
Abstract
Background:
In the United States, cigarette smoking accounts for almost 20% of all deaths attributed to heart disease. More women than men die each year of cardiovascular diseases (CVDs). Women who smoke have shown to be at a higher risk of cardiac deaths. The current study aims to determine the trend in smoking prevalence among women with CVD and their utilization of smoking cessation agents from 2004 to 2011.
Materials and Methods:
This was a retrospective exploratory study using Medical Expenditure Panel Survey data from 2004 to 2011. All female respondents with any one cardiovascular condition were identified. Descriptive statistics were carried out to obtain the number of female patients with CVD, their smoking status, and their use of smoking cessation agents. Furthermore, disparities in smoking status and smoking cessation agent utilization with respect to race and ethnicity were studied.
Results:
Among total CVD patients, 53% were females, which corresponded to 25.3 million females in the United States. Around 12.3% among them were current smokers. Only 6.9% among these females used smoking cessation agents. Smoking trends in females were inconsistent throughout the 8 years. Overall, the trend showed a decrease in the percentage of female smokers, while use of smoking cessation agents remained low from 2004 to 2011. Whites and non-Hispanics had more current smokers and women using smoking cessation agents.
Conclusion:
The eight-year trend shows that the use of smoking cessation agents among females is very low, particularly among non-whites and Hispanics. This is of great concern and future efforts could focus on increasing the utilization of smoking cessation agents and collectively decreasing the risk of smoking in CVD by healthcare professionals.
Introduction
S
The use of smoking cessation agents is one of the most effective ways for women to quit smoking. 7 The risk of heart attack relapse and death from heart disease can be reduced by 50% or more if a person quits smoking. 4 In women, most of the health risks associated with smoking are reduced upon quitting smoking, and the risk of MI decreases virtually to the level of nonsmokers after about 2 years of smoking cessation. 8 A study by Wilson et al. supported this evidence by showing that the decrease in risk of mortality in patients with MI after quitting tended to be greater in women than men. 3 Considering the detrimental effects of smoking among women with CVD and the beneficial effects of using smoking cessation agents, the prevalence of smoking among women and their use of smoking cessation agents warrant further investigation. Research suggests that the risk of death from cigarette smoking continues to increase among women. 4 However, the prevalence of current smoking among women with CVD and their utilization of smoking cessation agents have been rarely studied. The current study aims to explore the yearly trend in smoking prevalence among women with CVD and their utilization of smoking cessation agents from 2004 to 2011 by using a national data set.
Materials and Methods
Study design and source of data
This was a retrospective exploratory study approved by the University of Toledo Institutional Review Board. Medical Expenditure Panel Survey (MEPS) was used for the purpose of this study, which is a publicly available data set frequently used for health service and public health research. 9 It includes a survey of noninstitutionalized individuals or their families, sampled from a nationally representative population across the United States. MEPS provides information on access to healthcare and healthcare utilization and expenditures, including inpatient stays, outpatient visits, emergency room visits, physician services, and prescription drugs. The data from the household component of MEPS were used. This component provides detailed information for each person on health conditions, health status, demographic characteristics, employment, healthcare access, healthcare use, satisfaction with care, medical expenditures, sources of payment, and insurance coverage. The survey is sponsored by the Agency for Healthcare Research and Quality and is administered every year. The survey has a rotating panel design, and each panel is subjected to five rounds of interviews over 30 months. Except for the first year, two panels are interviewed each year, and individual sampling weights are assigned to the participants in two panels to obtain a national estimate of population.
Data collection
Data from the MEPS's full-year consolidated medical conditions and prescribed medicine files from 2004 to 2011 were extracted for the purpose of this study. Full-year consolidated medical conditions and prescribed medicines files were combined for each year.
From medical conditions data files, all patients with CVD were identified using International Classification of Diseases, ninth revision (ICD-9) codes for each of the cardiovascular conditions. These cardiovascular conditions were identified according to the American Heart Association (AHA) definition of CVD. According to AHA, hypertension (ICD-9 code 401), hypertensive heart disease (ICD-9 code 402), hypertensive renal disease (ICD-9 code 403), MI (ICD-9 code 410), angina pectoris (ICD-9 code 413), coronary atherosclerosis (ICD-9 code 414), atherosclerosis (ICD-9 code 440), ischemic heart disease (ICD-9 code 411), heart failure (ICD-9 code 428), intracerebral hemorrhage (ICD-9 code 431), transient cerebral ischemia (ICD-9 code 435), and cardiac arrhythmia (ICD-9 code 427) constituted the broad category of CVDs. Smoking status of these patients with CVD was obtained from full-year consolidated data files. Patients who responded “Yes” for the question, “Do you currently smoke?” were considered as current smokers. Use of smoking cessation medications was identified among the current smokers, using the prescribed medicine files. From the earlier identified patients, female patients who smoked and used smoking cessation medications were identified.
The trend in the prevalence of smoking among women with CVD was explored from 2004 to 2011. Similarly, the utilization of smoking cessation agents was observed among the same population for 8 years and compared to smoking prevalence. This cohort of women was further divided according to race and ethnicity to study the effect of these characteristics on smoking status and the utilization of smoking cessation agents.
Data analyses
Descriptive statistics were used to ascertain the number of female patients with CVD, their smoking status, and their use of smoking cessation agents in each year.
The complex survey design of MEPS and nonresponse bias were adjusted by using sample weights for stratum, cluster, and individual persons. SAS version 9.3 (SAS Institute, Inc., Cary, NC) was used to accommodate for the complex sample design and weights.
Results
During the 8-year period from 2004 to 2011, there were around 477 million patients with CVDs. As shown in Table 1, among these CVD patients, 53% were females. This corresponded to an estimated 25.3 million females with CVD in the United States. The percentage of females with CVD ranged from 51% to 54% and consistently remained higher than the percentage among males in the 8 years. After diagnosis, there were around 67 million CVD patients who were current smokers, of whom nearly 46% were female. Of the total number of smokers, the percentage of female smokers ranged from 43% to 48.2% in the 8 years studied. The percentage of female smokers was highest in 2004 at 48.63%. There were 4 million smokers who were using smoking cessation agents, making up only 6% of the smokers with CVD; of them, 52.38% were females. The percentage of female smokers utilizing smoking cessation agents was consistently higher than that for males each year except for 2008. The percentage of females using smoking cessation agents ranged from 5% to 10% during the 8 years. The percentage of females utilizing cessation agents was the highest in 2007, at 10.18%. According to race, whites contributed to a larger proportion of female smokers than non-whites, and utilization of smoking cessation agents was higher in whites compared to non-whites (Table 2). An analysis of female smokers with CVD was conducted based on ethnicity, and it showed that most of the female smokers were non-Hispanic, and the average smoking cessation utilization was higher in non-Hispanics compared to Hispanics.
CVD, cardiovascular disease.
Figure 1 shows the trends of smoking and use of smoking cessation agents in females. Smoking trends among females were inconsistent throughout the 8 years. Overall, there was a slight decrease in the percentage of female smokers from 2003 to 2011. The number of female smokers showed an upward trend in 2007 and 2009, while showing a decrease in other years. After 2009, the number of female smokers continuously decreased until 2011.
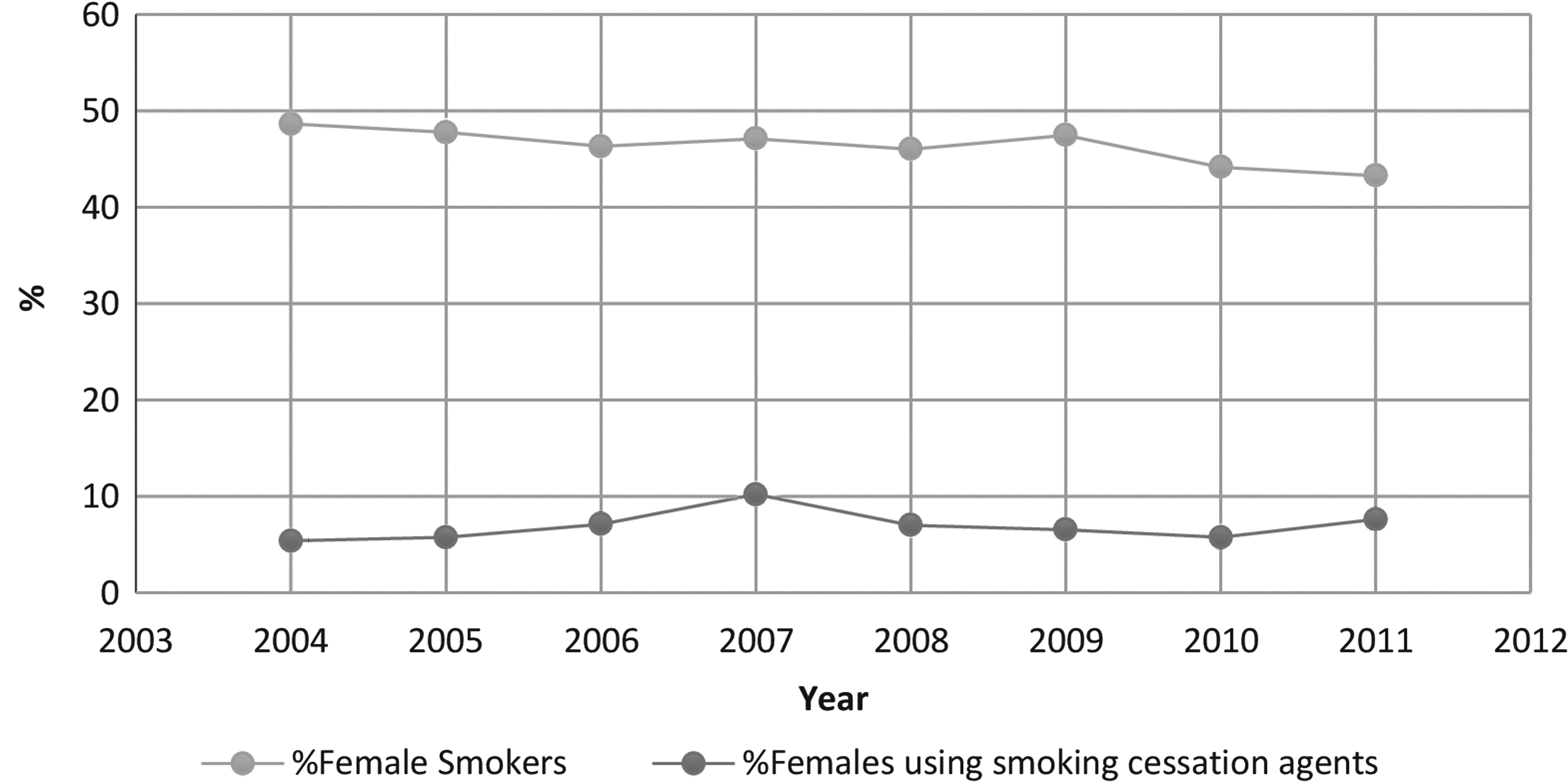
Trends in smoking and use of smoking cessation agents in females.
From Figure 1, it evident that the proportion of female smokers who use smoking cessation agents is significantly low. From 2004 to 2007, there was an increase in the use of smoking cessation agents among female smokers, which then showed a consistent decrease until 2010. Figure 2 shows the use of smoking cessation agents based on race. This graph shows inconsistent use of smoking cessation agents in both whites and non-whites. However, their use is higher among white female smokers than among non-whites.

Use of smoking cessation agents among whites and non-whites.
Discussion
Results from the current study show that the prevalence of CVD among females was consistently higher than that for males in all years. Females have been shown to have additional risk factors for acquiring CVD, such as menopause and use of birth control pills. 10 These factors, along with regular risk factors such as smoking and older age, might be responsible for the higher representation of females with CVD. Smoking is a major factor that has been shown to increase mortality among females. Our research found that an average of 12.37% females continued smoking, even after CVD diagnosis. This is a major public health concern that needs to be addressed, as CVD adds to healthcare costs and utilization. Overall, smoking among females has decreased from 32.7% to 12.2% during the period of 1980–2009 in the United States. 11 Although such a decrease was not found in our study, the data demonstrated that smoking prevalence remained in the 12%–13% range, even among females with CVD.
Many smoking cessation strategies are available to help this population to quit smoking. Smoking cessation through pharmacological treatment has been shown to be particularly effective. 12 Three types of pharmacological treatments, nicotine replacement therapy, bupropion and varenicline, alone or in combination, approved by the Food and Drug Administration (FDA), have been recommended to help patients quit smoking. 12 Interestingly, we found that a very small proportion of females with CVD used smoking cessation agents. Also, trend analysis in the use of smoking cessation agents in females with CVD who smoke showed an inconsistent rise and fall in the use of smoking cessation agents among this population from 2004 to 2011. A possible reason for this finding might be the preference for counseling over pharmacotherapy among patients who smoke. In contrast, this finding might suggest that treatment strategies for CVD may rarely include smoking cessation along with addressing CVD complications. This warrants special attention from healthcare professionals, as females with CVD who smoke are at higher risk of heart attacks and cardiac deaths. Research has shown that quitting smoking is more effective in decreasing the risk of mortality in females compared to males. 3 A mix of counseling and pharmacotherapy or other more intensive interventions have shown to be effective in smoking cessation and can be integrated into therapy for females who smoke and have CVD. 13,14 The American Society of Clinical Oncology (ASCO) along with FDA had put forth various smoking cessation efforts with the goal of improving patient's health. Various policy recommendations by ASCO such as increase in rates of insurance coverage, education for healthcare providers and patients, and incorporation of smoking cessation counseling as a part of key vital signs of care are also significant to end smoking cessation. 15,16 However, significantly more research might be needed to advance the goal of smoking cessation in a comprehensive and effective manner. In addition, it is not appropriate to expect immediate success with this strategy. The problem of nonadherence and relapse often hampers the progress of smoking cessation. Change of behavior is psychologically challenging for people addicted to smoking and it requires strong determination and effort to follow smoking cessation strategy. Patients who perform treatment tasks effectively have lower chances of relapse, which is normally not the case with serial smokers. 17 In addition, adherence to smoking cessation treatment is a challenge for these patients, especially if they are on multiple medications for CVD. Patients may fail to fill prescriptions or may discontinue therapy, which unknowingly increases the individual cost of therapy. These barriers are difficult to overcome through counseling and pharmacotherapy that puts onus on government as to how they tackle policies governing tobacco and the tobacco industry. Policies such as tax penalties may have an effective contribution to decreasing barriers of smoking cessation.
Additional analysis in terms of race and ethnicity showed that smoking behavior and the use of smoking cessation agents were higher in whites than in non-white females with CVD. This confirms the findings of a study conducted by Bush et al., in which almost 49% of smokers were female and the majority was whites. 18 According to ethnicity, the number of current smokers and the use of smoking cessation agents were higher in non-Hispanic females compared to Hispanic females. This finding gives some clues as to focusing recommendations for smoking cessation to help reduce morbidity and mortality related to CVD in women. Further research needs to be done to understand the reasons for low utilization of smoking cessation agents. There is a need for multi-professional and multi-sectorial involvement to improve tobacco control. Besides the use of smoking cessation agents, healthcare professionals such as physicians, nurses, pharmacists, and public health professionals also play important individual roles through their organizations. These healthcare professionals are in prime positions to influence policies, laws, and regulations that may favor smoking cessation. Health promotion and disease prevention programs are the focus of public health promoters and educators, and are also considered an important component, according to the American Association of Colleges of Pharmacy. 19 Adequate training of healthcare professionals at the college level in the area of suitable interventions for tobacco users or smokers will help improve cessation rates. Involvement of the governmental health sector may help increase awareness among health personnel and contribute to developing sustainable tobacco control programs at the national level. Regular screening of patients, providing at least minimal routine counseling, and regular follow-ups, along with the establishment of few regulations and policies regarding tobacco sales and use, are some strategies that may help in minimal to no use of tobacco among the population and especially among CVD patients. Promotion of evidence-based practices such as policies related to inclusion of tobacco use status and screening in pharmacies' dispensing systems, cost coverage by insurance companies in smoking prevention and cessation, and availability of nonprescription smoking cessation agents might help in smoking cessation efforts. 19 Like other studies, our study has strengths and limitations. Since MEPS is representative of the U.S. population, our study is generalizable, but due to the use of a secondary database, there might be some missing information that has a possibility of introducing bias. Social desirability bias and response bias are the possible limitations, as smoking status and smoking cessation use-related information in the database were self-reported by the patients. Self-reported surveys rely on patient recall, which may depend on perceived social acceptability of smoking behavior. In addition, it was not possible to collect information at the time of diagnosis of CVD in relation to smoking status and smoking cessation use. Collection of this information could have given some knowledge on the prevalence of smoking and use of smoking cessation agents in relation to time of diagnosis and disease duration.
Implications for practice and/or policy
The study shows that there were a considerable number of females with CVD who continued to smoke even after diagnosis and the use of smoking cessation agents was very low among them. It was observed that, over the years, neither did the number of female smokers with CVD decrease nor did the utilization of smoking cessation agents increase. Healthcare providers are at prime position to understand the reasons for low utilization of smoking cessation agents especially among females suffering from CVD and to subsequently address them. Provision of tailored smoking cessation counseling and regular monitoring of medication compliance for long term (e.g., at least 3–6 months) to females are some of the efforts that can be exercised. Health insurance programs may extend their coverage to smoking cessation pharmacotherapy to motivate healthcare providers in recommending smoking cessation agents. Also, tobacco cessation therapy could be made easily available in managed care and fee-for-service settings. We hope that dissemination of findings will encourage healthcare providers to ensure that all their patients who smoke are offered effective treatments.
Future research
A possible future research idea could be in the direction of exploring various reasons behind low utilization of smoking cessation agents among this patient population. Studies that evaluate the consequences related to quality of life, morbidity, and mortality because of this failure to utilize smoking cessation agents would be beneficial. It is also very important to explore some possible solutions to improve the utilization of smoking cessation agents. Another potential research could be done to assess the impact of policy changes, such as Electronic Health Records Incentive Program for smoking cessation efforts, in which clinicians and healthcare systems are incentivized and motivated to identify patients who smoke and to provide them with treatment.
Conclusion
The 8-year trend shows that the use of smoking cessation agents among females is very low, particularly among non-whites and Hispanics. Although the use of smoking cessation agents has been found effective in quitting smoking, the low utilization among women with CVD is alarming, warranting further investigation in this area. Collective efforts by health educators, pharmacists, clinicians, policy makers, and patients in preventing the use of tobacco and increasing the utilization of smoking cessation agents will help to decrease the risk presented by smoking in CVD.
Footnotes
Author Disclosure Statement
No competing financial interests exist.