
Abstract
Background:
Chronic pain may be perceived differently according to gender and race, which may affect physical health and psychological wellbeing. We evaluated daily pain ratings in black women as compared to white women with provoked vestibulodynia (PVD).
Methods:
Seventy-one women (44 black, 27 white) rated pain severity with tampon insertion and sexual intercourse and recorded daily vulvar pain level on a visual analogue scale (0 = no pain to 10 = worst pain imaginable). In addition, they completed the Brief Pain Inventory (BPI) Interference Scale and Hamilton Anxiety Depression Scale (HADS). Multivariate analysis was performed to determine the effect of race on pain intensity after adjusting for functional impairment, affective distress and demographic characteristics.
Results:
Pain ratings from tampon insertion (6.37 ± 1.89 vs. 5.61 ± 1.98, p = .12) and sexual intercourse (6.28 ± 2.11 vs. 5.29 ± 2.50, p = 0.24) were similar, but daily vulvar pain (4.57 ± 2.27 vs 2.74 ± 2.43, p = <.01) was significantly higher in black women. BPI-interference scores were associated with small, but significant increases in tampon insertion pain (p = <.01, beta = .06 units) and daily pain (p < .01, beta = .10 units) and to a lesser degree with sexual intercourse pain when corrected for multiple comparisons (p = .05, beta = .06 units). Race had no effect on pain after adjusting for other variables.
Conclusion:
While race was associated with functional impairment, after accounting for this, race was not associated with level of vulvar pain with PVD.
Introduction
T
Besides gender-based differences in the pain experience, differences based on race, both historically and culturally, influence the pain experience. Blacks with chronic pain experience higher pain severity, depression, and functional impairment than whites with chronic pain. 2 –4 Thus, the gender-race intersection may expose black women to different levels of physical (e.g., pain severity, functional impairment) and psychological (affective distress, depression) sequela.
Three studies have conducted comparative analyses of the relationship between chronic pain and race in women, controlling for sociodemographic, affect and functional impairment. Jordan 5 found no differences in pain severity in 48 black and 52 white women seen in an outpatient rheumatology clinic; and, similarly, Eastwood 6 found no racial differences in chest pain severity in a cohort of 69 black and 397 white women undergoing coronary angiography for suspected ischemia. As well, Ndao-Brumblay 7 found that race did not predict pain severity in a retrospective analysis from a clinical database of 104 black women and 1,088 white women with chronic pain.
In addition to social, cultural, and psychological influences, biological factors may also contribute to gender-race differences in the pain experience, as blacks report lower pain tolerance and higher suprathreshold ratings of pain across different stimulus modalities; 8,9 and, compared to men, women report lower pain tolerance to thermal and pressure pain and lower pressure pain thresholds. 10 However, no studies have compared experimental pain between black and white women.
The effect of race on pain severity in vulvodynia, a chronic pain condition of the vulva, has not been studied. As with other chronic pain disorders, women with vulvodynia are more likely to have a history of depression and experience psychological distress than those without vulvodynia. 11,12 Provoked vestibulodynia (PVD), a subtype characterized by pain at the entrance of the vagina and painful sexual intercourse, 13 is particularly distressful and significantly affects a woman's quality of life. 11
The purpose of this study was to use the baseline data from a multicenter clinical trial to compare pain ratings on tampon insertion, sexual intercourse, and daily pain self-report among black and white women with PVD.
Materials and Methods
Institutional review board approval was obtained from the University of Rochester School of Medicine and Dentistry, Rutgers-Robert Wood Johnson Medical School and the University of Tennessee Health Science Center, and all subjects signed an informed consent before participation.
Participants
Baseline data were collected from women who were randomized to treatment in the multicenter clinical trial studying the therapeutic effect of gabapentin vs. placebo. Women were recruited from urban, suburban, and rural areas from ambulatory centers of the participating research sites, vulvovaginal specialty clinics, and through research study advertisements.
Women were 18 years of age or older, and experienced dyspareunia, pain to vulvar touch, or both for at least 3 continuous months (modified “Friedrich's criteria”). 14 They were required to demonstrate moderate to severe tenderness in the vulvar vestibule, which was greater than the score in the outer vulvar area or the score in the vagina on the cotton swab test during the pelvic examination and report an average pain level of 4 or greater (0 = no pain to 10 = worst pain imaginable) with two tampon insertions during a 2-week screening period.
Women were excluded from study participation if they had other vulvar conditions, including dermatoses, vulvitis, atrophic vaginitis or active vaginal infection, a prior vestibulectomy, were pregnant or at risk for pregnancy and not using a reliable birth control method for at least 3 months prior to entering the study, had any unstable medical or psychiatric condition, or used centrally acting medications, with the exception of the long term, stable dose use of selective serotonin reuptake inhibitors (SSRIs) for the treatment of depression or anxiety.
Four hundred twenty-eight women were prescreened by telephone interview, and 128 were screened at the research sites and completed the questionnaires. Eighty-three participants were eligible and completed daily diaries, and 71 were randomized to treatment. The number of participants recruited from each research site and the reasons for exclusion are depicted in Figure 1.
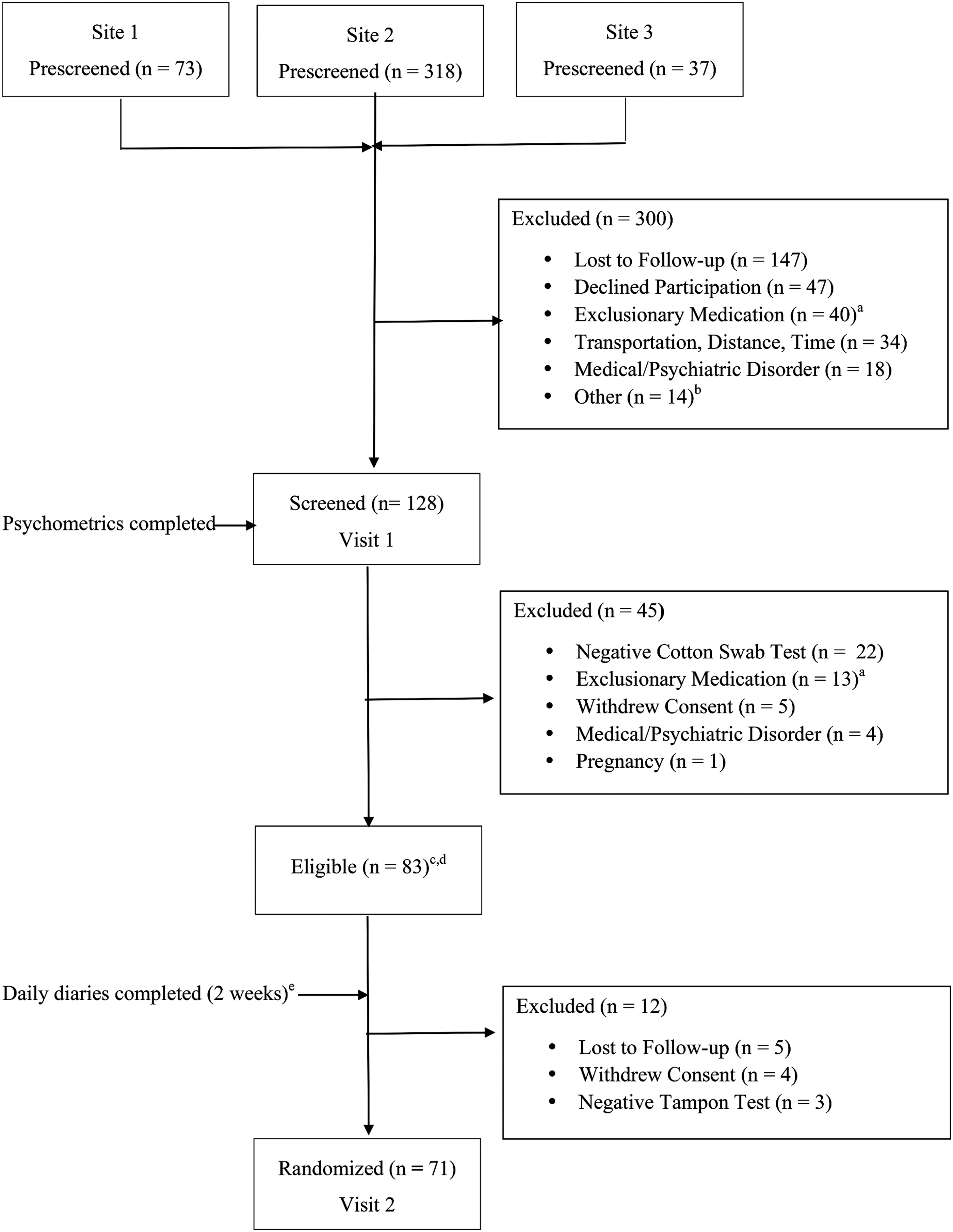
Subject enrollment flow diagram. aExclusionary medications included serotonin norepinephrine reuptake inhibitors (SNRIs), tricyclic antidepressants (TCAs), CNS stimulants, benzodiazepines, opiates, muscle relaxants, and topical lidocaine. Selective serotonergic reuptake inhibitors (SSRIs) used on a long-term basis were not exclusionary, and 2 subjects (1 black and 1 white) received them for the treatment of depression in the study. bOther exclusions included vulvar dermatoses, vestibulectomy, abnormal laboratory values, multiple allergies, previous use of study medication, gastric bypass. cSix subjects had vaginitis and entered the study after treatment. dTwo subjects were receiving topical hormone therapy at screening. One subject had ≥10 parabasal cells and vaginal atrophy at screening and entered the study after 6 weeks of topical hormone therapy. eSubjects were required to record the insertion of 1 tampon per week (total of two tampons) in their daily diary. A mean score of 4 or greater (11 point NRS) was necessary for randomization.
Pain Measures
Using a numeric rating scale (NRS, 0 = no pain to 10 = worst pain imaginable), subjects completed an electronic daily diary during a 2-week period that recorded pain from tampon insertion, coital pain (when intercourse was attempted), and average pain for the last 24 hours. Data were reported as mean ± standard deviation (SD) for each of the pain measures during the 2-week period. For subjects who did not have access to a computer, a paper copy of the electronic daily diary, along with written instructions was provided.
Tampon Test
The “Tampon Test” was used as the primary outcome measure because coital pain may be so intense that women may completely abstain from intercourse. Data have shown that the Tampon Test is an accurate, easily accessible, and cost effective primary outcome measure because it includes qualities of appropriateness of content, reliability, validity, responsiveness, and limited participant burden. 15
Subjects were provided with Original Regular Tampax Tampons (Proctor & Gamble Corp, Cincinnati, OH) supplied in standard cardboard applicators and instructed to insert one tampon per week during the 2-week screening period, to remove the tampon immediately after vaginal insertion, not to lubricate the tampon before insertion and to only use the tampon that was provided.
Coital Pain
Subjects reported daily whether they experienced sexual intercourse in the last 24 hours. The possible responses were 1—“No, too painful,” indicating the subject could not accept an approach to physical intimacy because of pain; 2—“No, not interested,” indicating the subject was not in the mood for sexual intimacy; 3—“No, no opportunity,” indicating that her partner was not available; and 4—“Yes,” meaning an attempt at sexual intercourse was made. If intercourse was attempted, the subject was asked to rate her level of pain. Coital pain has been used as an outcome measure in a number of efficacy studies. 16,17
24-Hour Pain
Subjects reported the average severity of vulvodynia pain over the last 24 hours in their daily diary.
Psychometric Measures
The Brief Pain Inventory (BPI) Interference Scale, a 7-item self-report measure, was used to assess the extent to which pain interfered with various components of functioning. 18 The seven categories of functioning include: general activity, walking, work, mood, enjoyment of life, relations with others, and sleep, whose mean comprises the Pain Interference Index. Items were assessed on 11-point numeric rating scales ranging from 0 (no pain) to 10 (worst pain imaginable). Observational studies have shown patients with chronic pain to report moderate impairment (5.6/10 to 6.6/10) on the BPI-Interference Scale. 19,20
The Hamilton Anxiety and Depression Scale (HADS) is a 14-item questionnaire consisting of anxiety (HADS-A) and depression (HADS-D) subscales that was used to measure psychological distress. 21 Each subscale contains 7 items with score ranges from 0 to 21, in which 0–7 is no distress, 8–10 is mild distress, 11–14 is moderate distress, and 15–21 is severe distress. Observational studies have shown chronic pain patients to report mild levels of anxiety (8.8) and depression (8.2) on these subscales. 19
Baseline scores on the BPI Interference Scale 18 and the HADS 21 were reported as mean ± SD.
Gynecologic Examination
The gynecological examination included cotton-swab palpation of 4 vestibular sites at the 1-, 5-, 7- and 11-o'clock positions and other areas of the external genitalia (i.e., labia minora, labia majora), commonly referred to as the cotton swab test, which constitutes the main diagnostic tool for vestibulodynia. 22 The cotton-swab test has been shown to be a reliable measure of vestibular pain with acceptable discriminant validity. 22 A standard bimanual palpation of the vagina, uterus, and adnexa was performed to rule out vaginismus and other forms of vulvar and/or pelvic pain. Visual inspection of the external genitalia and vaginal vault and collection of vaginal specimens were performed to determine if dermatological or infectious conditions were present.
Data Analysis
The data were analyzed using SAS version 9.3 (SAS Institute Inc., Cary, North Carolina). Difference between groups in age and scores on the HADS, BPI-Interference Scale, tampon insertion, daily pain, and sexual intercourse were analyzed by two-sample t-tests (mean ± SD), and differences in duration of pain and educational status were analyzed using Chi-square. Independent associations between pain ratings with ethnicity, age, education, pain duration, HADS, and BPI-interference were studied in multivariate analyses using linear regression. Statistical significance was set at the 1% level to adjust for multiple comparisons.
Results
Demographic characteristics
Seventy-one, self-identified as black (44) and white (27) completed the questionnaire. The average age of subjects was 37 years, with 46% having a college degree or higher and 61% having had pain of at least 5 years duration. Demographic characteristics were similar to those reported in population-based studies. 23 Black women were less likely to have completed college (p < .01), but there were no significant differences in age or duration of pain (Table 1).
One black subject and 1 white subject were being treated for depression with selective serotonergic reuptake inhibitors (SSRIs).
SD, Standard Deviation.
Two-sample t-test for equal variances (pooled).
Chi-Square.
HADS, Hamilton Anxiety Depression Scale (0 = no impairment to 42 = severe impairment).
HADS Subscales (0 = no impairment to 21 = severe impairment).
Brief Pain Interference Scale (0 = no disability to 10 = severe disability).
Numeric Rating Scale (0 = no pain to 10 = worse pain imaginable). Values are reported as mean ± SD during a 2-week period.
Univariate Analysis
All scores are expressed as mean ± SD. HADS scores were similar between black and white women (10.09 ± 6.87 vs. 8.52 ± 5.60, p = .32) and on the depression (3.75 ± 3.51 vs. 2.93 ± 2.99, p = 0.31) and anxiety (6.34 ± 3.98 vs. 5.59 ± 3.32, p = .42) subscales, respectively, indicating little to no impairment. BPI-interference scores were significantly higher in black women (4.27 ± 2.40 vs. 2.25 ± 2.17, p < .01), indicating mild functional impairment compared to minimal dysfunction in white women (Table 1).
Pain from tampon insertion (6.37 ± 1.89 vs. 5.61 ± 1.98, p = .12) and sexual intercourse (6.28 ± 2.11 vs. 5.29 ± 2.50, p = 0.24) were similar in black and white women, respectively, and were rated as moderate in severity. Black women reported significantly greater daily pain (4.57 ± 2.27 vs. 2.74 ± 2.43, p = <.01), which was reported as moderate in severity compared to mild severity described by white women.
Multivariate Analysis
All scores are expressed as mean ± SD. After adjusting for depression, functional impairment, age, educational status, and duration of pain, race had no effect on daily pain (p = .32) (Table 2), tampon insertion pain (p = .69) (Table 3), or pain with sexual intercourse (p = 1.00) (Table 4).
SD, Standard Deviation.
HADS, Hamilton Anxiety Depression Scale.
BPI, Brief Pain Interference Scale.
SD, Standard Deviation.
HADS, Hamilton Anxiety Depression Scale.
BPI, Brief Pain Interference Scale.
SD, Standard Deviation.
HADS, Hamilton Anxiety Depression Scale.
BPI, Brief Pain Interference Scale.
When adjusted for other variables, a unit increase in functional impairment was associated with 0.1 unit increase in daily pain (p < .01), and 0.06 unit increase in pain with tampon insertion (p = <.01), and an insignificant 0.06 increase in pain with sexual intercourse (p = .05) (Tables 2 –4). No other covariates were significant after adjustment.
Discussion
These data compared pain ratings on tampon insertion, sexual intercourse, and daily pain self-report among black and white women with PVD. Black women rated their daily pain almost twice as severe as white women, but after adjusting for age, educational level, pain duration, depression and functional impairment, race had no significant effect on pain severity. These findings are consistent with population-based studies when these variables were controlled. Compared to white women, black women with arthritic, 5 anginal, 6 and other forms of chronic pain 7 did not report their pain as more severe.
No differences were observed in pain severity with tampon insertion and sexual intercourse, even before adjusting for these confounders. The acute nature of provoked pain may be less likely to be influenced by socio-demographic or psychosocial factors.
Functional impairment, as measured by the BPI-Interference Scale, was greater in black compared to white women, and was associated with daily pain and pain with tampon insertion regardless of race in this study. Ndao-Brumbley, 7 Jordan, 5 and Eastwood 6 found that black women with chronic pain reported greater functional impairment and physical inactivity compared to white women, but did not measure whether functional impairment was an independent predictor of pain. Baker found that functional impairment was a significant predictor of greater pain intensity among 181 older black women with chronic pain, but did not compare findings to a white population. 24 Thus, unlike previous literature, we determined the independent effect of functional impairment after adjusting for race.
Functional impairment was associated to a lesser degree with pain from sexual intercourse when adjusted for multiple comparisons. It is possible that sexual intercourse pain may lead to a distinctly different pain experience than pain from tampon insertion or daily pain. However, pain ratings were similar between sexual intercourse and tampon insertion, suggesting that the tampon test was an appropriate surrogate measure of coital pain. It is also possible that our sample size was too small to detect a significant association, since only half of the subjects engaged in coital activity. Larger samples are necessary to determine whether there is a more robust association between functional impairment and all types of vulvar pain and whether this impairment predicts pain that is clinically meaningful.
It is also important to note that the BPI-Interference Scale is a generic measure of functional impairment and may not demonstrate responsiveness to the specific symptoms of vulvodynia. Validated, disease-specific measures are necessary to further explore this association. Finally, sexual intercourse pain outcome measures remain problematic in vulvodynia studies, since women refrain from coital activity due to dyspareunia.
Affective scores were similar between black and white women, and indicated limited to no impairment. An association was observed between affective scores and pain measures, but the association did not meet the criteria set at 1%, and the use of SSRIs had no bearing on this relationship. A history of depression has previously been demonstrated to predict vulvar pain. 11
Because this was a cross-sectional study, it was not possible to determine the directionality between functional impairment and pain ratings. Although functional impairment may have led to the worsening of pain, it is also possible that pain may have resulted in greater functional impairment. A longitudinal study would be necessary to determine the sequence of events.
The sample size is a limitation of this study. Other limitations include potential selection bias due to eligibility criteria that were part of the clinical trial, restriction of subjects to two ethnic groups, use of only three geographic locations and over-representation of subjects from a single site, so that our findings may not be generalizable a larger sample of women with PVD. However, use of standardized instruments, prospective daily ratings and a numeric rating scales are strengths of our study.
From our review of the literature, it appears that these are the first data to show that black women with PVD report more functional impairment with chronic vulvar pain and that functional impairment is associated with both pain from tampon insertion and daily pain ratings in both racial groups studied. In addition to evaluating vulvar symptoms, these data highlight the importance of assessing the mental and physical health of women with PVD, because diminished functioning has a tremendous impact on their psychological and social wellbeing and quality of life. Future investigations should focus on understanding why race appears to play a role in women with PVD.
Conclusions
From these data, there were no differences in pain ratings on tampon insertion, sexual intercourse and daily pain self-report in black and white women with PVD after adjusting for demographic characteristics, affective distress, and functional impairment. Functional impairment was highly associated with pain from tampon insertion and with daily pain. Clinicians should assess these factors when providing care for women with this chronic pain condition.
Footnotes
Acknowledgments
This work is supported by grant number R01HD065740 from the Eunice Kennedy Shriver National Institute of Child Health and Human Development (NICHD) and the Office of Research on Women's Health (ORWH), the University of Tennessee General Clinical Research Center (GCRC) and Depomed, Inc. who provided gabapentin extended release and matching placebo for the study. The content is solely the responsibility of the author and does not necessarily represent the official view of the NICHD, ORWH, GCRC or Depomed, Inc.
Author Disclosure Statement
No competing financial interests exist for any of the authors.