
Abstract
Background:
Some cancer diagnoses and treatments can place patients at risk for infertility. The American Society of Clinical Oncology recommends that health care providers address the possibility of infertility with cancer patients who are treated during their reproductive years; however, research suggests that many providers do not disclose the risk of infertility to their patients. This study examines adolescent/young adult (AYA) cancer survivors' use of and costs for fertility preservation (FP) over time.
Methods:
The study included 550 AYA cancer survivors diagnosed at the ages of 15 and 39 years between 2006 and 2012. Logistic regression analyses and chi-squared tests were conducted to identify factors associated with FP use, barriers, and expenses.
Results:
One hundred eighty two (33%) of the AYA survivors took steps to preserve their fertility. Men, survivors who did not have children, those who received chemotherapy, and those who lived in the Northeast (vs. the South) were more likely to have FP. The majority of men using FP used sperm banking (99%), whereas women used egg preservation (40%), embryo preservation (40%), and other methods (37%). On average, women paid more for FP than men (p < 0.001); however, costs for women significantly declined over time (p = 0.021).
Conclusions:
The study points to other areas for research in women's health, including the development of educational interventions with patients and providers to reduce gender disparities in FP and ensure timely patient–provider discussions related to fertility issues.
Introduction
I
In 2006, the American Society of Clinical Oncology (ASCO) released guidelines for cancer-related fertility issues, recommending that health care providers address the possibility of infertility with cancer patients who are treated during their reproductive years (or with parents or guardians of diagnosed children) and should make a referral to a reproductive specialist for those who are interested in FP. 6 Cancer survivors who receive counseling on fertility concerns and options have shown greater knowledge regarding FP, 7 less regret, and higher quality of life. 1
Despite the ASCO guidelines, many cancer patients do not receive information about FP. One study found that only 12% (85 out of 697) of cancer patients recalled receiving FP counseling. 8 In a study of female cancer survivors who received cancer treatment that could affect their fertility, Letourneau and colleagues 1 found that only 61% of women were counseled by their oncology team about FP with even fewer (5%) receiving counseling by fertility specialists, resulting in only 4% of women in the study taking steps to preserve their fertility.
Some research suggests gender disparities in FP referrals and use among AYA cancer patients. Pediatric oncologists have reported referring male pubertal cancer patients to fertility specialists prior to treatment much more frequently than female pubertal cancer patients (46% vs. 12%, respectively, referred >50% of the time). 9 In a study of adult cancer survivors in Sweden, men were more likely than women to receive information about the potential impact of cancer treatment on their fertility (80% vs. 48%) and information on fertility preservation (68% vs. 14%). 10 Perhaps as a result, while 54% of the men in this study used FP, only 2% of the women did so. 10
Since the 2006 ASCO guidelines, 6 the development of new guidelines and innovations has the potential to impact the accessibility and use of FP for women. For example, in 2008, the American Academy of Pediatrics released guidelines prompting physicians to consider the impact of cancer treatment on patients' fertility and to consider FP for children and adolescents undergoing treatment that could adversely affect their fertility. 11 In 2013, ASCO updated their 2006 guidelines to include more information on cancer treatments that could affect fertility and additional information to help oncologists assess their patients' risk of infertility. 12 The updated guidelines also recommended that all oncology healthcare providers, not just medical oncologists, should be prepared to discuss infertility risks. Finally, the new guidelines also acknowledged egg freezing as a viable preservation option for patients. This addition was prompted by the American Society for Reproductive Medicine's 2012 decision to recategorize egg freezing as first line fertility treatment instead of experimental treatment. 13
Further research is needed to examine gender differences in FP use and associated barriers and costs among a national sample and whether these have changed over time. The purpose of the current study is to examine AYA cancer survivors' use of FP, identify barriers to preserving fertility encountered among this population, explore possible gender differences in FP use, and examine potential changes in FP use and costs among this population over time.
Materials and Methods
Survey design
In 2012, with support from RTI International, the Livestrong Foundation fielded the Livestrong Survey from June through December. Livestrong developed the majority of the instrument using questionnaire items from the Medical Expenditures Panel Survey: Experiences with Cancer Survivorship Supplement. Other relevant questionnaires, such as the Health Information National Trends Survey, were reviewed, and relevant questions were added or adapted. In addition, input was gathered from cancer survivors and experts in survey methodology and oncology to develop new questionnaire items, which were subsequently tested through cognitive interviewing with a small number of cancer survivors. The Livestrong Survey asked people diagnosed with cancer about their practical concerns, as well as other issues such as fertility and talking to children about their diagnosis. The Western Institutional Review Board reviewed and approved the Livestrong Survey.
The 2012 Livestrong Survey was fielded exclusively online and was available on Livestrong.org. Livestrong constituents were notified about the survey through emails and Twitter and Facebook posts and asked to promote the survey Additionally, Livestrong's partner organizations (e.g., the American Cancer Society) and state cancer coalitions shared information about the survey with their constituents.
Those who were interested in responding to the survey were directed to the Livestrong survey's landing page. The survey was voluntary and anonymous. As no identifying information was gathered from respondents, there is the potential that the survey could have been completed by the same person more than one time. However, the extensive length of the survey, which was 157 items, reduces the chance of that an individual would choose to complete the survey more than once.
Measures
Respondents were asked whether they had taken steps to preserve their fertility before treatment began and if not, why they had not. In addition, respondents using fertility preservation were asked to indicate which fertility preservation option they used before beginning treatment (sperm banking, egg preservation, embryo preservation, ovarian tissue freezing, testicular tissue freezing, or other) and how much they have had to pay for fertility-related expenses, including initial and annual fees and other out-of-pocket costs. Other questions included whether they had tried to get pregnant/father a pregnancy since cancer treatment ended and whether that attempt had been successful. Demographic information, including gender, age, race/ethnicity, income, education, employment, marital status, sexual orientation, and insurance coverage, was also gathered. In addition, respondents were asked about their history of cancer (e.g., year of diagnosis, age at diagnosis, type of cancer, and type of treatment received).
Participants
A total of 6,383 cancer survivors completed the 2012 Livestrong Survey. Given that the ASCO recommendations on FP were released in 2006, 6 the sample was restricted to respondents diagnosed with cancer since 2006 (n = 3,984). Among these respondents, 1,025 were AYA cancer survivors (diagnosed between the ages of 15 and 39 years). Respondents were excluded from the analyses if they lived outside the United States (n = 202), did not respond to the survey items on taking steps for FP (n = 5) or on gender (n = 6), and/or indicated they were not interested in having any/any more children (n = 264). A final sample of 550 AYA cancer survivors (225 men and 325 women) was included in the analyses.
Statistical analyses
Frequencies and percentages were computed for survey items on whether the survivor took steps to preserve his/her fertility before beginning cancer treatment, the types of methods used, amount of money spent, and reasons for not preserving fertility. Chi-squared tests were conducted to compare reported barriers to FP across demographic groups based on gender and age at diagnosis. Respondents were divided into two epochs based on year of cancer diagnosis (2006–2009 and 2010–2012) to examine possible changes in FP practices over time. A logistic regression model was computed to identify subgroup differences in FP based on epoch, demographics, and cancer-related factors. Similarly, a linear regression model was conducted for the amount paid for FP by these factors.
All analyses were weighted to represent the United States' national population of cancer survivors based on estimates from the Centers for Disease Control and Prevention's 2011 Behavioral Risk Factor Surveillance System. 14 Weights were developed using a calibration weighting procedure as implemented in the SUDAAN® survey analysis software. 15 The weight adjustment included race/ethnicity and gender as the covariates in the calibration model.
Results
Participant characteristics
Most respondents were white (81% men, 74% women) and did not have children at the time of diagnosis (81% men, 74% women) (Table 1). The mean age at first diagnosis was 28 years for men and 30 years for women (range 15 to 39 years). The largest percentage of men reported receiving both chemotherapy and radiation (46%), while among women, 43% received radiation only and 31% received chemotherapy and radiation. The most common cancer types among men were genito-urinary (52%) and hematologic (20%); the most common cancer types among women were breast (32%) and hematologic (23%). The sample was geographically diverse with approximately 20%–30% of the sample in each of the four U.S. Census regions (West, Midwest, South, and Northeast).
Total sample sizes: males, n = 225; females, n = 325.
Sample sizes for survivors who took steps to preserve fertility: males, n = 114; women, n = 68.
Number of missing values by item: race, n = 3; had children, n = 2; treatment type, n = 2; cancer type, n = 1; geographic region, n = 9; method, n = 14; and amount paid, n = 32.
Fertility preservation use
A total of 182 (33%) AYA cancer survivors in the sample took steps to preserve their fertility. Male survivors were significantly more likely to take steps to preserve their fertility than female survivors [49% vs. 22%; chi-squared (1) = 28.50, p < 0.001] (Table 1). Based on the logistic regression model, the following subgroups were more likely to take steps to preserve their fertility: men, did not already have children, had chemotherapy (either alone or in combination with radiation), and lived in the Northeast (vs. South) (Table 2). There was also significant variation in FP by cancer type: those having breast or genito-urinary cancers were most likely to take steps to preserve their fertility in comparison with those with hematologic cancers. Controlling for demographic- and cancer-related factors, there was no significant difference in FP across the two epochs (2006–2009 vs. 2010–2012).
Total sample n = 534.
Odds ratios are adjusted for gender, year of diagnosis, age at diagnosis, race, had children, treatment type, cancer type, and geographic region.
CI, confidence interval; OR, odds ratio; REF, reference category.
Among participants who did not take steps to preserve their fertility, the most commonly reported reasons among men were the cost (27%) and not having enough time (25%) (Fig. 1). Women were most likely to report they did not have enough time (39%), cost (24%), and other reasons (26%) when not taking steps to preserve fertility. A total of 28% of men and 33% of women indicated reasons related to lack of information, including that they did not have information about FP options before treatment began, did not have information about risks to their fertility, did not know what steps to take, or did not know where to receive services. Men were significantly less likely than women to indicate lack of time before treatment [chi-squared (1) = 6.66, p < 0.01] or that they were ineligible [chi-squared (1) = 4.06, p = 0.04] as reasons for not taking steps to preserve their fertility. There were no significant differences in reasons across the age groups (Fig. 1).
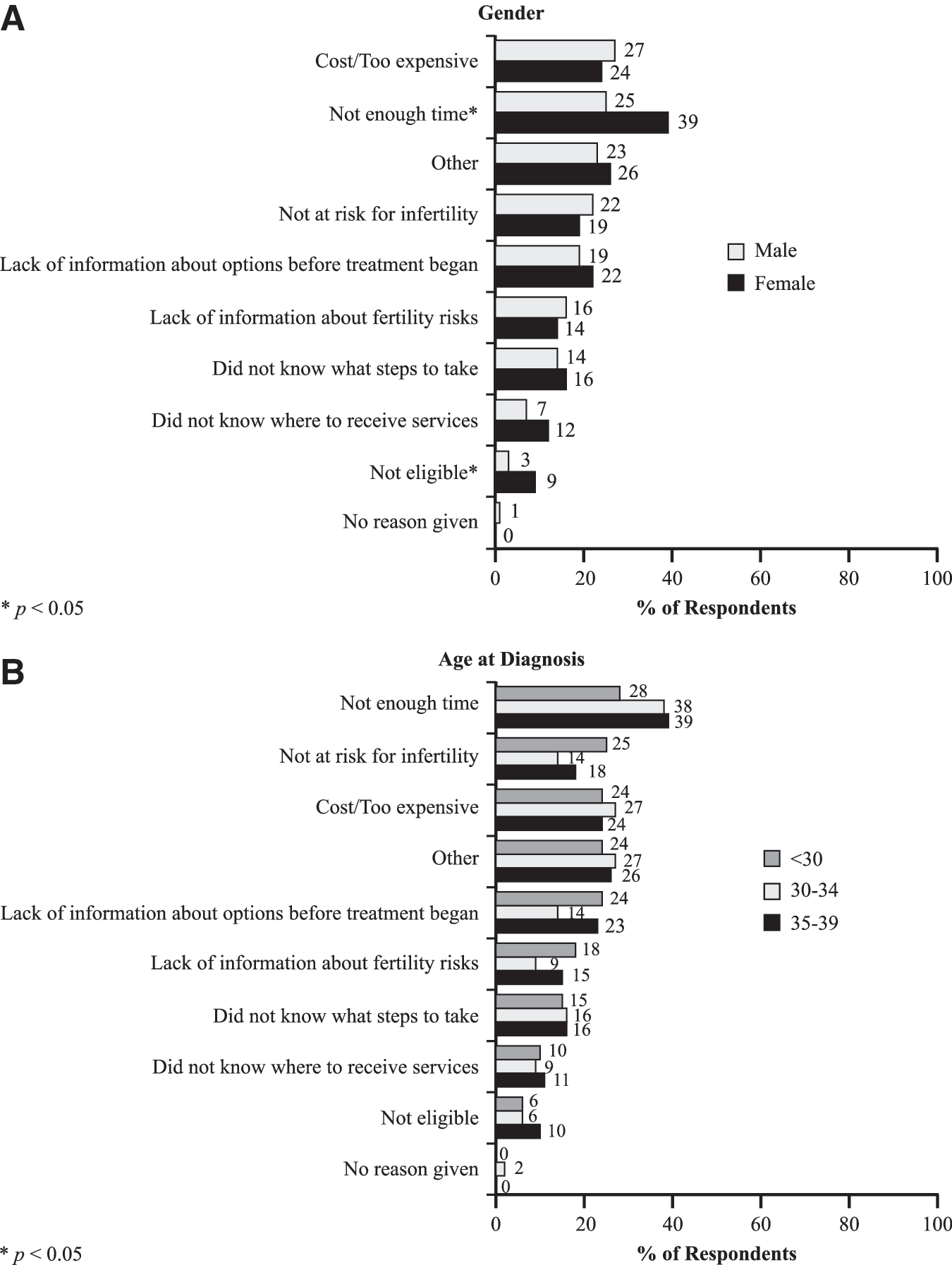
Reasons for not taking steps to preserve fertility by gender
Fertility preservation methods and costs
For respondents using FP methods, the vast majority of men used sperm banking (99%), whereas women used egg preservation (40%), embryo preservation (40%), and other methods (37%) (Table 1). Among respondents who took steps to preserve their fertility, the costs for FP services varied across respondents: less than $1,000 (41%), $1,000–$2,499 (29%), $2,500–$4,999 (9%), $5,000–$9,999 (8%), $10,000–$14,999 (6%), and $15,000 or more (7%). Females paid more for FP than males [chi-squared (5) = 96.62, p < 0.001] (Table 1). Among females, 24% paid $15,000 or more compared with only 2% of males.
Gender differences in amount paid for FP remained significant after controlling for demographic and cancer-related factors in the regression model [B(SE) = −0.99 (0.41), p = 0.017]. White respondents paid significantly more than nonwhite respondents [B(SE) = 0.86 (0.31), p = 0.007], while those who had children paid significantly less than those who did not have children [B(SE) = −0.69 (0.28), p = 0.015]. There was also variation in costs across some cancer types. The costs of FP decreased over time: Participants diagnosed more recently (2010–2012) paid significantly less than those diagnosed earlier (2006–2009) after controlling for gender, year of diagnosis, age at diagnosis, race, had children, treatment type, cancer type, and geographic region [B(SE) = 0.53 (0.23), p = 0.021]. The greatest cost reductions were seen among female survivors (Fig. 2). Although 41% of female survivors diagnosed in 2006–2009 paid $15,000 or more for FP, only 14% diagnosed in 2010–2012 paid this much.
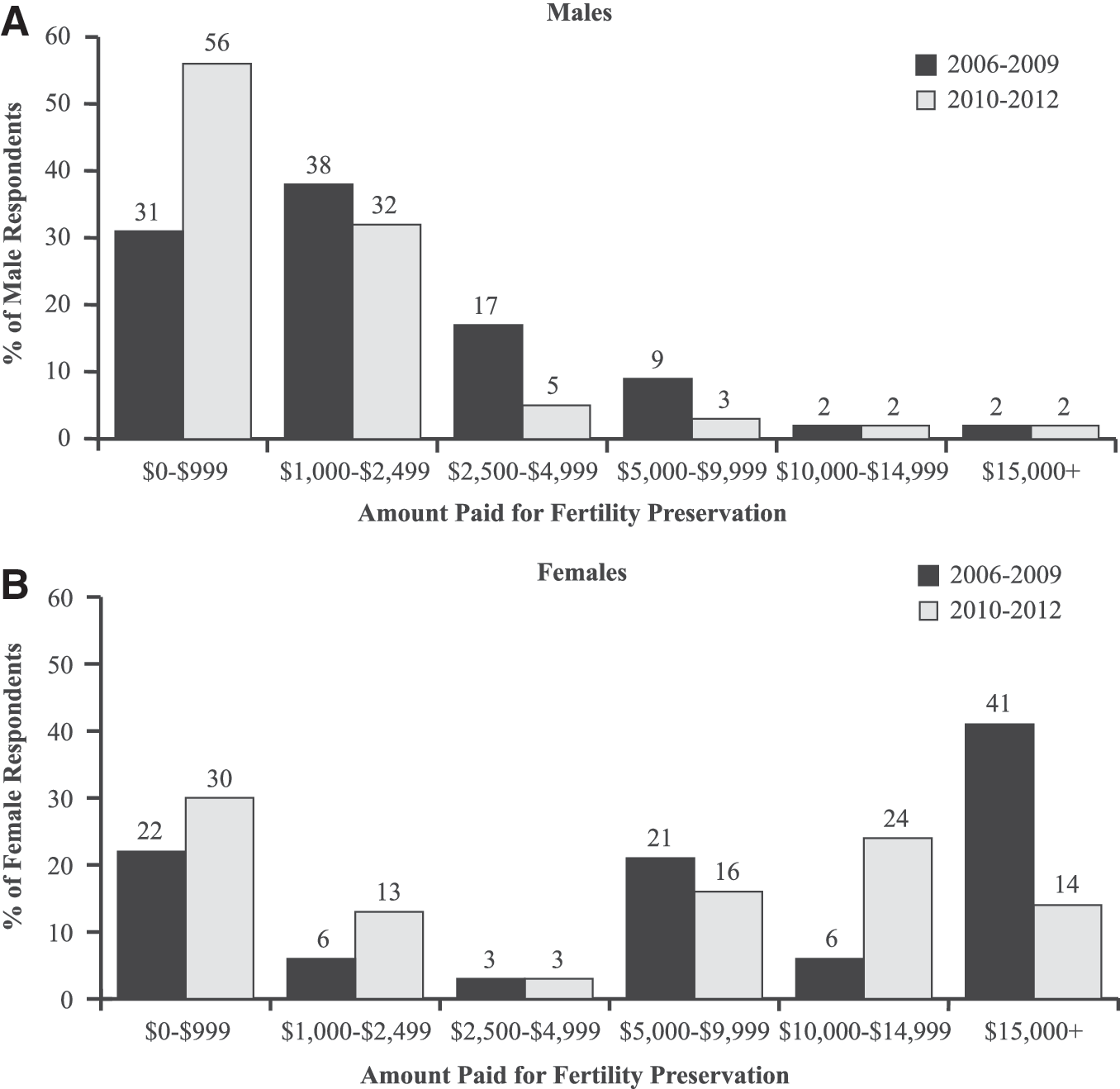
Amount paid for fertility preservation by gender and year of diagnosis.
To further understand the declines in costs of fertility preservation, we explored possible changes in use of specific fertility preservation methods over time (Fig. 3). Male survivors were consistent in use of sperm banking over time, with 100% of survivors diagnosed in 2006–2009 using this method compared with 98% of those diagnosed in 2010–2012. However, female survivors in the later epoch (2010–2012) were generally more likely to use egg preservation (53% vs. 28%) (although not statistically significant; p =0.058) and less likely to use other methods (21% vs. 53%; p = 0.025). To determine whether these changes explained the reduction in costs, we fit a regression model of amount paid for fertility preservation among female survivors by epoch, fertility preservation method, and demographics (gender, year of diagnosis, age at diagnosis, race, had children, treatment type, cancer type, and geographic region). There remained a significant reduction in costs over time [B(SE) =1.47 (0.65), p = 0.028].

Fertility preservation methods by gender and year of diagnosis.
Discussion
This study examined fertility preservation among a national sample of cancer survivors who were AYA at the time of their diagnosis, including respondents who did and did not take steps to preserve their fertility, the reasons for not doing so, and the costs incurred. Thirty-three percent of cancer survivors in our sample took steps to preserve their fertility before undertaking cancer treatment. While a strength of the survey is the inclusion of both male and female AYA survivors with a range of geographic locations, ages, and cancer diagnoses, a limitation is the use of an opt-in sample. The sample may not be representative of all the cancer survivors across the United States. When comparing the demographic profile of all cancer survivors in the United States in 2012, Livestrong survey respondents were more likely to be white and have higher incomes and education.To help alleviate any potential biases we have weighted the data to represent characteristics of the U.S. population, using a calibration weighting procedure that has been shown to reduce error and bias in estimates when combining data from a probability survey with an opt-in web survey. 16 –18
In our sample, male cancer patients were much more likely to take steps to preserve their fertility than female cancer patients (49% vs. 22%). This discrepancy is consistent with previous research findings that adolescent males are more frequently referred to FP specialists than females. 9,10 Among respondents who did not take steps to preserve their fertility, females were more likely to indicate there was “not enough time” in response to the question about why they did not take steps to preserve fertility before starting treatment. Egg and embryo freezing do require more time compared with sperm preservation, with the entire process generally taking from 2 to 6 weeks. However, for at least some of the female respondents there may have been sufficient time to pursue FP had providers addressed the topic in a timely manner. It is difficult to know whether the respondents' impressions that there was not enough time for FP before treatment are based on advice from health care providers and/or on the respondents' own sense of urgency to get started with treatment.
Although women paid more on average than men for fertility preservation, they were slightly less likely than males to cite cost as a reason for not taking steps to preserve their fertility (although the difference was not statistically significant). In addition, our study revealed a reduction in FP costs for women over time, even after controlling for demographic and cancer-related factors. Forty-one percent of women diagnosed in 2006–2009 paid $15,000 or more for FP while only 14% diagnosed in 2010–2012 paid that much. This difference in costs remained significant even after controlling for fertility preservation method. Further research is needed to fully understand the reasons for changes in FP costs over time.
Prior research suggests that women are less likely to be provided information about FP. 10 Information also played a role in FP for many of the women in our study with 33% of women indicating lack of information as the reason they did not take steps to preserve their fertility before undergoing cancer treatment (compared with 28% of men). Some of the reported information gaps included not having information about risks to their fertility, options for FP before treatment began, what steps to take, and where to receive services.
Given the potential barriers to FP for women—higher costs and the time needed for common methods—it is critical that providers routinely advise women about infertility risks and FP options in a timely manner. Educational interventions for both patients and providers are needed to close the gender gap in fertility preservation use by ensuring all cancer patients at risk of infertility risks are counseled about FP options. Continuing medical education provides an opportunity to reach providers with up-to-date guidelines, professional recommendations, and protocols related to FP.
Future studies could examine the reasons physicians are less likely to address FP with women. Qualitative research methods, such as focus groups and key informant interviews, can examine patient-provider discussions on FP, and the decision-making process for women with respect to FP to further understand the reasons for and how to address gender disparities.
In addition, the responsibility for raising the topic of FP does not have to rest solely on the shoulders of physicians. Other health care staff—including nurses, social workers, and patient navigators—may be well positioned to take on this responsibility and ensure that the option of FP has been introduced to every oncology patient of reproductive age. Electronic health records offer a platform for reminders and conversation prompts, and future research conducted with patients and their family members will inform the optimal time, initial messages, and mode of delivery to introduce the topic of FP.
Additionally, oncologists and health care providers could refer patients to cancer support organizations that are equipped to address gaps in information and help patients navigate the health care system to obtain FP services in a timely manner. For example, the Livestrong Navigation Services provides FP information and services to cancer patients, including assistance locating local fertility-related resources and accessing financial support.19 Additional resources for patients and families are available from the National Comprehensive Cancer Network20 and ASCO. 21 A multipronged approach may be needed to ensure that patients receive the information and support they need in time to make an informed decision about FP.
Footnotes
Acknowledgments
This research was supported by the Livestrong Foundation.
Author Disclosure Statement
No competing financial interests exist.