
Abstract
Background:
Venous thromboembolism (VTE) is rare among young women and is often presumed to occur in the setting of a genetic predisposition or during the use of estrogen-containing combined hormonal contraceptive or to have an unknown cause. This study aims to describe the distribution of VTE risk factors among women with a confirmed VTE.
Methods:
We identified all women aged 15–46 years with a VTE diagnosis at Columbia University Medical Center from 2005 to 2012 using medical center databases. We then reviewed all electronic medical records to validate the diagnoses and identify risk factors associated with each confirmed case.
Results:
We identified 315 cases and confirmed 186 (59%). The proportion of unconfirmed cases increased over time. Forty percent of confirmed cases were associated with hormonal contraceptives or pregnancy. Ninety-five percent of confirmed cases had identifiable major risk factors including a personal history, family history, malignancy or other predisposing illness, recent long-haul travel, trauma, hospitalization, and obesity; many had multiple simultaneous risk factors. None of the confirmed cases was associated with a previously known genetic predisposition, but in 10 confirmed cases a genetic predisposition was identified during evaluation. In only 10 of the 186 confirmed cases could we not identify any acquired risk factor, and only 2 of those 10 women had a genetic predisposition.
Conclusions:
Many reproductive age women experiencing a VTE have risk factors unique to this group, and most have multiple risk factors, confirming that this is a multifactorial disease. The large proportion of unconfirmed cases suggests the need for great caution in using administrative databases for research due to poor diagnostic specificity and due to lack of information about additional risk factors.
Introduction
V
Well-recognized major risk factors for VTE in reproductive age women include estrogen-containing hormonal contraceptives (CHC) and pregnancy. CHC use confers a two- to four-fold increase in risk for VTE compared to nonusers 1,3 with the greatest increase within the first 3 months of use. 4 Pregnancy confers a five-fold increase in risk for VTE, 5 –7 with the highest risk during the puerperium. Malignancy is a major VTE risk factor at any age, and among reproductive age women confers up to a nine-fold increase in risk of VTE compared with women without cancer. 8 –10 Additional risk factors for VTE include personal or family history of VTE, trauma, long-haul travel, certain chronic illnesses, hospitalization with or without surgery and postoperative immobility, heritable thrombophilias and antiphospholipid antibody syndrome, ovarian stimulation, as well as increasing age and obesity. 1,11 Appendix Table A1 lists chronic illnesses (limited to those encountered in this case series) that confer at least a moderate increase in VTE risk.
The goal of this analysis was to characterize the distribution of VTE risk factors among reproductive age women with this diagnosis in a single academic medical center. In addition, because many investigators rely on large administrative databases for pharmacoepidemiology studies, we sought to assess the validity of our medical center database for correctly identifying women with VTE diagnoses. 12
Methods
After receiving Columbia University Medical Center (CUMC) Institutional Review Board approval, we obtained from the institution's Clinical Data Warehouse a list of all women age 15 to 46 years old with a diagnosis of VTE between 2005 and 2012, years during which data were most likely to be complete. 13 The Clinical Data Warehouse collects data from the electronic health records in two CUMC applications, a web-based clinical information system (WebCIS) and Eclipsys SunriseXA. WebCIS was implemented in the hospital in 1998 and Eclipsys SunriseXA was implemented in 2003. 13,14 Diagnoses in the Clinical Data Warehouse are represented using International Classification of Diseases, 9th revision (ICD-9) codes and the database covers emergency department and outpatient clinic encounters as well as hospitalizations; the WebCIS portion of the system includes radiology, laboratory, pathology, and operative reports. Eclipsys also includes clinical notes from all encounters. Prior to 2013 the warehouse did not cover faculty office visits, thus excluding from this analysis those women whose only encounter or evaluation here consisted of a faculty practice visit. We included cases only from 2005 forward due to concern that electronic notes during the earlier years may have been incomplete. Appendix Table A2 lists the ICD-9 diagnosis codes used to identify VTE events for this analysis.
With the list of results, we used an ad hoc data collection template to abstract relevant variables from each woman's electronic chart including demographic information and site of care, medical history, and other event-related information. We collected the results of radiological imaging and laboratory tests directly from radiology and laboratory reporting systems, respectively. If diagnostic imaging took place at an outside facility, we included the case if the images and/or formal report were included in the CUMC chart (as was nearly universal). One physician (VP) initially abstracted all charts. Using these data, we evaluated the VTE event, and confirmed a diagnosis of VTE by review of the history and clinical assessment supported by radiological imaging including Doppler ultrasound, duplex scanning, or contrast venography for DVT and chest computed tomography scan or magnetic resonance imaging compatible with diagnosis for PE. A VTE diagnosis was ruled out if imaging was negative or in the absence of an appropriate imaging study. In all cases of ambiguity of the diagnosis, a hematologist (AE) re-abstracted the record. Our criteria for VTE diagnosis were equivalent to the World Health Organization's algorithm for diagnosing definite VTE. 15
For all confirmed cases a second investigator (CW) re-abstracted the records to identify and confirm VTE risk factors. We included a pregnancy within two months of the event as a risk factor, 7,8 and other transient risk factors (including CHC use) only if present within 1 month preceding the diagnosis. Our goal was comprehensive identification of risk factors; we did not assess the reliability of record abstraction among the investigators. Because most women with confirmed VTE had easily recognizable risk factors, clinical guidelines did not indicate extensive additional laboratory testing; thus, we cannot report on genetic thrombophilias or antiphospholipid syndrome for most of the confirmed cases in this series. 16 –18
Statistical analysis
We calculated the true positive rate of confirmed VTE among women who were in the NewYork-Presbyterian Hospital (NYP) Clinical Data Warehouse (following Severinsen, 2010). 19 We calculated descriptive statistics for demographic and clinical factors related to VTE for all women in the database, and analyzed the distribution of risk factors, focusing on those with known associations to VTE risk. Statistical analyses were performed using SAS 9.3 (SAS Institute Inc.). This study included all VTE events at a single institution, and no sample size calculations were performed as this was a descriptive rather than a hypothesis-testing study.
Results
Three hundred fifteen unduplicated reproductive age women with ICD-9 diagnoses for VTE were identified in the electronic health records of CUMC's Clinical Data Warehouse over the 8-year study period. Figure 1 shows the flow of the chart review. Of the 315 women the Clinical Data Warehouse identified, we retrieved 100% of the associated medical records and confirmed 186 (59%), but could not confirm 129 (41%) of the VTE diagnoses. We excluded only two of the VTE events due to lack of radiological imaging. We excluded 101 due to negative imaging and 26 because the encounter was miscoded and no VTE event had been suspected. Most of those 26 women had experienced a VTE in the more distant past that was completely unrelated to the index encounter. Among the 101 women with negative imaging, a diagnostic code had been assigned during an initial encounter, and prior to the results of the imaging. As the ICD-9 coding system does not have a way to specify a tentative diagnosis, the initial diagnosis survived in the records even after lack of confirmation. The annual number of confirmed cases ranged from 15 to 31 with no evidence of a secular trend. In contrast, the annual number of unconfirmed events ranged from 6 to 25 and increased over time such that the proportion of confimed cases was 69% in the earlier 4 years and dropped to 54% in the more recent 4 years (Chi-squared = 6.78, p = 0.01). One hundred twenty-five of the confirmed VTEs were DVTs alone. Fifty-one events were PEs and 41 of the PEs occurred in combination with a DVT; 10 events were CVTs. Seventy-six percent of the VTEs were first events (n = 141/186). During the years reported here CUMC admitted 101,158 women aged 15–44 years, constituting about 20% of total admissions. The prevalence of confirmed VTE among reproductive age women was thus approximately 1.84 per 1000 admissions.
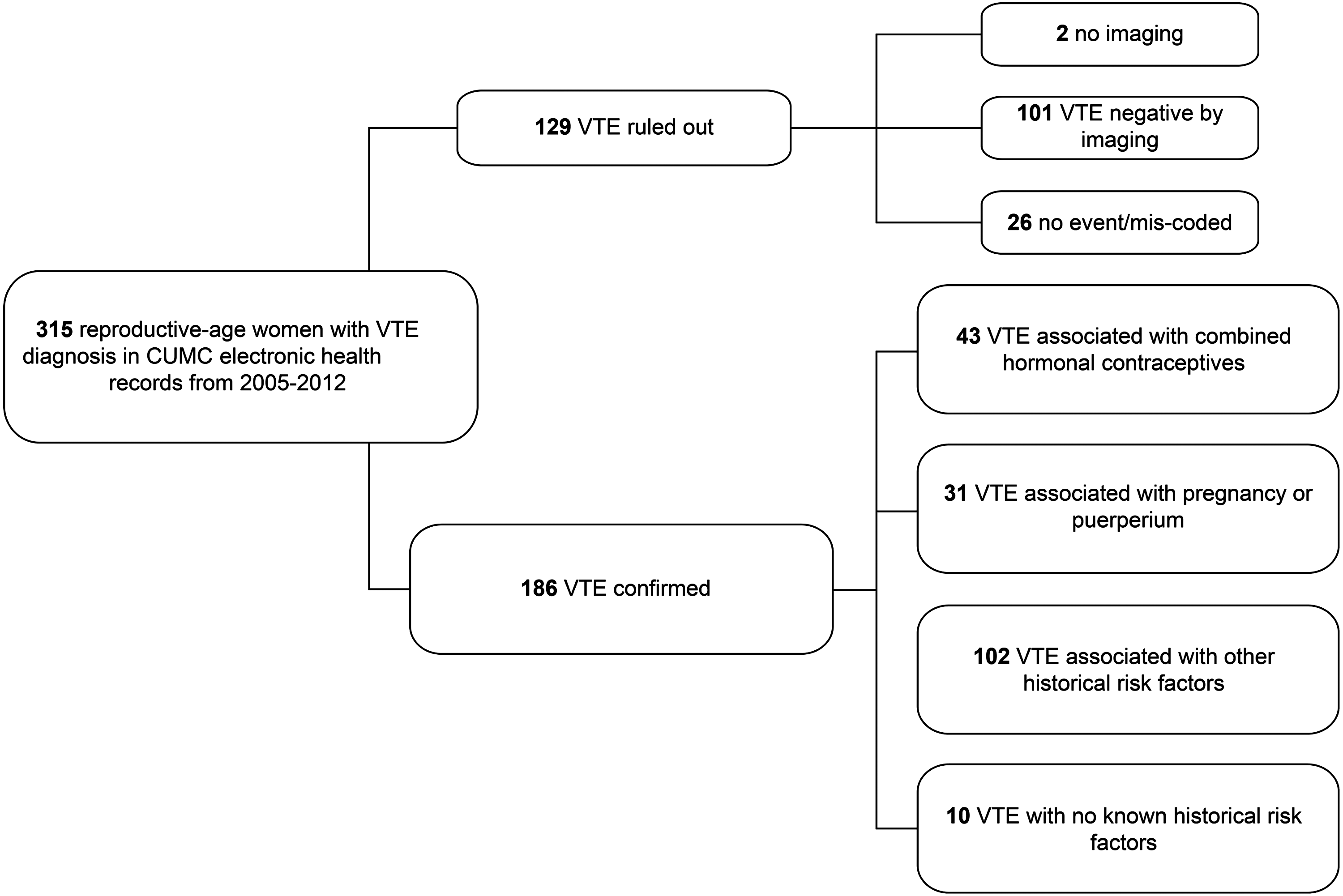
Flow diagram of chart review process. VTE, venous thrombo-embolism; CUMC, Columbia University Medical Center.
Table 1 displays baseline characteristics of women included in this study stratified by VTE confirmation or exclusion of the event. Most women with confirmed VTE were either already hospitalized or admitted during this episode (n = 163/186, 88%), while unconfirmed cases were more likely to be outpatients. We assessed the independence of type of VTE (DVT alone versus PE with or without DVT) among the major risk factors (CHC use, pregnancy, or other; 32%, 13% and 29% of VTE's were PE's, respectively) (Chi-squared = 5.10, p = 0.08). There were too few CVT cases to evaluate the difference in major risk factors for this subgroup.
Age is provided as the mean (range); all other characteristics are provided as n (%).
Women were classified as inpatients if they received both inpatient and outpatient care associated with the index event.
CVT, cerebral venous thrombosis; DVT, deep vein thrombosis; PE, pulmonary embolism; VTE, venous thrombo-embolism.
The major reproductive risk factors among these women were CHC use and pregnancy (Table 2). Of the 186 confirmed VTE diagnoses, 43 were associated with CHC use within the last month, 31 were associated with pregnancy within the last 2 months, and 112 were associated with other known risk factors including personal or family history of VTE, chronic illness including malignancy, long-haul travel, trauma and hospitalization, as well as obesity. We included in Table 2 only those chronic illnesses reported among these cases that give a substantial increase in VTE risk (as listed in Appendix Table A1). An additional 55 women had other chronic illnesses, but those illnesses are associated with VTE weakly or not at all (e.g., hypertension). Of the 186 women with confirmed VTE, 132 records included a calculated body mass index (BMI) (median = 27.5) and 50 of these 186 women had a BMI > 30 kg/m2 (median BMI of this group was 35.9). An additional 7 women had a clinical note indicating obesity/morbid obesity without a calculated BMI in the record. In only 6 women (3%) was obesity the sole VTE risk factor (median BMI 33.8). We identified one VTE associated with ovarian stimulation in a woman with breast cancer; the absence of other such events during this time interval was confirmed by the CUMC Division of Reproductive Endocrinology (personal communication). Table 2 shows the distribution of additional risk factors stratified by CHC use, pregnancy, or other (i.e., women with other known risk factors or none). Many of these risk factors are not mutually exclusive. Only 10 of the 186 women (5%) with confirmed VTE had no known acquired risk factors.
Age is provided as the mean (range); all other characteristics are provided as n (%).
Risk factors are not mutually exclusive and the sum of each column is thus > 100%.
Chronic illnesses associated with increased risk of VTE, excluding malignancy, which is categorized separately. An additional 55 women had other chronic illnesses that are not associated with increase in VTE risk.
Long-haul travel defined as 4 hours or more.
BMI, body mass index; CHC, combined hormonal contraceptive.
Table 3 shows the number of risk factors identified for each case. Overall, we identified 345 risk factors among the 186 confirmed cases, or 1.9 risk factors per event. Ten women with a confirmed VTE had no risk factors identified by medical history; 6 additional women had obesity as the only risk factor. Of the risk factors we consider here, obesity has the most limited effect on VTE risk. Eliminating obesity leaves about 1.6 risk factors per confirmed event. For 9 of the 43 women (21%) with a CHC-associated VTE, CHC use was the only identified risk factor, while 34 women (79%) had additional historical risk factors, as shown in Tables 2 and 3. One of the CHC users received a diagnosis of a gastrointestinal adenocarcinoma shortly after her VTE diagnosis, which probably contributed to her VTE risk, but was unknown prior to that event. The other cancer case in a CHC user noted in Table 2 was an astrocytoma diagnosed 15 years prior to the VTE with treatment completed 10 years prior to the VTE. Sixty-one percent of the women with a pregnancy-associated VTE also had additional risk factors.
All values are provided as n (%).
Other known risk factors include family history, personal history, hospitalization, chronic illness (limited to chronic illnesses associated with increased risk of VTE), malignancy, trauma, long-haul travel, and obesity.
The index VTE occurred during or shortly after a hospitalization in 51 women, making hospitalization itself the most common risk factor in this series. In many cases this hospitalization was associated with trauma, a complication of pregnancy or a chronic illness. In 23 of those hospitalizations the women underwent a specific procedure known to carry a VTE risk, such as orthopedic surgery to a lower extremity or cardiac catherization. We did not include a hospitalization for delivery alone as an additional predisposing event because essentially all pregnant women ultimately have a hospitalization for delivery; 9 of the 31 pregnant women with a VTE had the diagnosis made in the postpartum time period.
Among the 186 women with a confirmed VTE, one-third underwent genetic testing for factor 5 Leiden mutation and/or for the prothrombin gene G20210A mutation, including 4/10 without additional risk factors and 3/6 women in whom obesity was the only risk factor. Ten of those tested had a positive result and 2 of these (1 with each abnormality) had no other risk known factors. No women with obesity as the sole risk had a positive result for these genetic predispositions. Many cases also underwent testing for proteins C and S and antithrombin; however, because these were functional tests and often measured during an event, we were unable to interpret these levels.
Discussion
This 8-year case series from a single medical center validated all VTE diagnoses based on review of individual records, and did not rely solely on ICD-9 codes identified in the hospital database. We were able to confirm only 59% of the VTE cases in the database, which is somewhat lower than the 70% confirmation rate reported by Severinsen in an assessment of VTE diagnoses in the Danish National Patient Registry. 19 This result implies that investigators should be cautious in using unconfirmed diagnoses of VTE from clinical or administrative databases to identify cases for epidemiological studies or for other research. Over 8 years, an average of 40% of our cases were unconfirmed following medical chart review, and we observed an unexpected and substantial increase in the proportion unconfirmed in more recent years. This change over time may result from an increase in diagnostic suspicion, or a change in documentation and coding. Secular changes in the accuracy of diagnoses recorded in databases may limit the value of this information for research and this result further supports the need for diagnostic confirmation when identifying cases from administrative databases.
This case series enumerates the common, readily identifiable factors contributing to VTEs among reproductive age women. Because patients may fail to report or clinicians may sometimes fail to ask about or record a risk factor and because we may have missed some risk factors during chart abstraction, the risk factors tabulated here are to some degree an underestimate of all risk factors for VTE among these cases. Among the most common individual risk factors were use of combined hormonal contraception (23%) and pregnancy (17%); thus 40% of the cases were partly attributable to mutually exclusive risk factors unique to reproductive age women. Notably, none of the 43 women with a CHC-associated VTE had a personal history of VTE, indicating excellent adherence to practice guidelines in the prescription of hormonal contraceptives. 20 Nonetheless, 79% of the women with a CHC-associated VTE had additional risk factors, and the prevalence of recent hospitalization, trauma, and long-haul travel among them may indicate missed opportunities to reduce VTE risk by stopping CHC use at the onset of a new predisposing condition. The relevant CDC practice guidelines do not address how long to discontinue estrogen-containing HC in the setting of transient risk factors, and this would be an excellent problem for future research.
In agreement with contemporary guidelines that among individuals with transient risk factors for VTE the search for a genetic predisposition is not recommended, only one-third of the confirmed cases in this series underwent genetic testing for VTE predisposition. 16 –18 In a series of 87 women with VTE or stroke while using exogenous hormones, all women underwent testing for genetic predispositions and 37% were positive, but, as was seen here, the majority had additional major risk factors. 21
Chronic illness and malignancy were present in one-quarter of these women. Because this study has no general population comparison group, we cannot estimate the importance of these risk factors; however, serious chronic illness and malignancy are unlikely to be this prevalent among women with a mean age of 34 years. In nearly one-quarter of the cases described here, the patient had a personal history of VTE, a reminder that the risk of recurrence is substantial. The prevalence of multiple risk factors in this series may indicate referral bias. Perhaps women who experience VTE in the presence of comorbidities are more likely to already receive care or be referred for care in an academic medical center, while healthier women experiencing a VTE might receive care as outpatients or in a community hospital. Are multiple risk factors more common among the women in this series than would be found in a population-based sample? Population-based series of VTE including men and women of all ages in both Rochester County, Minnesota and in Worcester, Massachusetts also identified that the vast majority of individuals with a VTE diagnosis had major risk factors. 8,22,23 Thus, the prevalence of easily recognizable risk factors in this case series has proven to be similar to that reported in other studies (which included mainly older people due to the increased incidence of VTE with age), and thus even among reproductive aged women idiopathic VTE is rare. This case series may be somewhat unrepresentative of the full spectrum of VTE among reproductive age women; however, those studies restricted to “idiopathic” VTE cases would be even more unrepresentative of the spectrum of the condition in the reproductive age population as we found that “idiopathic” cases are rare.
VTE increases with age, and reproductive aged women comprise a minority or those affected. It may be surprising that 95% of the women described here had well known acquired risk factors for VTE, and that most of them had multiple risk factors. VTE is recognized as a multifactorial condition, and even the 40% of women in this series with hormonal contraceptive use or pregnancy as a risk factor had numerous additional risk factors. Attention to these relationships should help clinicians to identify reproductive aged women predisposed to a VTE and may thus help reduce risk. The most salient example would be to avoid the use of estrogen-containing contraceptives in women with multiple chronic or transient VTE risk factors.
Finally, that we could confirm only half of the cases identified in an administrative database may be surprising. The proportion of cases confirmed over time decreased, perhaps due to greater diagnostic suspicion or simple changes in the approach to coding. That result suggests the need for great caution in the use of diagnostic codes from administrative databases to identify VTE cases for epidemiological studies, except where it will be possible to carry out a search for diagnostic confirmation.
Footnotes
Acknowledgments
This study was funded by the Howard Solomon Research Fund of the Department of Obstetrics and Gynecology at Columbia University Medical Center and the Irving Institute for Clinical and Translational Research Collaborative and Multidisciplinary Pilot Research Award from CUMC.
Author Disclosure Statement
CLW consults for Merck and Bayer, both of which manufacture hormonal contraceptives. The other authors do not report any competing financial interests.
| Billing code | Diagnosis |
|---|---|
| 415.1 | Pulmonary embolism and infarction |
| 437.6 | Nonpyogenic thrombosis of intracranial venous sinus |
| 453.40, 453.41, 453.42 | Acute venous embolism and thrombosis of deep vessels of lower extremity (irrespective of location) |
| 453.50, 453.51, 453.52 | Chronic venous embolism and thrombosis of deep vessels of lower extremity (irrespective of location) |
| 671.40, 671.42, 671.44 | Deep phlebothrombosis postpartum (irrespective of timing) |
| 671.50, 671.51, 671.52, 671.53, 671.54 | Other phlebitis and thrombosis complicating pregnancy and the puerperium (irrespective of timing) |
| 673.20, 673.21, 673.22, 673.23, 673.24 | Obstetrical blood-clot embolism (irrespective of timing) |
| 674.00 | Cerebrovascular disorders occurring in pregnancy childbirth or the puerperium (irrespective of timing) |