
Abstract
Victims of domestic violence (DV) are not only subject to physical and emotional abuse but may also be at increased risk for less recognized dangers from infection with human immunodeficiency virus (HIV) and other sexually transmitted pathogens. Because of the close link between DV and sexual risk, women need to be educated about the consequences of acquiring a life-threatening sexually transmitted infection, risk reduction measures, and how to access appropriate HIV services for diagnosis and treatment. It is therefore critical for DV workers to receive sufficient training about the link between DV and HIV risk so that sexual safety planning can be incorporated into activities with their clients in the same way as physical safety plans. In this article, we discuss how the Many Hands Working Together project provides interactive training for workers in DV and DV-affiliated agencies to increase their knowledge about HIV and teach sexual safety planning skills to achieve HIV risk reduction.
Introduction
D
The Many Hands Working Together (MHWT) project provides training to DV agencies to achieve these objectives. The training intervention is based in theory on the AIDS Risk Reduction Model (ARRM) and employs interactive sessions to train workers in DV and DV-affiliated agencies. Since most clients seen in DV agencies are heterosexual women, our intervention focused on this group. However, similar kinds of abusive power dynamics occur in same-sex relationships.
The purpose of this article is to outline in more depth the theory behind the trainings, provide a brief curricular outline, and share initial lessons learned in the project.
Models of DV: Situational Violence Versus Intimate Terrorism
Developing a sexual safety plan requires acknowledging risk and planning ahead to mitigate sexual risk. Despite how much is known about DV, the widely held lay view is of a sudden, unpredictable violent outburst resulting from some type of victim-initiated trigger. 4 Within this model, safety planning is difficult because the episodes are unexpected, explosive, and uncontrolled.
Even among professionals who study it, there is a debate about the models used to describe DV. In one model, DV is situational, that is, resulting from a more gender neutral dynamic that exists within the context of a relationship in which both partners use violence symmetrically. This dynamic is theoretically remediable by counseling of the couple; however, situational violence is considered to be relatively rare. 5,6 In an alternative model termed intimate terrorism first described by Johnson in 1995, 7 the perpetrator (usually a man) exerts physical force (including physical and sexual violence) and emotional abuse as a means of control and subordination of a partner (usually a woman)—a situation unlikely to be alleviated through discussion. Physical injury is almost always associated with a pattern of escalating controlling behaviors, including limiting access to friends and family, insisting on knowing the woman's whereabouts, jealousy, and limiting information about family finances even when asked. A study by Lichtenstein 8 using focus groups and in-depth questionnaires with HIV-positive women in the southeastern United States elucidated the close link between sexual risk and DV. In this study, the women consistently described a pattern of highly sexualized abuse from disempowered men asserting power and control and projecting a sense of enforced ownership over women. A corroborating study from Finland by Flinck and Paavilainen 9 interviewed male perpetrators of DV who described it as their quest to find personal dignity, respect, and control by directly inviting communication through confrontation. Because the dynamic in intimate terrorism is rooted in a need to control and subdue, this places the health of the subdued partner at significant risk emotionally, sexually, and physically.
Intimate Terrorism and Risk for HIV
According to the CDC, 10 women in relationships with violence have four times the risk for contracting STIs, including HIV, compared with women in nonviolent relationships. Victims of intimate partner violence (IPV) more frequently report behaviors associated with an increased risk for HIV, including injection drug use, treatment for an STI, multiple sex partners, and intercourse without a condom. 11 A study of women in low-income urban settings found an inverse association between higher rates of IPV and condom use. 12 Low self-esteem, depression, and fear of abuse contribute to poor safer sex negotiation practices. Furthermore, coercive sex by a promiscuous partner who refuses condom use, uses injectable drugs, and limits access to early diagnosis and treatment places these women at high risk for HIV. 11,13
Authors of reviews of cross-sectional studies have noted an association between DV and HIV. 14,15 In fact, some have proposed that the inter-relationships between DV, substance abuse, and HIV risk constitute a syndemic. 15 However, few have documented DV as a specific risk factor for HIV in women, and the actual risk of acquiring HIV within the context of DV is unknown. Dunkle et al. 16 found a significant association between DV and increased risk of HIV infection (odds ratio 1.48, 95% confidence interval 1.15–1.89) in South African women after adjustment for women's own risk behavior. Lichtenstein's work describes the power dynamic whereby men actively subjugate women such that their vulnerability to an HIV-positive partner is increased. El-Bassel et al. 17 describe the progressive effect of DV on a woman's psyche resulting in her inability to resist unsafe sex. In addition, women with a history of childhood sexual abuse or abuse before their current situation have been conditioned to yield to power and control and will be unlikely to develop a sexual safety plan on their own. 13
Part of the subjugation of women is economic, and financial control is a key component of intimate terrorism. In resource-poor countries, it is universally acknowledged that violence against women and HIV acquisitions go hand in hand. A novel intervention in South Africa using microfinance reduced IPV by 55% 18 ; with longer term follow-up, it may show a reduction in HIV as well. In the United States, many women are no less bound to their partners economically—they are often dependent on their partners for housing, food, and health insurance.
Knowing about HIV risk and risk reduction is not sufficient for women to be able to practice risk reduction. 19 Consistent condom use is the most effective way of preventing HIV in sexually active adults, but is not a viable solution for the majority of women DV survivors. In general, negative attitudes by both men and women are a barrier to their use. Men employing intimate terrorism will likely feel less control and be more likely to inflict physical injury if asked to use a condom. For women, the potential safety gain in STI risk reduction with condom use is offset by the potential safety loss in the violence in the relationship. Therefore, condom use, the principal pillar of most HIV prevention programs, is not available for most women in a violent relationship.
The ARRM (described in detail below) was designed to change high-risk sexual behaviors associated with HIV transmission by examining contributing social and psychological factors (e.g., perception of risk and self-efficacy beliefs) and implementing solutions directed at reducing high-risk activities (e.g., communication skills, help seeking behavior). 20 Based on this model, we developed an intervention (the MHWT project) incorporating HIV education and sexual safety planning for agencies that work with victims of IPV.
The Need for Sexual Safety Assessment and Planning
In the safety assessment phase, a woman must make behavioral changes based on her assessment of risk and lethality. Cognitive behavioral change models, the theoretical models that underpin much of HIV prevention, assume that participants have free agency to make change once knowledge is gained. Within DV, women have options, but may become paralyzed by how limited the options are—harm reduction rather than harm elimination. Planning around physical safety is a hallmark of practice by DV agencies and acknowledges harm reduction as the initial step in the process.
It is incumbent upon staff in agencies serving survivors of DV to implement concrete sexual safety plans in the same way that they develop safety plans around physical safety. The Family Planning Council in southeastern Pennsylvania instituted an outreach and education program around DV and HIV in 2003. Their needs assessment discovered that DV workers were reluctant to bring up sexual health issues, had poor baseline knowledge about HIV and HIV prevention, and had no tools for developing a sexual safety plan. Their intervention involved working to overcome partner resistance to condom use, but was unsuccessful in creating change. 21 Although the New York State Department of Health provides excellent resources that integrate screening for DV during HIV testing as well as resources for general practice social workers around HIV risk reduction, it does not specifically link DV and HIV for training for DV workers. 22
Women need to be made aware that their HIV risk is increased, HIV is lethal, it is preventable, and given tools for harm reduction. This is accomplished first at an agency level by improving staff knowledge about HIV risk and risk reduction, teaching skills around the risk interview and risk reduction counseling, and helping staff find opportunities for incorporating sexual safety planning into daily activities with clients.
Theoretical Models for the Intervention
The ARRM summarized in Figure 1 20 is a three-stage process involving (1) Labeling—recognition of risk for HIV, (2) Commitment—developing a conscious commitment to change behavior, and (3) Enactment—acting on the commitment to change through adoption of risk reduction practices.

AIDS Risk Reduction Model. (Adapted from Catania J, et al. Towards and understanding of risk behavior. 1990.)
ARRM was tested with high-risk heterosexual couples 23 and found to be efficacious in improving condom use and sexual communication. It is most effective in areas where the risk of HIV infection is perceived as greatest; simple knowledge of the threat is not enough. In a meta-analysis of factors important in condom use in a general population, 24 viewed through an ARRM lens, behavior-specific cognitions, social interaction, and preparatory behaviors were more important than increasing knowledge and beliefs about the threat of infection, that is, development of a specific commitment and enactment plan was more important than the labeling alone. In a study by Longshore et al., 25 examining gender differences with use of ARRM, women's confidence that they could practice risk reduction was more significant than improved knowledge alone.
ARRM teaches techniques based on motivational interviewing, a patient-centered counseling style that uses a form of collaborative conversation to strengthen an individual's own motivation and commitment to change by addressing ambivalence about change and exploring the person's own reasons for change within an atmosphere of acceptance and compassion 26 to develop a sexual safety plan. The client and counselor form a partnership, in which the client's autonomy and freedom of choice drive the interaction. The motivation to change is elicited from the client by her desire for safety. It is the client's responsibility to work through the conflict between continuing in the current abusive relationship and making changes that would bring with it new challenges. The DV counselor acts as a consultant to provide information on a menu of safety options, but does not proscribe particular risk reduction choices. Motivational interviewing is effective because the client's readiness for change may fluctuate based on time, distance from the most recent threat, and by what the specific threat is. The vague threat of HIV infection may seem less real than the bruise around her eye. Motivational interviewing addresses these issues.
The MHWT program
The MHWT project is an interactive training intervention based in theory on the ARRM for workers in DV and affiliated agencies developed in response to a request for proposal from the federal Office on Women's Health, Department of Health and Human Services. The core of the program was developed over the course of a year based on information gathered through focus groups with DV staff and women who were either in an abusive relationship or who had left one. This information helped to identify issues the curriculum would need to address and confirmed the strong desire expressed by the women about receiving information about HIV/other STI. The project was initiated in 2007 at two DV agencies in the Philadelphia area. Feedback was obtained after each training. Check-in sessions were also conducted with the staff on a regular basis to discuss progress in implementation of HIV risk reduction with their clients.
The goal of the MHWT project is to train DV workers to help clients take measures to reduce their HIV risk through improving their awareness of their HIV risk, taking concrete steps to reduce their HIV risk when possible, and seeking early diagnosis and treatment when HIV prevention has failed. The design of the training is to build on an intervention where DV counselors already have proficiency—the safety plan—by adding a sexual safety plan. They are educated about the link between HIV and DV through relevant case studies, about HIV prevention measures and the importance of early diagnosis and treatment, and how to access HIV testing and care services. Through interactive sessions, counselors role-play sexual safety planning and are provided assistance in how to integrate sexual safety planning into existing practice.
Overview
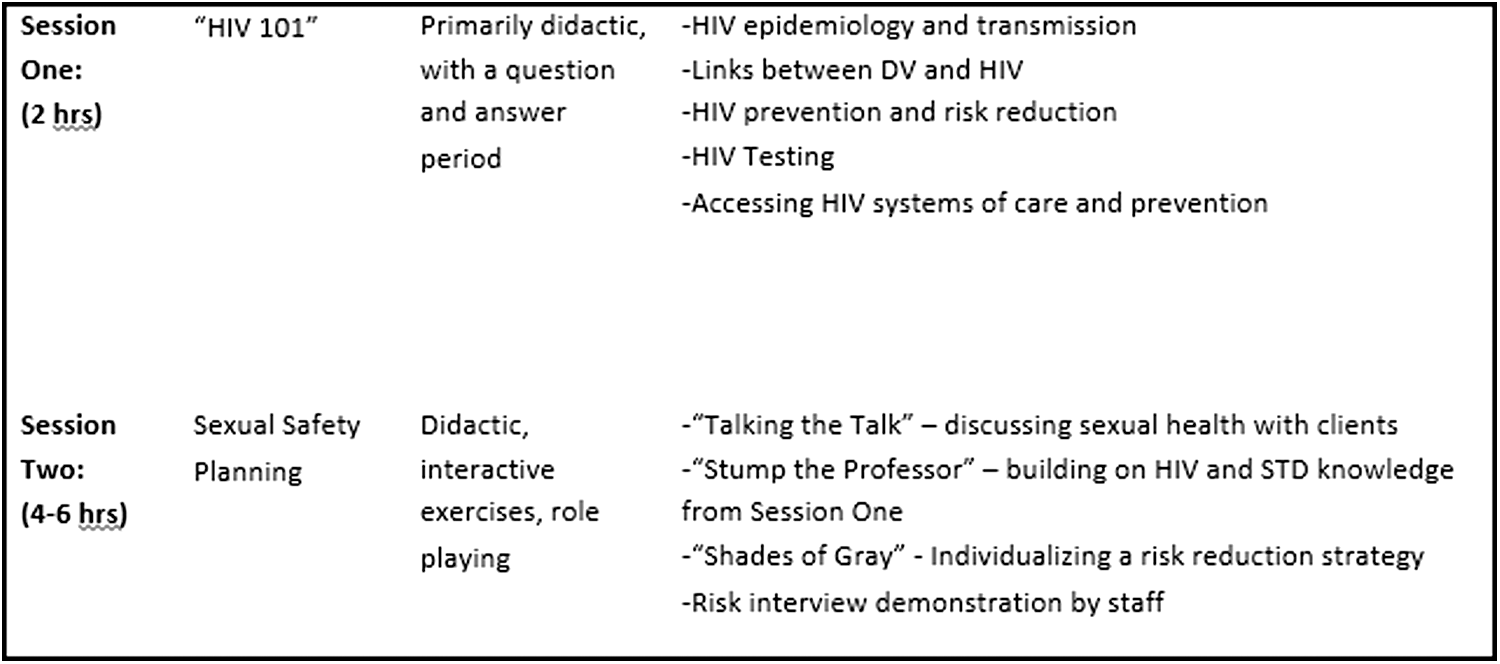
The MHWT curriculum consists of two interactive educational programs for DV workers to increase their knowledge about HIV and to teach sexual safety planning skills. The curriculum is followed by monthly check-ins with DV staff to reinforce the material presented in the trainings, help troubleshoot the process of integration of safety planning into daily practice, and to provide periodic updates to address knowledge gaps and offer new information as needed. The program is provided by program staff to staff at DV agencies and other sites such as homeless shelters where there is a high concentration of women DV survivors. A train the trainer module has also been developed so that HIV providers in areas beyond Philadelphia can be trained to provide the MHWT curriculum locally (Fig. 2).
Many Hands Working Together curriculum.
Session 1
This module is intended to prepare DV workers to perform sexual safety planning by modeling discussion of sexual health matters in a comfortable yet authoritative way and providing workers with the baseline knowledge needed to develop a sexual safety plan. The didactic session assumes that baseline knowledge about HIV is poor and is given by a medical provider to all agency staff. The goal is to improve awareness for anyone who might interact with clients around HIV issues, to inform the learners about the links between HIV and DV, and to debunk common myths around HIV. The lecture is divided into sections on basic epidemiology and HIV transmission, DV/HIV links, principles of HIV prevention for DV survivors, and what happens after a positive HIV test.
Session 2
This workshop-type format is provided only for direct line staff interacting with clients clinically (i.e., case managers, hotline workers, and court advocates) within 1 month of session 1. The intent is that workers will seek opportunities within their individual roles to provide information on sexual safety planning. This may be a case manager working with a client to develop a comprehensive safety plan around physical and sexual safety over multiple sessions and/or a hotline worker advising a caller at risk to get an HIV test.
The session explains how to perform a risk interview that both seeks information from a client about her specific risks and provides brief, concrete harm reduction information. The risk interview is client centered, but semidirective, focuses on providing small bits of pertinent information, and is goal oriented. Figure 3 is a sample encounter demonstrating a risk interview.

Sample risk interview encounter.
Before a risk interview can be performed, the counselor must be comfortable talking about sexual matters, have sufficient HIV prevention knowledge to be able to provide risk reduction strategies, and be willing to partner with the client to determine the best plan for her. In the first exercise, Talking the Talk, workers take turns role-playing interviewing a client about her sexual risk. The purpose of this is to enhance worker comfort with sexual content and to provide feedback about their use of language. Workers are encouraged to speak frankly about sexual health. Facilitators guide them away from using indirect terms and euphemisms for reproductive anatomy and sexual matters. Vernacular and slang terms used by clients are explored and situations discussed where it is appropriate to use the client's terms rather than the correct clinical terms.
The second exercise, Stump the Professor, asks, “What questions might your clients ask that you might not know the answer to?” (e.g., “How can a woman using a female condom still urinate?”). Workers are given a prize if they can come up with a question about sexual health, HIV, and STIs that project staff are unable to answer. This further increases their comfort level in discussing sexual health, gives them an opportunity to ask questions left unanswered in session 1, and explores areas of knowledge gaps.
The third exercise, Shades of Gray, provides opportunities to strategize around best- and worst-case scenarios in safety planning—and then all the options in between. For example, Jane has an abusive partner who is newly diagnosed as HIV positive. He continues to force her to have unprotected sexual intercourse. The best case is that she is able to eliminate her risk by leaving him. The worst case is that she continues to have unprotected sex and does nothing else. Options in between include encouraging him to take medicine to lower his risk of transmitting HIV to her, introducing condoms as sexual play in their relationship, decreasing the frequency of intercourse by feigning a yeast infection, headache, etc., and getting an HIV test regularly. Although there is a risk that behavior change could lead to escalating abuse, the goal is to provide more information for workers about choices and allow them to see that there may be intermediate options that can potentially provide some harm reduction, so they can partner with and empower Jane to choose among a menu of potential solutions.
The final exercise is a demonstration by staff of how to provide sexual safety planning through a risk interview (in a longer form than what is presented above as a sample). In this exercise, comfort with discussion of sexual health is modeled, partnering with a client is demonstrated, and more risk reduction content is delivered. At the end, workers are asked to imagine performing a risk interview and provide an assessment on their readiness to perform one. Workers are asked to try to integrate risk interviewing into their practice for the next month and a date for the first check-in is given.
Participants complete both a pre- and post-test for HIV knowledge, as well as a session evaluation and questionnaire, assessing perceptions of their knowledge and comfort with discussions about HIV. At the first and subsequent monthly check-ins, workers are asked to give examples of how they have integrated sexual safety planning into their practice. Feedback is given by project staff to enhance effectiveness, correct information, and provide mini-lectures on topics where there is consistently a need for more knowledge and/or clarification.
Initial Lessons Learned
Implementation of the MHWT training program at two DV agencies in the Philadelphia area resulted in greater awareness, knowledge, and understanding of HIV among the 31 counselor participants, as well as greater comfort and confidence in discussing HIV and HIV risk reduction with clients, referring them for HIV testing, and helping them address HIV risks. At the end of the first year of the program, approximately two-thirds of the DV providers developed sexual safety plans as part of a physical safety plan, referred clients for testing, and distributed materials on HIV.
As our experience illustrates, the use of the sexual safety plan as an intervention for DV workers to help reduce risk of HIV can be effectively implemented, although its ultimate effectiveness is unknown and warrants further research. Safety planning is familiar to DV workers, so addition of sexual health content is a logical next step. That being said, there are cultural, attitudinal, and logistical barriers to instituting HIV prevention in DV agencies that must be overcome.
To measure the effectiveness of the MHWT program in terms of impact on clients and reduction in HIV transmission would require a larger number of participants (both workers and clients) and study over a prolonged period of time. Unfortunately, feasibility of doing this in DV agencies is questionable. Most agencies are working with limited resources (time and financial) and these are allocated to providing quality services to a high-need population. Taking time and focus from their primary service mission to run a study, even with additional funding, would create cultural and practical issues for the staff and potential trust issues with clients. A more detailed study design would also likely involve a more intensive consent process with a vulnerable population in a setting where confidentiality is of high concern. Thus, one of the strengths of our study was that it focused on working with staff rather than clients, therefore ameliorating these concerns.
The field of DV ties together a diverse group of agencies with the primary aim of providing physical safety for women resulting from violence where immediate impact can be seen. While national medical expert panels write practice guidelines for HIV, 27 it is more difficult for DV. Agencies tend to be either a social service agency or an extension of a legal services agency, so it is difficult to develop a unifying set of principles that would guide all workers. Many agencies avoid use of written notes lest they be subpoenaed, yet the lack of documentation makes it difficult to evaluate the impact of an intervention or secure research funding. Agencies are perpetually underfunded and understaffed and many rely heavily on workers who are themselves survivors of DV so that the addition of HIV prevention may not seem possible. Workers are more likely to view the danger of a client being hit by an abusing partner as more dangerous than a woman acquiring HIV from her partner—yet also feel that while HIV can be life-threatening, there is nothing a woman can do to avoid it. All of these challenges lead to difficulty in developing and implementing evidence-based measures that can be widely disseminated.
Careful project planning is important in overcoming these challenges. Each agency brings with it a specific culture, practice model, and demographic that requires fine-tuning of the curriculum. Meeting with program leadership first to learn about their motivation to participate and how they see this fitting in with what they already do is important. Agencies with a strong history of valuing training and innovation will be the most successful. Agencies with a paid professional staff that consistently provides service over time will benefit the most from this training rather than agencies with staff that consists primarily of volunteers who may be transient. Whatever the perceived comfort level with HIV knowledge a staff has, it is important that a solid foundation of HIV knowledge is laid down; sexual safety planning without HIV risk reduction content is inadequate. Beyond knowledge, skill in discussing sexual health is essential. Although DV workers are trained in social services, they may lack the knowledge and skills to address other aspects of women's lives, including sexual health. DV workers may perceive that since they talk to women about their intimate relationships, those skills translate to efficacy in sexual health. In our experience, rarely have we found this to be the case.
Connecting DV agencies to an HIV infrastructure much the same way they are already tied into the legal system is an important component of the program. It would be unthinkable for a DV worker to not know how to help a client obtain an order for protection, but we discovered that few workers at baseline know how to obtain an HIV test. As workers gain comfort in sexual safety planning, they will need to have linkages with HIV testing agencies, providers, and other services and resources for their clients. Finally, involvement of HIV providers is crucial, not only during the train the trainer component of the project but also in becoming proficient in appropriate DV screening referral. Development of strong professional relationships that outlast the MHWT project will help to ensure reinforcement of the curricular content and sustainability of the project goals.
Footnotes
Author Disclosure Statement
No competing financial interests exist.