
Abstract
Aortic stenosis is the commonest valve defect in the developed world and is associated with a high mortality once symptomatic. There is a difference in the way that male and female hearts remodel in the face of chronic pressure overload: women develop a concentrically hypertrophied, small cavity left ventricle (LV), whereas men are more prone to the development of eccentric hypertrophy. At a cellular level, there is an increase in collagen and metalloproteinase gene expression in males suggesting a different regulation of extracellular volume composition according to sex. Male hearts with aortic stenosis appear to have more fibrosis than their female comparators. The trigger for this appears to be in part related to estrogen receptor signaling, but other factors such as renin–angiotensin activation, nitric oxide, and circulating noradrenaline levels may also be implicated. Treatment options include surgical valve replacement (SAVR) and more recently transcatheter aortic valve replacement (TAVR). Female sex may be a risk factor for adverse outcome following SAVR and conversely appears to confer a survival advantage when undergoing TAVR. Whether the lower mortality seen following TAVR in women compared with men (despite their increased age and frailty) reflects their longer life expectancy, smaller annular size (and less post-TAVR aortic regurgitation), more favorable LV reverse remodeling, or more likely, a combination of these factors remains to be established.
Introduction
A
Surgical aortic valve replacement (SAVR) has been available since the 1960s 7 and was for a long time the only available treatment for patients with aortic stenosis. However, both advancing age and significant comorbidity markedly increase operative risk and postoperative morbidity, with prolonged intensive care unit and hospital stays, higher rates of stroke and cognitive impairment, and a longer postdischarge recovery time, 8 leading to a reluctance to operate on those deemed to be high risk. Finally, there are a group of patients such as those with porcelain aorta or a hostile mediastinum from previous radiotherapy in whom surgery is not technically possible. All these factors mean that there are a substantial number of patients who are declined SAVR. This was evident in the EuroHeart Survey, which identified that 33% of all patients with symptomatic AS remained untreated despite their very poor prognosis. 2 Recently, transcatheter aortic valve replacement (TAVR) has become a viable alternative in the treatment of inoperable or high-risk patients with severe AS.
Historically, women have a worse prognosis with asymptomatic and symptomatic AS when compared with men. This can be partly explained by later onset of symptoms, lower referral rates, and lower rates of surgery. 2,9,10 While female sex is identified as a risk factor in cardiac surgery (as recognized by the European System for Cardiac Operative Risk Evaluation score [EuroSCORE] 11 ), the relationship of female sex on outcomes after SAVR is subject to conflicting data. 12 The impact of sex on outcomes following TAVR is still under scrutiny; however, there appears an emerging trend for improved survival in females over males.
In this article, we seek to review the differences in aortic stenosis patterns of left ventricular (LV) remodeling, fibrosis, and outcomes following aortic valve intervention according to sex.
Methods
For the purposes of the review, a systematic literature search was performed using MEDLINE and EMBASE for studies published between January 1, 1980, and May 31, 2014 including aortic, stenosis, operative, surgical, transcatheter, outcome, LV remodeling, LV hypertrophy, LV mass, and sex as subject headings. The authors reviewed all abstracts and titles to identify those suitable. Large-scale trials were identified from meta-analyses and systematic reviews.
Pathogenesis of aortic stenosis and its effect on the myocardium
Aortic stenosis can be defined as obstruction to blood flow at the level of the aortic valve leading to an increase in LV afterload. The majority of older patients presenting with AS have trileaflet valves of equal size and shape of each cusp (Fig. 1), whereby there is an equal amount of shear stress distributed to each valve leaflet, with blood flow directed centrally through the aortic valve. Over time, the valve leaflets become progressively calcified and fibrosed with reduced systolic excursion and narrowing of the valve orifice. Although this calcific AS was traditionally felt to be purely a degenerative phenomenon, there is an increasing body of evidence to suggest that the process has an inflammatory 13 and genetic component. Congenitally abnormal valves (the most common being a bicuspid valve affecting around 1%–2% of the population) are prone to premature degeneration due to unequal shear stresses on the leaflets. Patients with bicuspid aortic valves typically experience symptoms in their fifth and sixth decades of life, with trileaflet valves degenerating in the eighth and ninth decades.

Transesophageal echocardiography demonstrating
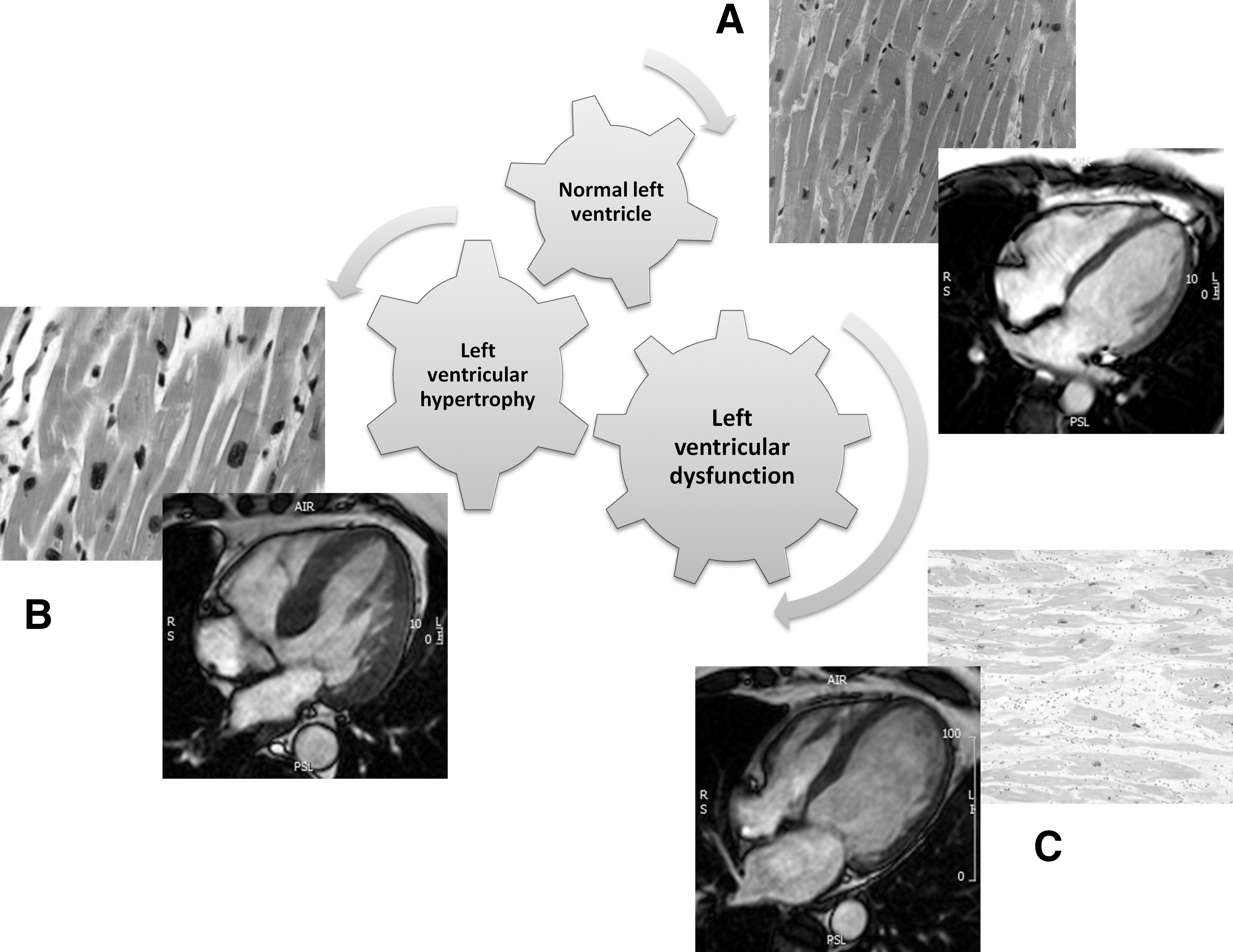
Cardiac remodeling, defined as “genome expression, molecular, cellular, and interstitial changes that are manifested clinically as changes in size, shape, and function of the heart after injury,” occurs in the pressure-overloaded heart of severe AS. 14 LV hypertrophy (LVH) is almost ubiquitous in severe AS, reflecting myocardial adaptation to chronic elevation of afterload. Increased LV mass is associated with adverse events. 6 Initially the LV adapts to the increase in wall stress by increasing myocyte size, allowing maintenance of ejection fraction but eventually progressive LV dysfunction occurs, initially affecting diastolic and then systolic function due to myocyte degeneration (a combination of apoptosis and oncosis) (Fig. 2). Patterns of hypertrophy can be concentric, eccentric, or asymmetric, and the degree of hypertrophy seen does not appear to correlate with severity of AS 15 but may be more closely matched to valvuloarterial impedance (Z VA), a global measure of afterload. 16
Sex-related differences in LV remodeling in aortic stenosis
In the normal heart, there are macroscopic and physiological differences between sexes. Due to their smaller body size, women have smaller hearts and therefore a lower stroke volume than men. Women have higher LV torsion and circumferential shortening compared with males due to an inherent difference in cardiac shape and fiber orientation. 17 Women have reduced sympathetic tone, as reflected by lower peripheral vascular resistance and increased parasympathetic tone in relation to men. Other differences include lower circulating levels of red blood cells (reflected in a lower hematocrit level), noradrenaline, and plasma albumin in females, alongside the obvious difference in hormonal profile. 18
The LV responds differently to chronic pressure overload in males and females. Women are found to have lower indexed LV mass, less wall tension, increased transvalvular gradients, higher pulmonary artery pressure, and better LV ejection fraction (LVEF) than their male counterparts. 19 –25 Women develop a concentrically hypertrophied, small cavity LV, 26 and men are more prone to the development of eccentric hypertrophy 19,27,28 (Fig. 3).
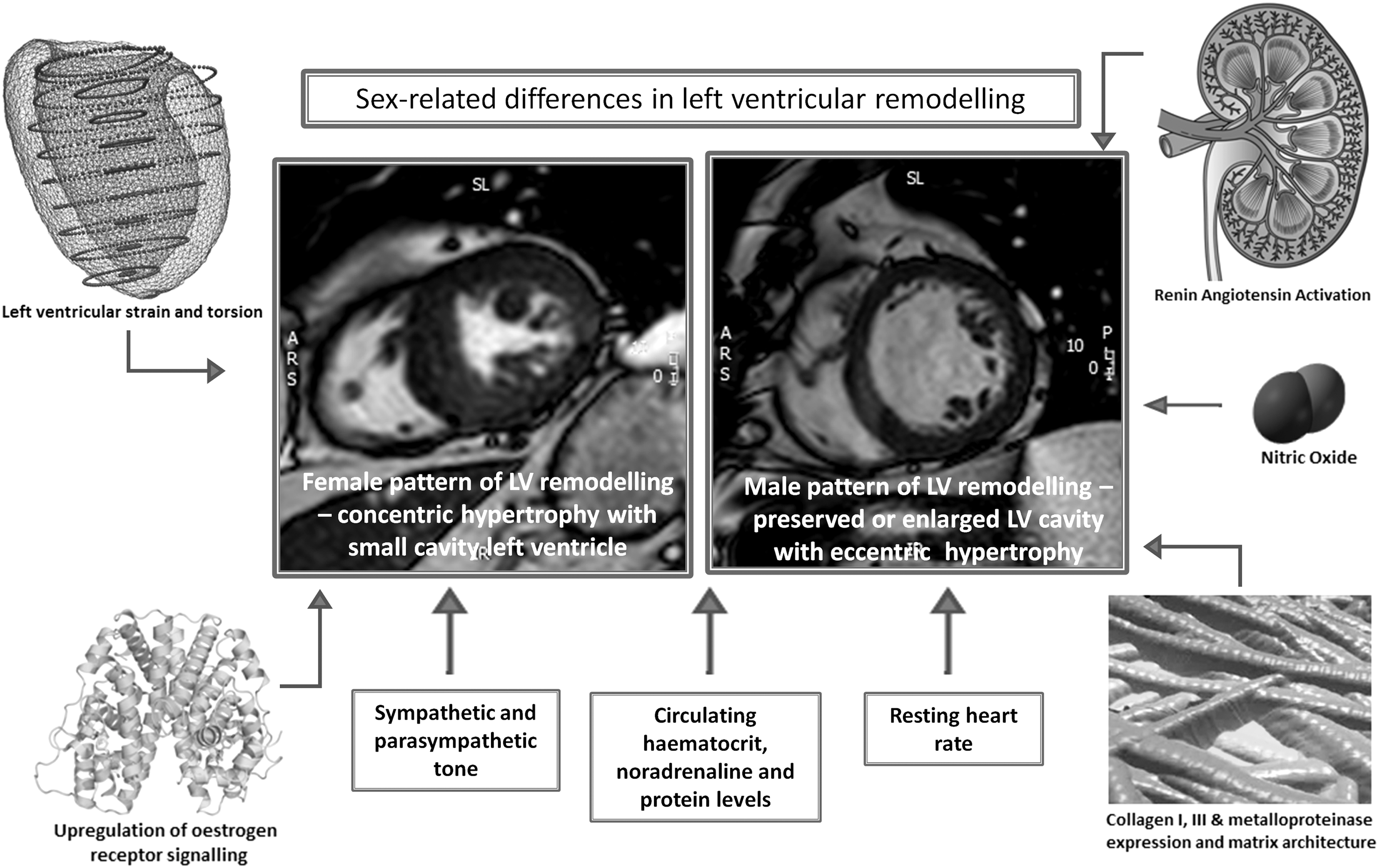
Potential mechanisms for differing patterns of LV remodeling between sexes in aortic stenosis.
Cellular, molecular, and neurohormonal mechanisms for differences in LV response to pressure overload according to sex
The physiological and biochemical basis for myocyte function is different according to sex. Males with severe AS are thought to have increased collagen 1, collagen 3, and metalloproteinases even in the context of normal LVEF. 29 There is increased upregulation of profibrotic genes and fibrosis in male rodent hearts compared with female rodents following aortic constriction. 30 Petrov et al. 31 evaluated biopsies from 10 human hearts with severe AS and compared them with normal controls. Men with AS had higher levels of collagen 1, collagen 3, and matrix metalloproteinase-2 gene expression compared with females with AS or controls, and this correlated with the degree of hypertrophy and changes in LV geometry. This suggests a different regulation of matrix synthesis and make up of extracellular volume according to sex. To further explore this altered extracellular volume in men, the group compared rat cardiac fibroblasts treated with 17β-estradiol and found a downregulation of collagen 1, collagen 3, and mRNA levels in female rat fibroblasts but increased expression in male rat cells. This is in keeping with the finding that in aging hearts without AS, there appears to be more fibrosis in male hearts. 32 Women with AS may therefore develop a different form of remodeled hypertrophy distinguished by less fibrosis in the heart.
Villari et al. 20 noted that interstitial fibrosis was more marked in male hearts with AS when compared with female hearts and those of controls without valvular disease. There was no relationship between total collagen volume and systolic function; however, there was an inverse relationship between “cross-hatching” (orthogonal collagen fiber meshwork) and LV systolic function. Those with increased cross-hatching also had stiffer hearts. In animal models male rats were found to have depressed cardiac reserve compared with female rats exposed to pressure overload (aortic banding) despite similar levels of hypertrophy. 33 Therefore it appears that although an increase in the extracellular volume does not relate to reduced ejection fraction, once abnormal collagen architecture has developed, there is deterioration in systolic and diastolic LV function.
One theory related to the sex differences observed in LV remodeling is the impact of sex hormones on the heart. Estrogen receptors (ERs) α and β can be found in both male and female myocardium and are felt to be implicated in the development of myocardial hypertrophy, 34 with estrogen binding having genomic effects on gene transcription and nongenomic effects such as protein kinase activation, initiation of intracellular signaling cascades, and modulation of growth factor signaling. 35 It has been proposed that rapid signaling of the nongenomic ERα can provide protection from myocyte necrosis and apoptosis, at least in animal models. 36 An upregulation of nongenomic ERα signaling in postmenopausal females may explain the differences in LV remodeling in response to pressure overload in the female heart. The presence of circulating estrogen is not a prerequisite for recruitment of estrogen receptors to transactivate estrogen-responsive genes, explaining why sex-related differences may still be observed in the postmenopausal state where the level of circulating estrogen is diminished. 37 Van Eickels et al. 38 studied two groups of female mice with transverse aortic constriction following oophorectomy and replaced 17β-estradiol in one group. They found that the estrogen treated group had a reduction in myocardial hypertrophy at 4 and 8 weeks compared with the placebo arm. The treatment arm was also found to have increased expression of atrial natriuretic peptide compared with placebo. 38
Testosterone exhibits an anabolic effect on the myocardium inducing myocardial hypertrophy in animal models. 39 Estrogen modulates the renin–angiotensin system by decreasing renin and angiotensin-converting enzyme (ACE) synthesis and increasing angiotensinogen synthesis. It is well established in animal studies that this affects the hypertensive response but may also be implicated in differences in LV remodeling. 40 Sex-related differences in nitric oxide (NO) expression and activity may also play a role. In a rat model of pressure overload, cardiac NO synthase expression is regulated differently between sexes. Male rats subjected to aortic banding experienced more early LV dysfunction and LVH than their female counterparts which correlated with a greater early increase in cardiac NO synthase 1 expression in males. 41 Female hearts appear to release less norepinephrine in response to myocardial stress than male hearts. 42 Although a direct link is yet to be established, it is evident that there is a relationship between circulating catecholamine levels and the development of LVH in the pressure overloaded ventricle. 43 There appear to be sex-related differences in insertion/deletion polymorphism of the ACE gene which affects serum ACE activity in patients with AS. 44 In women, absence of DD allele is associated with a higher LV mass whereas the opposite is true for men, with higher LV mass correlating with the presence of a DD genotype.
Surgical aortic valve replacement
It is well established that aortic valve replacement for severe AS leads to an improvement in morbidity, mortality, and quality of life. 45 –47 Mechanical valve design has evolved over the decades, with newer bileaflet designs offering improved valvular hemodynamics and requiring lower levels of anticoagulation than earlier models. Bioprosthetic valves, usually fabricated from bovine or porcine pericardium, obviate the need for anticoagulation altogether and although less durable, are often the valves of choice in the elderly population. Patient–prosthesis mismatch (PPM)—a phenomenon where the orifice area of the implanted valve is too small for the patient body size—can be seen following aortic valve replacement and is associated with less regression of LV mass and adverse outcome. 48,49 Women, with their smaller aortic annuli, are at increased risk of this postoperative phenomenon. Stentless valves, which offer improved valvular hemodynamics, have been shown to be associated with more LV mass regression. 50 However, for those with a very small LV outflow tract, aortic enlargement surgery should be considered prior to valve implantation. 51
Transcatheter aortic valve replacement
TAVR is a novel technique first described in 2002, whereby a balloon expandable bovine or porcine pericardial aortic valve is delivered via a catheter usually from the femoral, subclavian, or apical approach. 52 The first randomized, controlled trial results (Placement of Aortic Transcatheter Valves, PARTNER B) were published in 2010 comparing best medical care with TAVR in those deemed inoperable, 53 demonstrating a dramatic reduction in 12-month mortality in those randomized to TAVR compared with those randomized to optimal medical management (30.7% vs. 50.7%), although at the expense of higher rates of cerebral and peripheral vascular complications. The trial not only highlighted the dismal prognosis in those with severe symptomatic AS, but also paved the way for the expansion of the technique to other patient groups. PARTNER A 54 randomized high-risk patients (defined as a society for thoracic surgeons [STS] score of ≥10%) with severe symptomatic AS to either SAVR or TAVR. At 12-month follow-up, TAVR was found to be non-inferior to SAVR in terms of mortality with differing periprocedural risks between the two groups. There was a significant increase in vascular complications at 30 days and a trend toward increased major stroke rate at 12 months in the TAVR arm. Conversely, in the SAVR arm, the rates of major bleeding and postoperative atrial fibrillation were significantly higher. A more recently published multicenter randomized control trial of 795 patients comparing balloon expandable TAVR with SAVR in high-risk patients demonstrated a significant survival advantage of TAVR over SAVR at 1-year follow-up (14.2% vs. 19.1%, p=0.04). 55 Real-world registry data confirms that TAVR is a safe and effective technique for inoperable or high-risk patients with severe AS. The U.S.-based Transcatheter Valve Therapy Registry of over 7000 patients (49% women) undergoing TAVR reported an in-hospital mortality of 5.5% and stroke rate of 2%. 56 As with SAVR, TAVR has been proven to improve quality of life at early and long-term follow-up in patients with severe AS. 45,57 Although the flow profile across TAVR is generally felt to be more physiologic than that of a surgically implanted valve, PPM can still be observed in a significant proportion (46.4%) of patients. Severe PPM (defined as an aortic valve area [AVA] of <0.65 cm2/m2) has been reported in up to 20% of patients following TAVR, although interestingly and in comparison with PPM following SAVR, this does not appear to impact on LV mass regression or long term survival. 49
Sex-related differences in outcomes and remodeling following surgical aortic valve replacement
The effect of sex on outcome following SAVR is difficult to accurately evaluate as most studies are retrospective comprising a heterogeneous group of patients including those undergoing concomitant bypass grafting (CABG). Surgery in women is usually more technically demanding due to smaller annuli size, increased need for aortic enlargement, and complications related to cardiopulmonary bypass. Also, women tend to be older and in a more advanced stage of the disease with greater frailty at the time of surgical referral. In the recently published multicenter Italian Observational Multicenter Registry (OBSERVANT) that enrolled 2108 patients undergoing TAVR and SAVR (some with concomitant CABG) across 101 heart centers, women represented 44% of the SAVR population. 10 Women were older, frailer, and more symptomatic than men with less peripheral and coronary artery disease (CAD). Baseline echocardiography demonstrated higher LVEF, more mitral regurgitation, higher transvalvular gradients, and lower indexed AVA in women with higher postoperative transvalvular gradients. Female sex was an independent predictor of risk-adjusted 30-day mortality following SAVR compared with males (3.7% female vs. 2.2% male, p=0.043, odds ratio [OR] 2.34). Women were more likely than men to undergo blood transfusions (OR 1.47), possibly due to a lower level of hemoglobin preoperatively. Duncan et al. 58 retrospectively analyzed 2212 patients undergoing isolated SAVR over a 9-year period. Although unadjusted in-hospital mortality appeared to be higher in females (3.5% females vs. 1.6% males), propensity matching did not find a significant difference in mortality between sexes. Women had shorter cardiopulmonary bypass and aortic cross clamp time, smaller prosthesis size, more tissue bioprostheses, and more aortic enlargement procedures than men had. Most other studies evaluating isolated SAVR have also failed to show a difference in risk-adjusted mortality according to sex, 59 –61 with a systematic review of 28 studies failing to demonstrate sex as a prognostic indicator. 62 Females, however, do appear to have an increased morbidity following SAVR; one recent study of 6809 patients undergoing SAVR found a higher rate of postoperative stroke in women compared with men (3% vs. 2.2%, p=0.031) and various studies have found that women receive more blood transfusions than men. 10,58,63,64
Although a systematic review of outcomes of SAVR in patients with AS found that sex did not impact on LV mass regression and change in EF, the studies analyzed were largely historic and included small studies. 65 More recent and larger studies can be seen in Table 1.
95% CI, 95% confidence interval; AVR, aortic valve replacement; CABG, concomitant bypass grafting; HR, hazard ratio; LV, left ventricle; LVMI, left ventricular mass index; TAVR, transcatheter aortic valve replacement.
The results are mixed and again contain a heterogeneous group of patients. At least in theory, females' smaller body size require smaller aortic valves which are associated with a higher postoperative transvalvular gradient and subsequently less LV mass regression. 70
Sex-related differences in outcomes and remodeling following transcatheter aortic valve replacement
Due to the fact that TAVR is a relatively new technique, few long-term data regarding sex differences are available and the findings are discordant. A subgroup analysis of the PARTNER A trial 54 suggested that women had improved outcomes after TAVR compared with SAVR, although it was unclear whether this effect was due to worse surgical outcomes or improved TAVR outcomes, or both. A more detailed substudy of this trial has recently been published. 71 The PARTNER A trial randomized 699 high-risk patients (42.9% female) with severe AS to either TAVR or SAVR. Women were older than men with less important comorbidities. They had higher transvalvular gradients but similar indexed aortic valve area. There was a non-significant trend to lower procedural mortality in women undergoing TAVR compared with those undergoing SAVR (6.8% vs. 13.1%, p=0.007) at the expense of higher stroke rates. Procedural mortality was significantly reduced in men undergoing TAVR compared with SAVR (6% vs. 12.1%, p=0.03) with no difference between the two techniques in terms of stroke. In both sexes, vascular complications were increased in the TAVR cohort and bleeding rates higher in the SAVR group. At 2 year follow up, all-cause mortality in the female TAVR group was significantly lower than the female SAVR group (hazard ratio [HR] 0.67), driven by a very significant reduction in women undergoing transfemoral TAVR, and no mortality benefit in those with a transapical access route. There was no survival advantage in men undergoing TAVR compared with SAVR at 2 years. A survival advantage at 1 year was also seen in women undergoing TAVR compared with those undergoing SAVR (HR 0.56, 95% confidence interval [CI] 0.33–0.95) in the randomized control trial by Adams et al. 55 This apparent survival advantage was not seen in men (HR 0.89, 95% CI 0.55–1.47).
In a prospective registry of 260 patients undergoing TAVR by Hayashida et al., 72 women were of similar age to men but with less coronary disease, a higher LVEF and lower EuroSCORE. On Cox regression analysis, women had an improved 1-year survival compared with males (76% vs. 65%); however, baseline characteristics between the two groups were not corrected for. Humphries et al. 73 recorded a prospective database of 641 patients undergoing TAVR over a 6-year period. Women pre-procedure were more frail but with less comorbidity and a higher LVEF than men. Vascular complications and the need for periprocedural blood transfusion were seen more frequently in women. There was improved survival in women at 2 years (72.5% in women and 61.7% in men, 95% CI 54.1%–68.3%). This mortality benefit was maintained even when demographic, clinical, and procedural factors were corrected for (HR 0.55). Buja et al. 23 studied 659 high-risk patients (55.8% female, mean age 81±6 years) with severe AS undergoing TAVR. At 1-year follow-up there was a 63% relative risk reduction in death, myocardial infarction, or major stroke observed in women. Reverse remodeling seen in the heart following TAVR may provide late but important differences in cardiac function in women pertaining to improved survival, as this mortality benefit was sustained when cardiovascular death alone was analyzed at 12 months (3% men vs. 0.4% women, p=0.048). More recently, Erez et al. 74 prospectively followed 224 high-risk patients (57% women) with severe AS undergoing TAVR for a mean of 17 months. Men had an independent 2.5-fold increased risk of death during 2 years of follow-up compared with women. In women, the presence of CAD was associated with a marked (>14 times) increase in mortality whereas in men the presence of CAD did not influence survival. The mechanisms for this finding are unclear; however, the study sample was too small upon which to formulate firm conclusions. It seems probable that preexisting coronary artery disease impacts unfavorably on long-term survival following TAVR. 75 Coronary artery disease was found to be a univariate predictor of mortality in a study by Dewey et al. 76 Although not specifically designed to demonstrate a sex-related difference, female sex did not appear to be an influencing factor. Furthermore, outcomes following concomitant CABG and SAVR have not found sex to be implicated as a predictor. 77 Additional larger studies are required to explore this apparent sex-based relationship before firm conclusions about referral practices in this group of patients can be established.
In one of the largest registries to date, women were found to have a similar 30-day mortality to men but an improved 1-year all-cause mortality (HR 0.75, CI 0.57–0.98, p=0.0346) despite being older. 78 The OBSERVANT registry also found no sex-related difference in 30-day mortality following TAVR, 10 with increased rates of vascular damage and blood transfusion in women as seen in other series. A propensity matched substudy of this registry 79 found comparable in-hospital mortality rates in females undergoing SAVR and TAVR with a higher transfusion rate, more renal and heart failure, and higher transvalvular gradients in females following SAVR and more postprocedural aortic regurgitation, a higher stroke rate, more vascular complications, and a higher permanent pacemaker insertion and percutaneous coronary intervention rate in women undergoing TAVR. The UK-based TAVR registry of 1627 patients (756 women) found no sex-related difference in 30-day or 1-year mortality, but again, women were found to have more vascular complications and less aortic regurgitation than their male counterparts. 80
Most studies have only evaluated high-risk patients undergoing TAVR, however, a prospective, multicenter comparison of intermediate risk patients (as defined by STS score of 3%–8%) undergoing TAVR and SAVR found that at 1-year follow up all-cause mortality was similar among both groups; however, women appeared to have an improved survival when undergoing TAVR compared with SAVR, endorsing the findings of the PARTNER A trial. 81 Other studies suggest no difference in all cause and cardiovascular mortality following TAVR according to sex, although it is clear that women receive more blood transfusions than men. 10,80,82 –85 To our knowledge, only one study to date has found female sex to be a predictor of adverse outcome at 1 year on Cox proportional hazard analysis. 86
Women have been found to have less significant (grade≥2) aortic regurgitation than men in several studies, 10,71,80,87,88 likely as a result of their smaller annular size. Significant aortic regurgitation is known to be associated with adverse outcome and this may play a role in apparent sex discrepancies. Differences in LV reverse remodeling and LVEF according to sex following TAVR may help explain this apparent survival advantage in women but has yet to be explored fully in the literature. Stangl et al. 69 assessed sex-related differences in LV reverse remodeling by echocardiography in a prospective cohort of 100 patients following TAVR. Women were older, smaller (both in height, weight and body surface area) and had a smaller aortic annulus size compared with men. They also had an increased LVEF, smaller common femoral artery size, lower cardiac output, and less comorbidity than men in keeping with previous registry reports. Although they found no sex-related difference in mortality, residual aortic regurgitation, pacing rates, or cardiovascular or cerebrovascular events at 3 months following TAVR, as with some of the SAVR studies, they did find that women had a significant improvement in ejection fraction following TAVR whereas men did not. A significant reduction in LV mass was seen in both sexes but to a greater degree in men. This study, to our knowledge, is the only study to have explored in detail the difference in LV remodeling following TAVR according to sex.
Conclusion
Aortic stenosis is a common condition associated with high morbidity and mortality if left untreated. LV adaptation commences with hypertrophy, progressing to heart failure and resulting in death in the absence of timely intervention. Sex influences the LV response to AS before and after valvular intervention and influences outcome. Women develop a concentric pattern of hypertrophy whilst men develop more eccentric hypertrophy in response to elevation in afterload. Possibly due to genetic and hormonal influences, women tend to develop less fibrosis than men, and this may be important when considering the outcomes of valvular intervention. Women may experience a higher morbidity following SAVR and seem to survive better than men following TAVR. Whether the lower mortality seen following TAVR in women compared with men (despite their increased age and frailty) reflects their longer life expectancy, smaller annular size (and less post-TAVR aortic regurgitation), more favorable LV reverse remodeling, or more likely a combination of these factors remains to be established.
Footnotes
Author Disclosure Statement
No competing financial interests exist.