
Abstract
Background:
Numerous studies have documented the strong inverse relationship between low-density lipoprotein cholesterol (LDL-C) levels and atherosclerotic cardiovascular disease (ASCVD). However, women are less likely to be screened for hypercholesterolemia, receive lipid-lowering therapy (LLT), and achieve optimal LDL-C levels.
Materials and Methods:
Data were extracted from a U.S. administrative claims database between January 2008 and December 2012 for patients with established ASCVD. The earliest date of valid LDL-C value was defined as the index date. Patients were followed for ±12 months from the index date and were stratified by gender, by baseline LDL-C level, and whether they were initially treated with a LLT then propensity score matched by gender using demographic and clinical characteristics. Both descriptive statistics and logistic regression models were used to explore the association of gender with the frequency of LDL-C monitoring, LLT treatment initiation in initially untreated patients, and prescribing patterns in initially treated patients.
Results:
A total of 76,414 subjects with established ASCVD were identified; 42% of the sample was women. In the unmatched cohort, 50.3% of men and 32.0% of women were prescribed a preindex statin (p < 0.0001). Among matched patients (n = 51,764), women initially treated with LLT were significantly less likely to receive a prescription for a higher potency LLT. Even among those with LDL-C levels above 160 mg/dL, women were more likely to discontinue LLT, odds ratio (95% confidence interval) 1.8 (1.2–2.3). Female gender and older age were significant predictors of discontinuation, and the potency of the index medication was the strongest predictor of dose titration. Initially untreated women were less likely to initiate LLT treatment than men, irrespective of index LDL-C levels (p < 0.0001).
Conclusions:
The observed disparities further reinforce the need for targeted efforts to reduce the gender gap for secondary prevention in women at high risk of cardiovascular disease.
Introduction
A
Despite compelling evidence from randomized control trials demonstrating that reduction in LDL-C levels (mainly with statins) is associated with a decrease in the cardiovascular outcomes for both high- and low-risk adults, 6 fewer than half of adults who qualify for lipid-lowering therapy (LLT) actually receive it. 8 A recent meta-analysis of 27 large statin trials corroborates that statins are equally effective at lowering LDL-C among men and women, translating to similar important reductions in cardiovascular events. 9 Despite this, numerous studies demonstrate that women are not only less likely to be screened for hypercholesterolemia but are also less likely to be treated and less likely to achieve optimal lipid goals, especially those in high-risk groups. 8,10 –12 However, with the widespread and growing use of statins, it is unknown if these gender-based disparities in lipid management persist in a large insured population.
The main objective of the study was to systematically examine gender differences in the use of LLT (statins and statin/ezetimibe prescription filled on the same day) in high-risk patients with established ASCVD in a large managed-care database.
Materials and Methods
Data source and patient identification
We performed retrospective analyses of individual demographic, diagnostic, treatment/procedure, and laboratory data that were extracted from a U.S. administrative and claims database associated with Optum Insight™ (OI; Eden Prairie, MN). The database consists of patient longitudinal records of enrollment, inpatient and outpatient medical claims, pharmaceutical claims, and laboratory results for over 45 million unique managed care members and maintains deidentified Health Insurance Portability and Accountability Act-compliant patient records of United Healthcare® (UHC) managed care enrollees in the United States (in all 50 states and the District of Columbia). OI maintains medical and pharmacy data, enrollment information, and linked laboratory results for a subset of enrolled patients. It also contains information about all outpatient prescription pharmacy services, including information about drug name, dosage, fill date, total medication supply for each fill, mail order status, financial information, and deidentified codes for patients and prescribers.
Demographics included age, gender, geographic location, urban versus rural designation based on baseline metropolitan statistical area, and type of health plan (EPO, HMO, POS, PPO, Other). Diagnoses were coded according to the International Classification of Diseases, Ninth Revision Clinical Modification (ICD-9-CM) codes, and procedures according to the Current Procedural Terminology-4 (CPT-4) codes or Healthcare Financing Agency (HCFA) Common Procedure Coding System (HCPCS) codes. Pharmacy claims' data included drug name, dosage, drug strength, fill date, days of supply, cost, and deidentified patient and prescriber codes. For about 30% of the enrollees, the database also contained information on laboratory results, mainly from blood-based tests. Patients were identified for study inclusion if they had had at least one valid LDL-C measure during the study period (January 1, 2008 through December 31, 2012), defined as values in the range of 50–600 mg/dL, if they were ≥18 years on the date of the first available LDL-C assessment (index date), were enrolled in a health plan for at least 12 months before and after the index date, and had codes indicative of a high risk of cardiovascular events within the 12 months preceding the index date. These were defined as the presence of (1) established coronary heart disease (CHD), including acute myocardial infarction and unstable angina; (2) clinical history of CHD, as manifested by stable angina or the need for coronary artery procedures; or (3) disease(s) that confer high risk for CHD events (CHD risk equivalents), including atherosclerotic diseases (significant carotid artery disease, peripheral arterial disease, or abdominal aortic aneurysm), and diabetes mellitus, defined as a medical claim with diabetes-related ICD-9-CM codes or ≥2 prescription claims for antidiabetic medications. The complete list of codes is available as Supplementary Table S1 (Supplementary Data are available online at
Patients were excluded if they filled a prescription, other than a statin or statin and ezetimibe prescribed on the same date, for lipid control. Excluded medications were prescription-strength niacin, fibrates, bile acid sequestrants, omega-3 fatty acids, any combination of these agents, or any other combination of medications containing a nonstatin or nonezetimibe lipid-lowering agent. Patients with underlying hepatic disease were not eligible for inclusion in this analysis, and those with missing or unknown gender or age were also excluded.
Patients were classified as initially treated or initially untreated based on a prescription record for LLT at any time during the 90 days before or on the index date (index medication), and this could include statin monotherapy, a fixed dose of statin/ezetimibe combination, or a loose pill combination of statin and ezetimibe when both prescriptions had the same fill date. The index medication and further LLT prescriptions filled during the 12-month postindex period were assigned to a 1–10 potency scale using a previously validated algorithm 13 (Supplementary Fig. 1).
Outcomes
The study assessed the frequency of LDL-C measurements for the entire postindex 12-month period, the proportion of initially untreated patients who started LLT in the postindex period, and the LLT prescribing pattern for initially treated patients in a 12-month postindex period based on the proportion of patients who (1) received constant treatment (a drug within the same potency level as the index medication); (2) received a dose escalation (a drug at a higher potency level than the index drug); (3) received a dose reduction (a drug at a lower potency level than the index medication); (4) discontinued treatment (no longer received any statin and/or ezetimibe index treatment with a gap of 120 days since the previous fill); and (5) discontinued for at least 120 days from the previous fill and then restarted with a drug at the same potency level as the index medication.
Statistical analyses
For the analyses, eligible patients were stratified by gender and assigned to one of five groups based on their index LDL-C level (<70, 70–99, 100–129, 130–159, and ≥160 mg/dL). Within each of the five LDL-C categories, patients were further stratified as initially treated or initially untreated with LLT. The similarity in the covariate distribution of the matched patients for the five LDL-group strata is shown in Supplementary Tables S2A-S2E and Supplementary Table S3. To ensure that male and female patients within each of these stratified groups were similar with respect to demographic and clinical characteristics, we used propensity score matching (1:1 ratio) with a greedy match algorithm having a maximum caliper of 0.1. The probability model used in the propensity score matching was a stepwise logistic regression model predicting sex with potential covariates, including demographics, clinical covariates, region (West, Midwest, Northeast, South), insurance product type (EPO, HMO, POS, PPO, Other), index LDL-C, index year, and the Charlson comorbidity score. The exit and enter level was set at 0.01. Propensity score matching was chosen as a method to select male–female populations with similar average population characteristics across over 40 demographics and comorbidity dimensions measured in this study, as has been validated in prior studies. 14,15 Matching quality was assessed by comparing the population distributions of the demographics and comorbidities using the Kruskal–Wallis test (interval variables) and chi-square tests (categorical variables). Preindex statin therapy was not included as a matching variable because this was one of the study endpoints.
Overall descriptive statistics of the preindex demographics, LDL-C index value, preindex statin usage, and clinical comorbidities (based on a Deyo–Charlson Comorbidity Score, Supplementary Table S3) 16 for the initially treated and untreated cohorts during the preindex period were compared between genders stratified by the index LDL-C level category. For each LDL-C baseline stratum, gender differences in the proportion of subjects initially untreated but subsequently initiated with LLT treatment were calculated and gender differences in the distinct medication use parameters were calculated for treated patients. The Kruskal–Wallis test (interval variables) and the chi-square test (categorical variables) were used to test for statistical significance. Statistical significance was set as a two-sided p-value of 0.05. Gender differences in the likelihood of an LDL-C testing in the postindex period were also computed.
Finally, adjusted predictive models to identify significant predictors of pattern of medication use were constructed using full (all covariates included) and stepwise unconditional logistic regression models. Only clinically significant variables and those variables with a statistically significant contribution to the model (p < 0.01, inclusion and exclusion threshold) were retained in the stepwise models. Demographic variables included as covariates were age, gender, geographic location, urban versus rural designation based on baseline metropolitan statistical area, type of health plan, and index year. Clinical covariates included Deyo–Charlson Comorbidity Index, noncardiovascular comorbid health conditions (e.g., chronic kidney disease, depression, anemia, obesity), and cardiovascular or atherosclerotic comorbidities (e.g., hypertension, heart failure, peripheral vascular disease, angina pectoris, prior myocardial infarction, cardiac arrhythmias). For each model, variable regression coefficients, odds ratios (OR), 95% confidence intervals (CIs), Wald chi-square, and p-values were calculated. All analyses were performed with SAS® version 9.3 (SAS Institute, Inc., Cary, NC).
Results
A total of 76,414 patients (31,859 women and 44,555 men) were eligible and included in the analysis. The characteristics of the study sample are shown in Table 1. The average age of the study sample was 55.0 years (SD 9.7) with a range of 18–84 years. For the total unmatched population, 42% of the selected patients were female; the mean index LDL-C levels were higher among women than men (111.4 ± 35.8 mg/dL vs.100.6 ± 34.5 mg/dL; p < 0.0001), and there was a higher proportion of men who were prescribed a preindex statin (50.3% vs. 32%; p < 0.0001). The stratified analysis according to index LDL-C groups showed that female patients in the groups with lower LDL-C (up to 129 mg/dL) were younger and had slightly higher index LDL-C values (p ≤ 0.0001 for all comparisons). In addition, women were more likely to be in the higher LDL-C groups than men (Fig. 1). For all LDL-C groups, the proportion of women who were prescribed a preindex statin was lower than for men and they had higher mean Deyo–Charlson comorbidity index scores. There were no significant differences in demographic and clinical characteristics between genders in the matched sample (51,764 patients; 25,882 females and 25,882 males), the population that was used for all further analyses.

Distribution of index low-density lipoprotein cholesterol (LDL-C) by gender in the total unmatched sample.
Significant p-values are in bold.
Not included as a matching variable because it was one of the study endpoints.
CI, confidence interval; LDL-C, low-density lipoprotein cholesterol; SD, standard deviation.
Patterns of care and medication use in initially treated patients
Patterns of care among those who were initially treated with LLT are shown in Table 2. Analyses revealed that the potency of the index LLT used was on average significantly lower for women than men, irrespective of the LDL-C group (p < 0.05 across groups). There were no significant differences in the percentages of men and women with an increase or decrease in dose with respect to the index medication during the 12-month postindex study interval for any of the LDL-C groups. Discontinuation of LLT treatment was higher for women than men in all index LDL-C groups. With the exception for the group with levels of 130–159 mg/dL (p = 0.0729), this finding was statistically significant across the LDL-C groups (p < 0.05). Women who were initially treated and had lower index LDL-C levels (<70 and 70–99 mg/dL groups) were significantly more likely to restart LLT during the postindex study period compared with men (p < 0.0093 and p = 0.0005, respectively). There were no gender differences in monitoring of postindex LDL-C levels for any of the LDL-C groups, with the exception of the ≥160 mg/dL group, favoring women (p = 0.0072).
Significant p-values are in bold.
Not included as a matching variable because it was one of the study endpoints.
Throughout the study period (four quarters).
LLT, lipid-lowering therapy.
Patterns of care and medication use in initially untreated patients
The proportion of women who were started on LLT during the course of the postindex study interval was significantly lower than men in each of the five initially untreated index LDL-C groups (p < 0.0001) (Fig. 2). Monitoring of postindex LDL-C levels was done significantly less often for women than men in the index LDL-C <70 mg/dL (52.5% vs. 59.3%; p = 0.0034) and 70–99 mg/dL groups (48.8% vs. 51.8%; p = 0.0082), with no significant differences in monitoring between men and women with index LDL-C values >100 mg/dL.
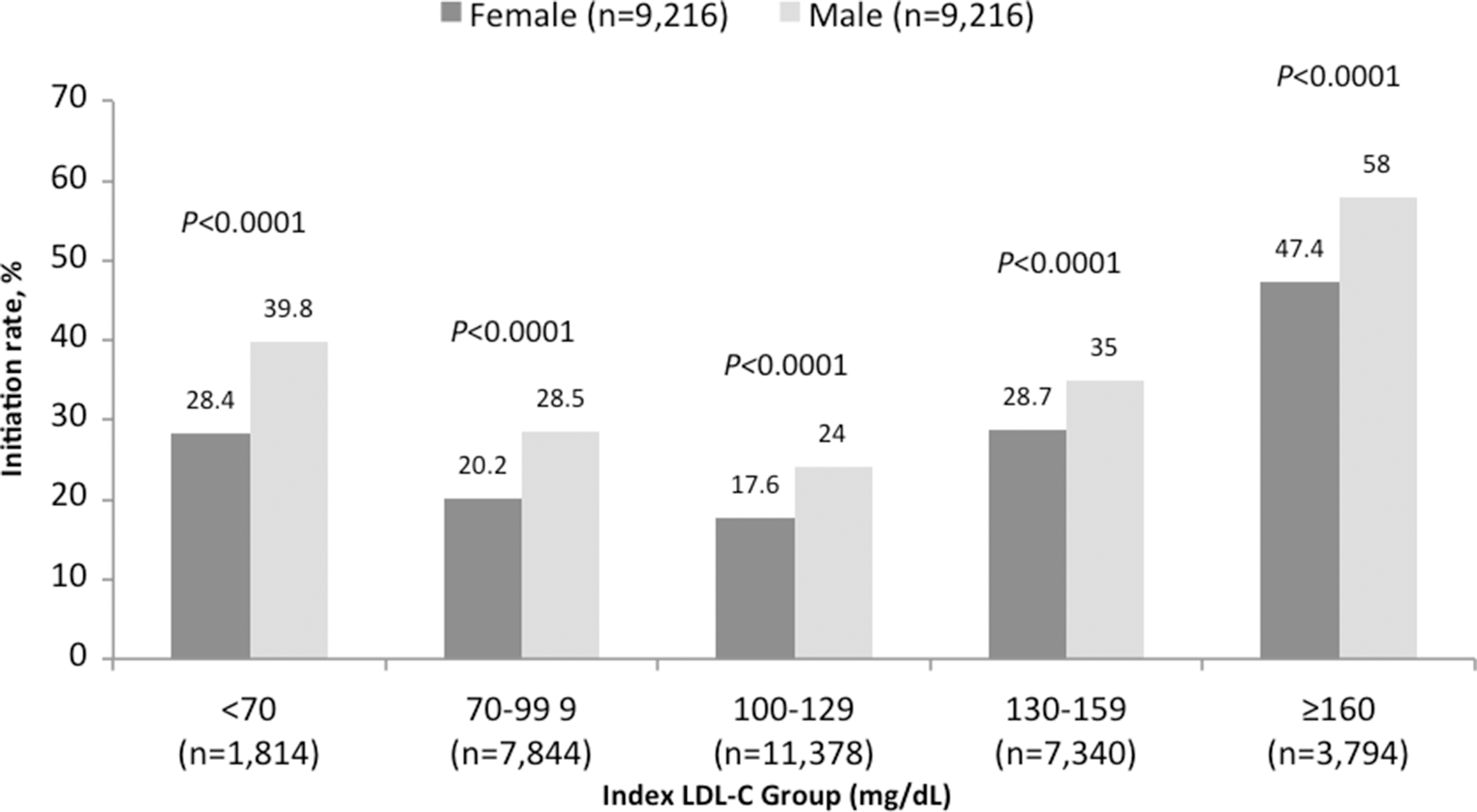
Initiation of lipid-lowering therapy by gender and index LDL-C level among initially untreated patients.
Predictors of care and medication use in initially treated patients
In general, the results of the full regression models were consistent with the ones obtained with the stepwise regression models. Summary results from the multivariable, stepwise logistic regression for initially treated patients are shown in Table 3. Women in all but the 130–159 mg/dL LDL-C group were more likely to discontinue LLT (p < 0.001 for each of the four groups), although the OR for the 130–159 mg/dL group was directionally consistent with this trend (OR = 1.17; 95% CI: 0.94–1.47). Moreover, older patients were less likely to discontinue for all but the ≥160 mg/dL LDL-C group (p < 0.001 for each group). Gender differences in restarting LLT treatment after ≥120 days of discontinuation were observed only in the LDL-C 70–99 mg/dL group, where women were more likely to restart LLT (OR = 1.2; 95% CI: 1.0–1.4).
Displaying the OR, 95% CI, and p-value for the variables that were required in all stepwise regression models. Other variables could have been included in the models depending on the results of the stepwise selection.
Significant p-values are in bold.
OR, odds ratio.
The strongest predictor of uptitration of LLT dose was the index medication potency (p < 0.0001 for all five LDL-C groups), with higher index potency associated with a lower likelihood of further dose increases. Moreover, dose increases were less likely to be recorded for women in the 70–99 mg/dL LDL-C cohort (OR = 0.86; 95% CI: 0.75–0.97) and the 100–129 mg/dL group (OR = 0.79; 95% CI: 0.68–0.92). Conversely, higher potency of index LLT was associated with a significantly higher likelihood of downtitration in doses for all five of the LDL-C groups (p < 0.0001 for all groups). In addition, a decrease in LLT dose during the follow-up interval was significantly more likely for women in the 70–99 mg/dL group compared with men (OR = 1.3; 95% CI: 1.1–1.6). However, a similar pattern was not evident for the four other LDL-C index groups.
Gender, age, index LDL-C level, and potency of index LLT were generally not significant predictors for frequency of postindex lipid assessment.
Predictors of care and medication use in initially untreated patients
The multivariable, stepwise logistic regression model for patients who were initially untreated revealed that gender, age, and index LDL-C levels were significant predictors for initiation of LLT (Table 4). The odds of having started LLT during the 12-month follow-up period in women were less than half that of men (p < 0.0001 for all five LDL-C cohorts), with ORs varying between 0.58 and 0.76 across LDL-C cohorts. Moreover, older patient age was associated with an increased likelihood of initiating LLT in all five LDL-C cohorts (p < 0.0001), and higher index LDL-C levels were also predictors of treatment initiation in all LDL-C cohorts (p < 0.0001), except in the group with the lowest index levels (<70 mg/dL).
Displaying the OR, 95% CI, and p-value for the variables that were required in all stepwise regression models. Other variables could have been included in the models depending on the results of the stepwise selection.
Significant p-values are in bold.
The main predictors of the frequency of postindex LDL-C assessment at follow-up were older age (p < 0.01 for all categories) and an index LDL-C level ≥70 mg/dL (p < 0.05 across the four corresponding cohorts).
Discussion
In a large, contemporary managed care cohort of high-risk patients with established ASCVD, we found significant disparities by gender in the use, intensification, and discontinuation of LLTs. Overall, women were more likely to have higher index LDL-C levels compared with men; yet, even after propensity matching for CVD risk, women were less likely to initiate LLT. Among treated patients, women received lower potency LLT, irrespective of index LDL-C levels. Women were also more likely to discontinue LLT during the study period.
It is notable that high-risk women with ASCVD in our cohort were more likely to have LDL-C >130 mg/dL, compared with men. However, and despite their overall higher LDL-C levels compared with men, fewer women overall were already being treated, and, in initially untreated women, women were less likely than men to have treatment initiated in the postindex period. Our findings are complementary to other studies that found that high-risk women are less likely to be treated with LLT 17 –19 and further add to the literature by showing that women are less likely to receive lipid intensification for high LDL-C levels and are more likely to discontinue LLT. For example, one study performed in primary care centers in Sweden in 5080 patients 60–90 years old with peripheral arterial disease found that preventive use of LLT was higher among men (OR = 1.3; 95% CI: 1.1–1.5). 17 Similarly, a prospective observational study conducted in Europe in 22,028 patients at high cardiovascular risk found that women received LLT less frequently for secondary prevention than men (68.2% vs. 73.1%). 18 Our results are also in line with studies performed in patients with diabetes mellitus, which observed that women are at a higher risk of not having treatment initiated and less likely to receive LLT than men. 12,20
Another important finding in our study was that both women in whom LLT was initiated and women who were already being treated were prescribed lower potency medications compared with men, irrespective of their LDL-C index levels. This result is in agreement with data from a recent study carried out in 2237 Chinese patients in secondary and tertiary hospitals being treated with statin therapy for dyslipidemia, which showed that among very high-risk groups (with CHD, ischemic stroke, peripheral artery disease, and diabetes mellitus), women were less likely to be prescribed moderate or high doses of statins than men (59.6% vs. 66.4%). 21 Our study further documents this finding in the outpatient setting among high-risk women who are undertreated for hyperlipidemia. Although not assessed directly in our study, the use of lower potency LLT could, in part, explain the lower likelihood of achieving optimal LDL-C treatment goals for women with ASCVD. 21 –26 In light of the recently released AHA/ACC prevention guidelines that recommend the use of high potency, fixed-dose statin therapies for adults with ASCVD, 13 our study highlights areas for improvement that are necessary to increase guideline adherence for women.
Possible explanations for the observed gender disparities in treatment and control of hypercholesterolemia in female patients are numerous and may include an underestimation of the true cardiovascular risk by physicians and also by patients themselves, 10,27 –29 a lower adherence to statins among women, 30 –32 and possibly a higher incidence of side effects leading to discontinuation of LLT among women. 33,34 In fact, higher intolerances to statins among women (particularly statin-induced myopathy) have been suggested in the literature, 35 –37 perhaps explaining the lower potency of statin prescribing patterns as well as the higher rates of statin discontinuation among women in our sample. Large statin trials have traditionally underrepresented women and often lack gender-specific analyses. A large recent meta-analysis, however, highlights that—even for primary prevention—statins are equally efficacious and safe for men and women. 9 However, more studies exploring a gender-specific response to LLT and developing well-tolerated drugs for women are needed.
Our results should be interpreted in the context of the AHA/ACC guidelines for the secondary prevention. The 2007 and 2011 AHA/ACC guidelines for CVD prevention for women recommend LDL-C lowering to <100 mg/dL with a suggested level of 70 mg/dL for women at a very high risk of a recurrent event. 27,38,39 Our results show that few women met these guideline recommendations during the study period. The 2013 AHA/ACC prevention guidelines recommend eliminating target LDL-C goals for high-risk patients with established ASCVD and recommend treatment with a high potency statin, irrespective of LDL-C levels. 13 By eliminating routine measurements of LDL-C and instead focusing on the use of the higher potency drugs, it remains to be determined if gender-based treatment gaps will be narrowed. However, statin intolerances and subsequent drug discontinuations will still need to be monitored.
Several potential limitations should be considered in the interpretation of these results. First, this was a retrospective analysis of data from an administrative claims database, which can introduce errors associated with coding. Our study represents a large sample of men and women who remained insured by a large managed care plan during the study period, thereby limiting generalizability to other populations not included in the geographic regions of the health plans included in the OI database. Moreover, this study was designed to examine gender differences in treatment patterns associated with prescriptions for a statin and or statin/ezetimibe combinations, but patients might have been treated with other LLT agents to treat hypercholesterolemia or other atherogenic lipids (such as triglycerides) or be on nonmedical interventions that could affect LDL-C levels, such as dietary modifications and physical activity. Similarly, there may be other systematic factors associated with gender that are not captured in this analysis and that might affect decisions about LLT and LDL-C goal attainment, such as socioeconomic status, race, ethnicity, and source of care (e.g., primary care vs. specialty care). We were also unable to account for reasons for discontinuation of statin therapy, including drug side effects, given the administrative nature of our database.
Conclusions
Despite higher baseline LDL-C levels, women continue to be less likely to have LLT initiated and to receive higher potency LLT, but are also significantly more likely to discontinue medication despite contemporary evidence supporting the beneficial effects of LLT for risk reduction of ASCVD in both men and women. These observed gender disparities reinforce the need for increased provider awareness of cardiovascular risk among women, including the need for assessment and targeting of interventions to address barriers to lipid screening, treatment, and monitoring, particularly among high-risk women.
Footnotes
Acknowledgments
Medical writing support was provided by Mònica Gratacòs, MD, PhD, Carole Alison Chrvala, PhD, and Bejal Joshi, MSc, of Plush Communique Limited. The study was funded by Merck.
Authors' Contributions
Fatima Rodriguez contributed to study conception, data interpretation, and article writing. Temitope O. Olufade contributed to study conception and article revision. Dena R. Ramey contributed to study conception and article revisions. Howard S. Friedman and Prakash Navaratnam contributed to study design, data analyses, article preparation, and article revisions. Kim Heithoff contributed to study design and article preparation. JoAnne M. Foody contributed to study conception, study design, and manuscript preparation.
Author Disclosure Statement
Dr. Foody serves as a consultant to Merck, Pfizer, Bristol Myer-Squibb, Sanofi, and Astra Zeneca. Drs. Navaratnam and Friedman have received consultant honoraria from Merck & Co., Inc. Drs. Olufade, Ramey, and Heithoff are employees or former employees of Merck Sharp & Dohme Corp., a subsidiary of Merck & Co., Inc. Dr. Heithoff owns stock in Merck Sharp & Dohme Corp. Dr. Rodriguez has no conflicts to report. Dr. Foody is now a Merck employee and served as Dr. Rodriguez's research mentor at the time of the study at the Brigham and Women's Hospital/Harvard Medical School.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.