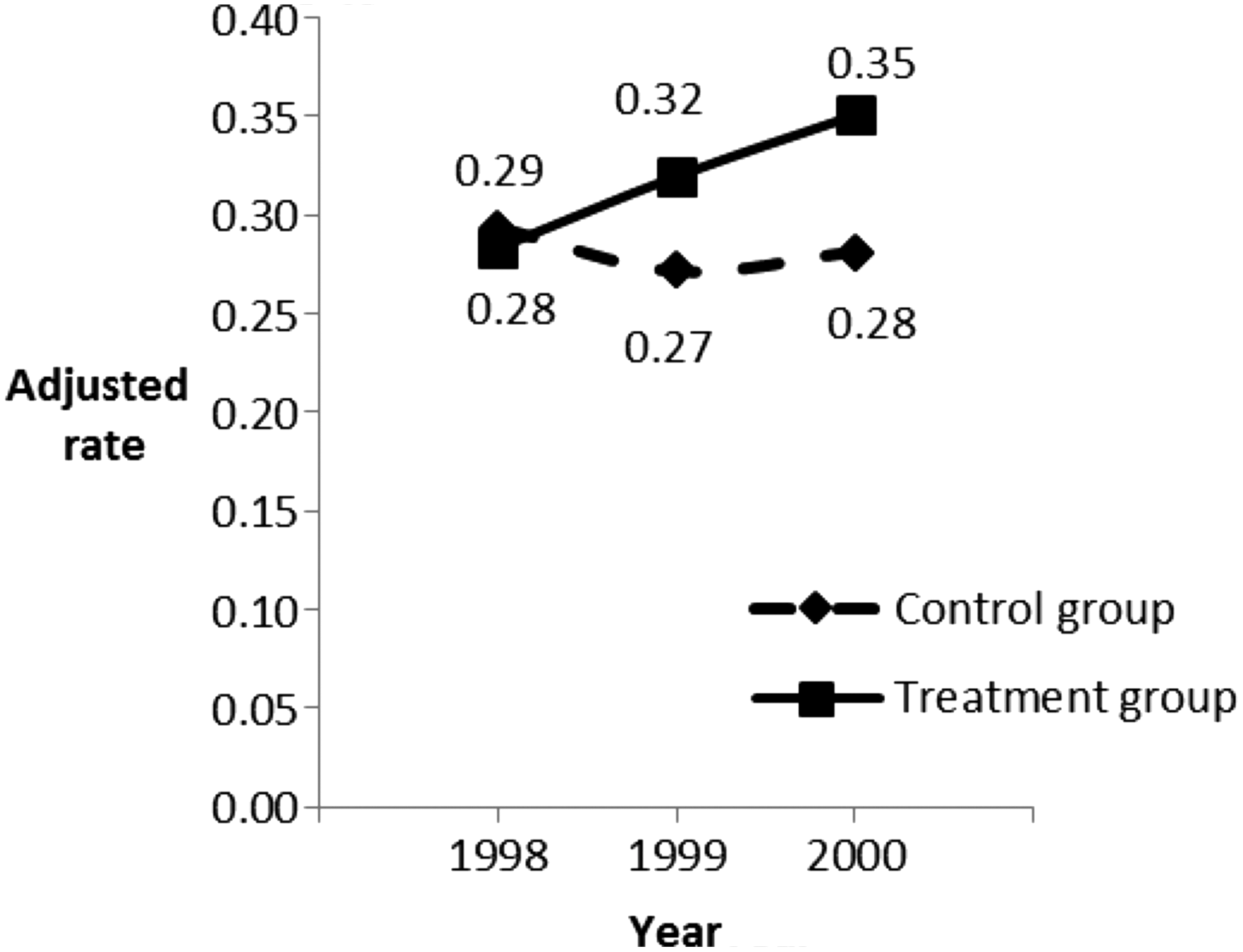
Adjusted rates of breast reconstruction use in treatment and control groups. The rates are adjusted for marital status, race/ethnicity, stage of breast cancer, use of radiation, and age at diagnosis.
Table 2 reports the logistic regression results from the DD model. Compared with the control states that had coverage mandates at the time the WHCRA was implemented, the utilization odds in the treatment group including states without such state laws increased after the WHCRA by an additional 31% in 1999 relative to 1998 (before WHCRA). Furthermore, the utilization odds increased in 2000 relative to 1998 by an additional 36% in the treated states compared with the control states. Both effects are statistically significant at p<0.01. In the sensitivity analysis that includes Connecticut in the control group (states with existing state coverage mandates), the results are similar to those from the main analysis: the utilization odds in the treatment states increased significantly after WHCRA (1999 and 2000) relative to 1998 compared with the control states (detailed results available from the authors).
The model simultaneously includes all the variables shown in the table.
p<0.01.
CI, confidence interval; DD, difference-in-differences approach; OR, odds ratio; WHCRA, Women's Health and Cancer Rights Act.
Other model covariates also have significant and interesting effects on reconstruction use. Non-white patients were at least 50% less likely to undergo breast reconstruction than whites (odds ratio [OR]=0.5 for black and Hispanic patients and 0.3 for other race; all significant at p<0.01). In terms of cancer stage, patients in stages 1 and 2 were significantly less likely to undergo breast reconstruction compared with stage 0 patients (OR=0.53 and 0.36, respectively, for stages 1 and 2; p<0.01). Patients who underwent radiation were less likely to undergo breast reconstruction (OR=0.68, p<0.01). Older patients were also less likely to undergo breast reconstruction (OR=0.95 for each additional year of age).
The model also shows state-level variation in utilization rates within the treatment and control groups before the WHCRA. Patients in Michigan are more likely to use reconstruction surgery than those in California, while those in Washington are less likely to do so. Similarly, three states in the treatment group (Hawaii, Iowa, and Utah) have lower utilization rates than California, but Georgia has a higher rate. As mentioned above, this variation is partly driven by state differences in health care availability and practices, insurance coverage, demographic and socioeconomic characteristics, and culture. 6,17 However, this state-level variation does not violate the DD assumptions. The DD framework that we employ to estimate the average effect of the WHCRA controls for utilization trends that resulted from other changes besides the WHCRA and affected both the treatment and control groups and is not biased by differences in utilization rates in 1998 prior to the WHCRA between states and between treatment and control state groups.
Discussion
We find that the WHCRA mandating insurance coverage significantly increased the breast reconstruction utilization rates following mastectomy in the states that had no state-level laws mandating reconstruction. This suggests that this policy improved access to reconstruction care as intended. The magnitudes of the estimated increase—31% and 36% in the odds of utilizing reconstruction services in 1999 and 2000, respectively, versus 1998—are of reasonable magnitude, which adds further validity to the study results. On a larger level, our study provides a broader understanding of the effects of federal mandates of health care coverage on utilization and highlights the effectiveness of policies mandating insurance coverage for health care services that may be inadequately covered in improving patient access to needed treatments.
The identification of this policy's effect requires meeting the assumptions of the DD model that: (1) the trends we observe between the treatment and control states have not started before the law and are not confounded by transitory events, and (2) there is no effect of the federal mandate on control states that had similar laws. One limitation of the SEER dataset is that it does not provide data on use of reconstruction services before 1998, which limits our ability to verify these trends over the pre-law period. However, as can be seen in Figure 2, the control states had a fairly flat trend without major increases in utilization between 1998 and 2000, consistent with our expectation given that these states had laws mandating essentially similar coverage as the WHCRA, unlike the treated states, which had noticeable increases in utilization. Furthermore, the number of breast reconstructive surgeries per year in all states included in the Nationwide Inpatient Sample (NIS) from the Healthcare Utilization Project was fairly steady between 1993 and 1996 (around 73,000–75,500 surgeries per year), a period when all of the states represented in the NIS had no mandates of reconstruction services, with the exception of Maryland which passed a mandate on Oct 1, 1996. 18 This strongly suggests that there were no historic trends of increases in use of reconstruction services in states without laws, further supporting the assumptions of the DD model. Any further threats to the assumption of the DD model, such as some insurers in the treated states anticipating the WHCRA and offering coverage before the law went into effect, or the possibility of a delay in the effect as patients may have needed time to learn about the law, would have biased the effects of the policy downward, rendering our estimates as a lower-bound of the real effect.
The flat trend of utilization in the control states shown in Figure 2 supports the second assumption of the DD model of WHCRA having no effect on these states and that the federal mandate substituted for state laws mandating coverage in these states. Here again, any potential threats to this assumption will likely result in underestimation of the effect and lower-bound estimates. For example, one could hypothesize that WHCRA had spillover effects on utilization in the control states by raising awareness of breast reconstruction among patients and physicians, which could have had some positive effect on utilization even though these states had already mandated coverage for breast reconstruction. However, for such effects to have occurred they would have to have been counteracted by some time trend or unobserved events since we see little change in use in the control states. We are unaware of any such trends of events. Furthermore, any positive spillover effects on the control states would result in underestimating the real policy effect on the treated states.
We focus on the first 2 years after the WHCRA implementation in order to reduce the threat of time trends from other events besides the federal mandate that are more likely to confound the law's effect when examined over a longer period post implementation. However, it is possible that the law had an immediate effect that dissipated over time, or conversely that the effect increased over time as individuals and providers became more aware of the law. In additional models, we estimated the overall effect of the WHCRA across 9 years from 1999 through 2007 (Table 3, model A) and then examined the WHCRA effect separately in each year (Table 3, model B) using the same DD framework described above. We found a significant increase in utilization across the entire period; overall utilization odds in the treatment states increased by 50% in this period. The effects are more prominent after 2001, which is the only year that shows no significant increase. These results indicate that the WHCRA had both immediate and long-term effects on utilization.
The models control for marital status, race/ethnicity, stage of breast cancer, use of radiation, and age at diagnosis.
The DD coefficient is the coefficient of the interaction term between the treatment group indicator and the post-law indicators (one indicator in model A for years 1999–2007 and individual year indicators in model B). The reference period in each model is 1998.
Our main analysis focused on the average effect across the states in the treatment group. It is possible, however, that the WHCRA effects varied between states. Figure 3 shows adjusted breast reconstruction utilization separately by state. There is a trend of increased utilization after the WHCRA in all treatment states but no evidence of an increase in the control states. In order to formally evaluate the heterogeneity in WHCRA effects between states in the treatment group, we reestimated the DD model including interactions between the post-WHCRA period and separate indicators for those states (the reference group remains all states in the control group combined). We estimated a model first for 1999 through 2000, with separate effects for each year (Table 4, model A), and then a model for the entire period from 1999 through 2007 (Table 4, model B). These models show that all states in the treatment group show an increase in utilization post the WHCRA except for Georgia and Utah in 1999. Of all states, only Georgia did not have a significant increase after the WHCRA when examining effects through 2007, possibly because of the much higher utilization rate in this state prior to the WHCRA. Hawaii has the largest increase from 1999 through 2007 followed by Iowa. The effects are similar between New Mexico and Utah across this period. Overall, these results indicate that most states in the treatment group experienced a significant increase in use of reconstructive surgery after the WHCRA, despite some heterogeneity in effects between states.
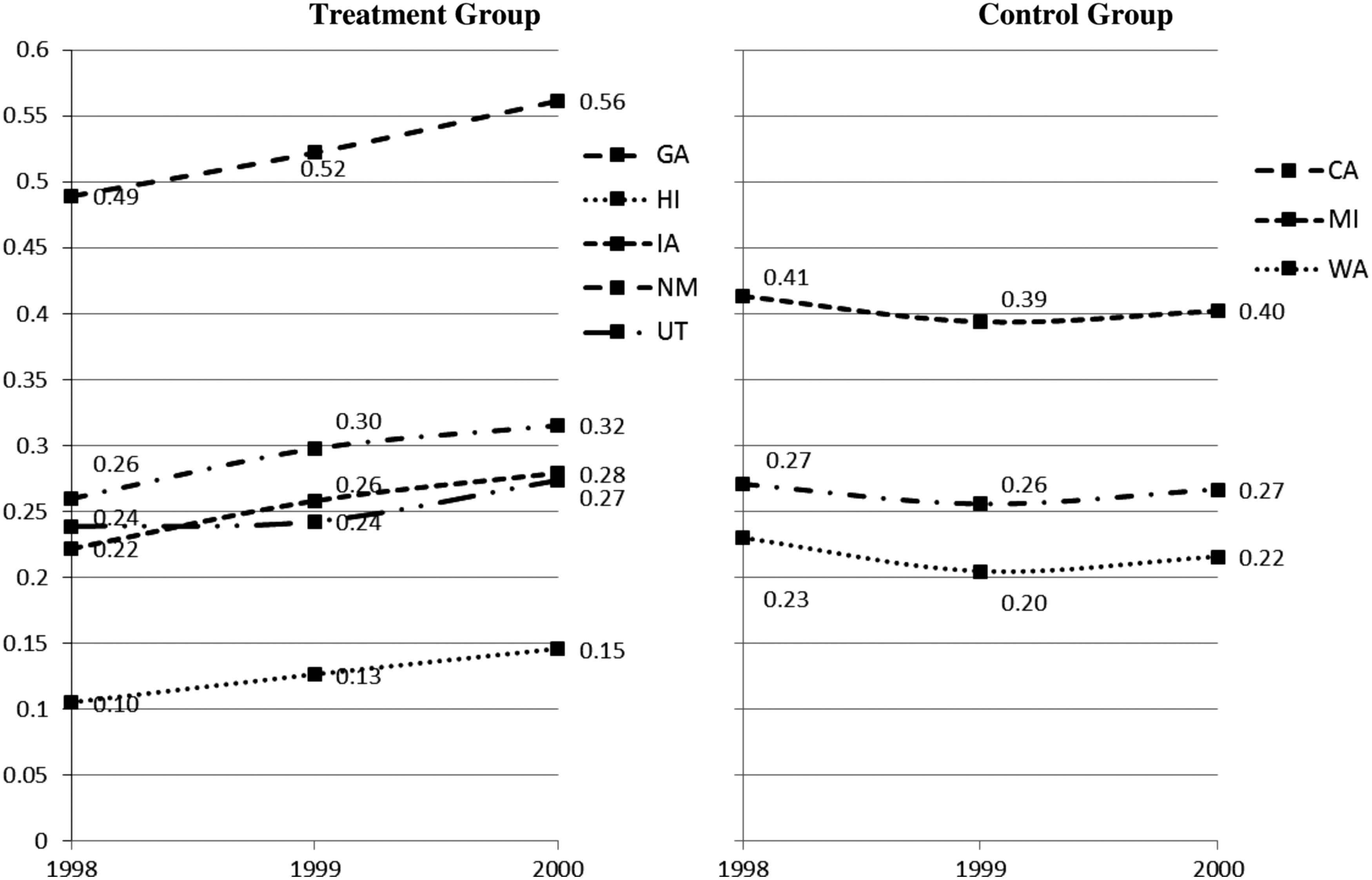
Adjusted rates of breast reconstruction use by state. The rates are adjusted for marital status, race/ethnicity, stage of breast cancer, use of radiation, and age at diagnosis. CA, California; GA, Georgia; HI, Hawaii; IA, Iowa; MI, Michigan; NM, New Mexico; UT, Utah; WA, Washington.
The models control for marital status, race/ethnicity, stage of breast cancer, use of radiation, and age at diagnosis.
The DD coefficients are the coefficients of the interaction terms between the indicators of states in the treatment group and the post-law indicators (indicators for 1999 and 2000 in model A and one indicator for 1999–2007 in model B). The reference period in each model is 1998.
CA, California; GA, Georgia; HI, Hawaii; IA, Iowa; NM, New Mexico; UT, Utah.
Some additional aspects of the dataset are worth discussing. We do not observe the actual date of surgery and only capture surgeries that were part of the initial course of treatment and performed within 4 months after diagnosis. Therefore, it is possible that some surgeries are missed, which could inflate the variance estimates; since we observe significant effects, this has no meaningful impact on our main inference. Also, some of the reconstruction surgeries for women diagnosed in 1998 may have been performed in 1999, after that WHCRA went into effect. If so, this would result in underestimating the law's effect in the treated states (i.e., our estimate would be a lower bound of the full effect). Also, SEER provides data on only a few states that we could include for the analysis. Thus the representativeness of our results can only go as far as the representativeness of the SEER Registry goes. Another limitation is that earlier state mandates did not apply to self-insured employers. We would expect the WHCRA to have an effect for women in employer self-insurance plans in states with previous coverage laws. However, we do not have data on patient insurance status and are unable to exclude women covered in self-insurance plans. This would also contribute to estimating a lower-bound effect in the DD model, as the WHCRA's effect on women in self-insurance plans would be differenced out. Lastly, SEER data only have information on breast reconstruction use during 1998–2002, which limits our ability to examine long-term effects on utilization.
In theory, any mandatory coverage policies may also create potential negative effects that may result from employers or individuals deciding to drop health insurance coverage due to increasing insurance premiums and health care costs. We were not able to test such hypothesis in our study due to not observing insured status of patients, but we believe such incidence may be rare, particularly in the case of reconstruction surgery. Also even if such a phenomenon existed, it should not bias our DD estimate of the average WHCRA effect on the treated states, as insurance status changes because of the WHCRA would be on the causal pathway between the policy and use of reconstructive surgery. Similarly, any potential effects of the WHCRA on choice of mastectomy over lumpectomy would have no consequence for our study, as our analysis of reconstruction surgery is conditional on undergoing mastectomy.
Our study provides interesting findings about associations of demographic and clinical characteristics with the use of reconstruction surgery and about differences in utilization between states. Consistent with existing literature, our study finds significant racial/ethnic disparities in breast reconstruction utilization. 6,17 Very little is known about the underlying reasons for such disparities, which need to be further studied. Future research aimed at evaluating if the WHCRA had similar or heterogeneous effects on use of reconstruction surgery by race/ethnicity is important for determining if this law helped to reduce or instead exacerbated these racial disparities if at all. Such an analysis would be informative for designing other policy interventions to reduce similar or related disparities. Our model also shows that married women were more likely to undergo reconstruction. Future research is needed to explain this association. Patients who had radiation were less likely to have breast reconstruction. Breast reconstruction is often not considered an optimal procedure for patients who require radiation therapy, and their physicians may discourage this surgery. Finally, examining specific mechanisms that contribute to the extensive variation in utilization observed between certain states (independent of the WHCRA) in future research could also identify pathways for other policy interventions in order to further improve access and reduce disparities in utilization.
Conclusions
The use of breast reconstruction after mastectomy significantly increased after the WHCRA. Any threats to the validity of the DD model suggest that at a minimum, our estimates are lower bounds of the real policy effect.
Footnotes
Author Disclosure Statement
No competing financial interests exist.