
Abstract
Background:
Whether reproductive factors are associated with coronary artery disease (CAD) has been debated. The aim of this study was to investigate etiologic associations of a wide range of reproductive factors of women with the presence of angiographic obstructive CAD.
Materials and Methods:
Study data were obtained from a nationwide registry that enrolled 687 Korean women (59.9 ± 11.4 years) with chest pain undergoing invasive coronary angiography (ICA). Obstructive CAD was defined as ≥50% luminal stenosis of one or more epicardial coronary arteries in ICA. Information on reproductive history, including ages at menarche and menopause, duration of reproductive capacity, number of pregnancies, hormonal replacement therapy, and history of twin pregnancy, was obtained using a standardized questionnaire.
Results:
A total of 178 women (25.9%) had obstructive CAD. Multivariable logistic regression analysis identified that later age at menarche (odds ratio [OR] = 1.265, 95% confidence interval [CI] = 1.064–1.504, p = 0.008, per year) and increased number of pregnancies (OR = 1.223, 95% CI = 1.026–1.457, p = 0.025, per pregnancy) were the independent predictors of obstructive CAD even after controlling for potential confounders, including age, diabetes mellitus, hypertension, dyslipidemia, renal function, high-density lipoprotein level, white blood cell count, hemoglobin, and E/e’.
Conclusions:
Later age at menarche and increased number of pregnancies may be reproductive risk factors for angiographic obstructive CAD, suggesting the important role of hormonal status in the development of CAD.
Introduction
I
Most of the previous studies investigating the association between reproductive factors and CAD are big epidemiological outcome studies. Although invasive coronary angiography (ICA) is the gold standard for the detection of CAD, the invasive nature of ICA limits its use clinically. Therefore, the impact of reproductive factors on angiographic CAD has been scarcely addressed. To the best of our knowledge, there has been only one study that examined whether the lifetime exposure of endogenous estrogen was responsible for the severity of CAD assessed by ICA. 16 Recently, the KoRean wOmen'S chest pain rEgistry (KoROSE), a prospective, nationwide multicenter registry, was established to investigate the clinical characteristics and outcomes of CAD in Korean women. Women with chest pain referred for ICA were enrolled in the registry.
The present study was conducted to determine whether reproductive factors of Korean women can predict obstructive CAD in ICA using data obtained from the KoROSE.
Materials and Methods
Study population
Data from the database of KoROSE were used. Twenty-nine cardiac centers in Korea participated in the registry. At participating sites, consecutive female patients aged 20 years and over, admitted with chest pain and referred for elective ICA, were asked to register into the database. Patients with end-stage renal disease, chronic obstructive lung disease, primary pulmonary hypertension, malignancy, and autoimmune disease were excluded. Between February 2011 and October 2013, a total of 687 women were registered into the database and analyzed in this study. Demographic characteristics, including age and body–mass index (BMI), and traditional risk factors, including history of hypertension, diabetes mellitus, dyslipidemia, and ischemic heart disease, were obtained. BMI was calculated by weight (kg)/height (m2). Diabetes mellitus was defined by a previous history of diabetes mellitus or antidiabetic medications. Hypertension was defined by a previous history of hypertension or antihypertensive medications. Dyslipidemia was defined by a previous history of dyslipidemia or antidyslipidemic medications. The information on women's reproductive life, including age at menarche and menopause, the length of reproductive period, the number of pregnancies, and a history of hormonal replacement therapy (HRT)/twin pregnancy, was obtained using the standardized questionnaire at initial admission for ICA. The number of subjects who answered each question was n = 410 for age at menarche, n = 321 for menopausal age, n = 478 for the number of pregnancies, n = 583 for HRT, n = 57 for HRT duration, and n = 511 for twin pregnancy. Age at menarche was defined as the age at the start of menstruation. Menopausal age was defined as the age at the last menstruation for natural menopause or age at hysterectomy or bilateral oophorectomy for surgical menopause. The duration of reproduction was defined as the number of years between age at menarche and menopause. The number of pregnancies is the sum of the number of live-born children, miscarriages, abortions, and stillborn children. Blood samples were collected after overnight fasting to obtain baseline data for laboratory tests. All data were entered in an electronic web-based computerized database. This study protocol was reviewed and approved by the Institutional Review Board of each center, and written informed consent was obtained from each study subject.
Definition of obstructive CAD
The degree of epicardial coronary artery stenosis was assessed in ICA. Obstructive CAD was defined as a ≥50% stenosis of one or more major epicardial coronary arteries. After ICA, all management strategies for CAD, including coronary revascularization and medications, were chosen at the attending physicians' discretion.
Statistical analyses
Data are expressed as mean ± standard deviation for continuous variables and percentages for categorical variables. Clinical characteristics of patients with and without obstructive CAD were compared with Pearson's chi-square tests for categorical variables or Student's t tests for continuous variables. Multivariable binary logistic regression analysis was performed to determine independent variables associated with obstructive CAD. Significant reproductive factors in univariate analyses were separately entered into multivariable analyses. Age, diabetes mellitus, hypertension, dyslipidemia, estimated glomerular filtration rate, high-density lipoprotein (HDL) cholesterol, white blood cell count, hemoglobin, and ratio of mitral peak velocity of early filling to early diastolic mitral annular velocity (e’) (E/e’ ratio) were adjusted in each multivariable model. Age at menarche was categorized into <14, 15–16, 17–18, and >18 years, and the incidence of obstructive CAD according to the categorized age at menarche and the number of pregnancies were estimated by the chi-square test of linear by linear association. A two-tailed p < 0.05 was considered statistically significant. All data were analyzed using SPSS for Windows 18.0 (IBM Co., Armonk, NY).
Results
Of 687 study women, 178 (25.9%) had obstructive CAD. Baseline characteristics with comparisons between women with and without obstructive CAD are shown in Table 1. Women with obstructive CAD were older and had more traditional risk factors, including diabetes mellitus and hypertension, than those without. Women with obstructive CAD took more cardioprotective medications, including aspirin, beta-blocker, angiotensin receptor blocker, and statin, than those without. In baseline laboratory examinations, high white blood cell count, low hemoglobin, high fasting glucose, low HDL cholesterol, and high triglyceride and low renal function were associated with obstructive CAD. Among echocardiographic parameters, left ventricular ejection fraction was lower, the left atrium was larger, and E/e’ was higher in women with obstructive CAD than in those without.
BNP, brain natriuretic peptide; CAD, coronary artery disease; CRP, C-reactive protein; eGFR, estimated glomerular filtration rate; HDL, high-density lipoprotein; LA, left atrial; LDL, low-density lipoprotein; LV, left ventricular; RAS, renin–angiotensin system; WBC, white blood cell.
Reproductive factors of study patients are demonstrated in Table 2. Later ages of menarche and menopause, higher number of pregnancies, and lack of HRT were associated with the development of obstructive CAD. The duration of reproduction, the duration of HRT, and the incidence of twin pregnancy were not different between women with and without obstructive CAD.
HRT, hormonal replacement therapy.
Even after controlling for potential confounders, including age, diabetes mellitus, hypertension, dyslipidemia, renal function, HDL cholesterol, white blood cell count, hemoglobin, and E/e’, age at menarche (odds ratio [OR] 1.265, 95% confidence interval [CI] 1.064–1.504, p = 0.008) and the number of pregnancies (OR 1.223, 95% CI 1.026–1.457, p = 0.025) were significantly associated with obstructive CAD (Table 3). Old age, diabetes mellitus, and low HDL cholesterol level were other independent risk factors for obstructive CAD in the analysis (data not shown).
Each variable entered in binary logistic regression analysis separately. Age, diabetes mellitus, hypertension, dyslipidemia, estimated glomerular filtration rate, high-density lipoprotein cholesterol, white blood cell count, hemoglobin, left ventricular ejection fraction, and E/e’ were adjusted in each multivariable model.
IC, confidence interval; OR, odds ratio.
With increasing age at menarche, the incidence of obstructive CAD increased proportionally (p = 0.019) (Fig. 1). The more pregnancies a woman had, the greater she was at risk for obstructive CAD (p < 0.001) (Fig. 2).
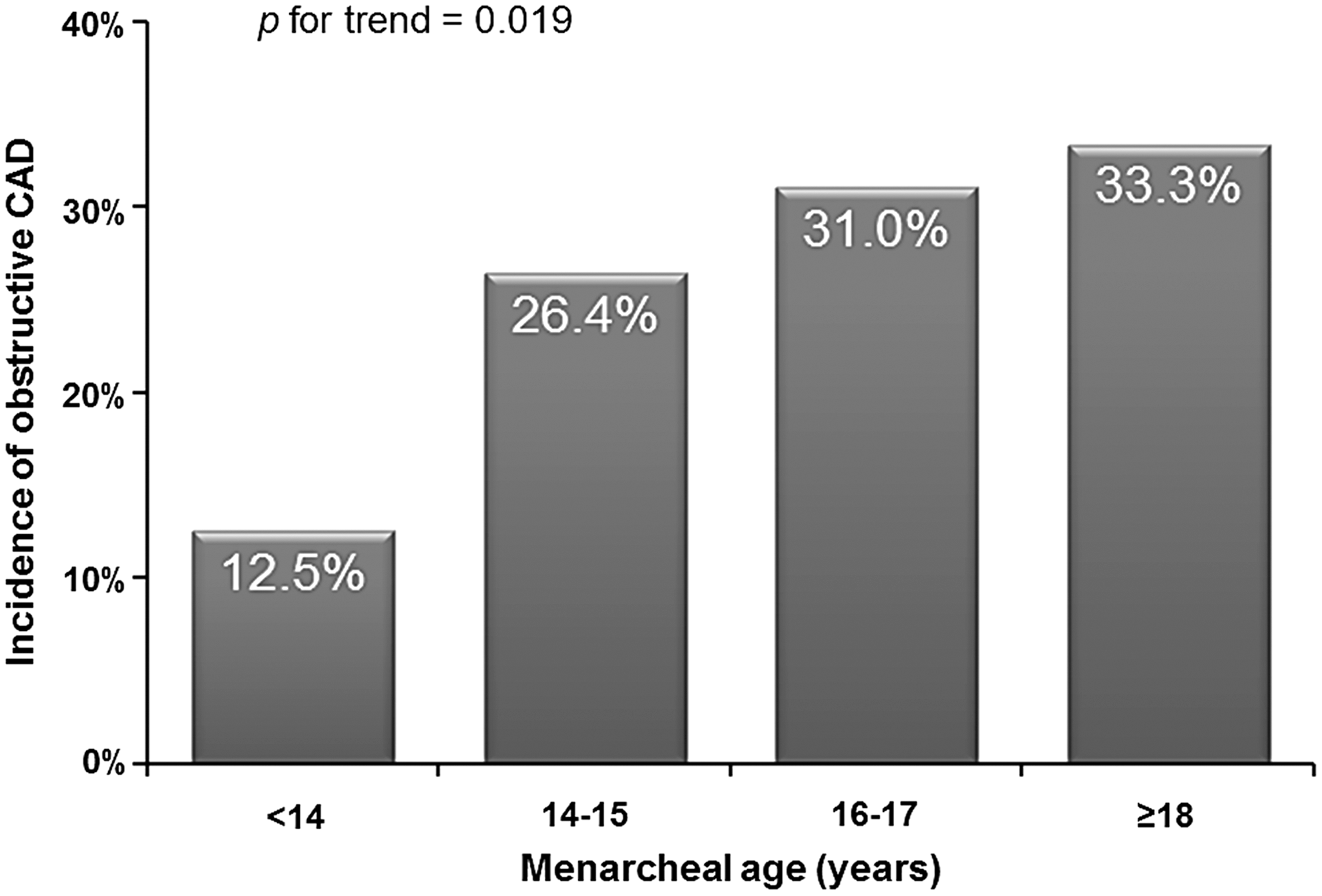
The incidence of obstructive CAD according to age at menarche. CAD, coronary artery disease.
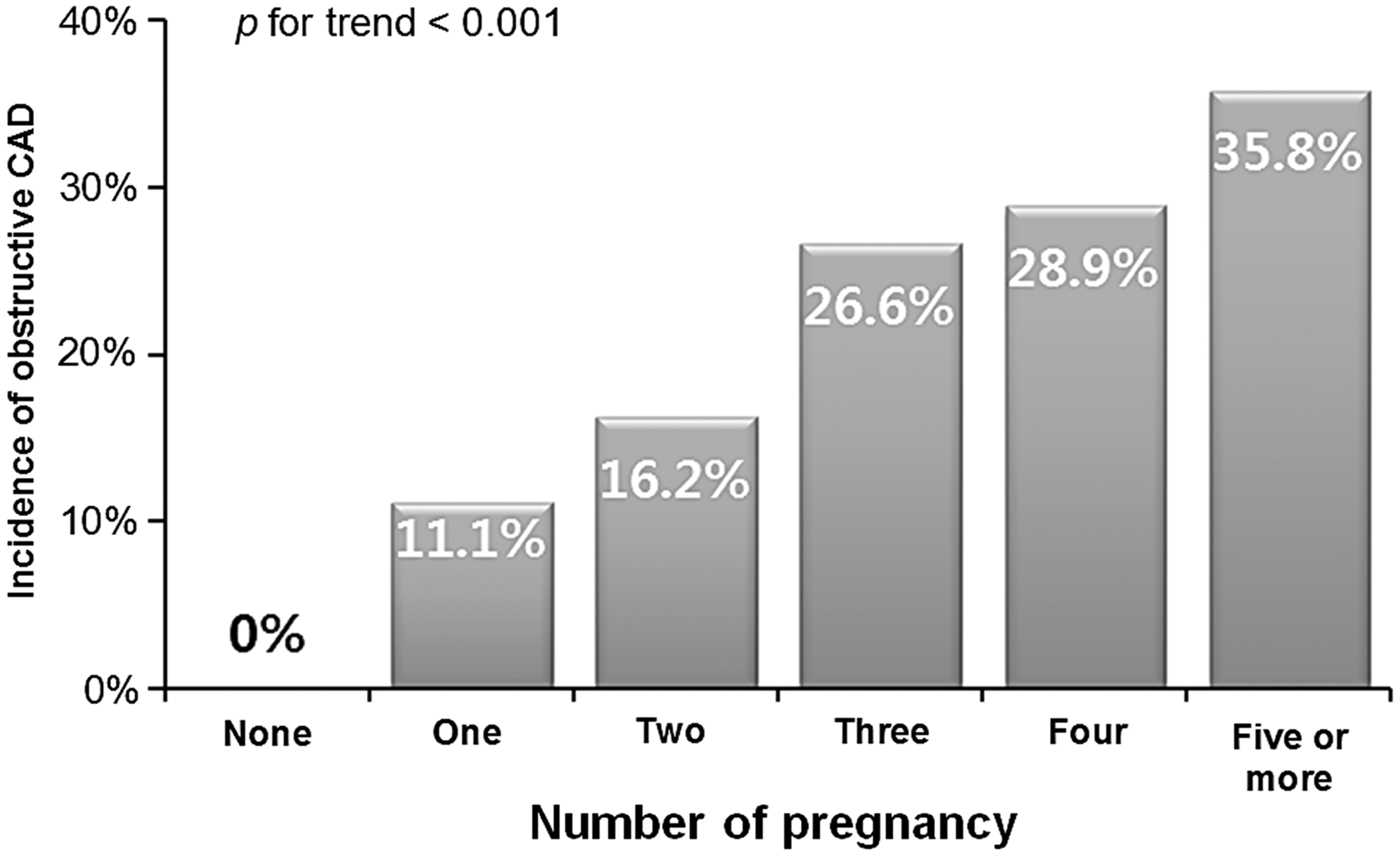
The incidence of obstructive CAD according to the number of pregnancies.
Study subjects were divided into two groups according to the median age at menarche (<16 years vs. ≥16 years) and the number of pregnancies (<4 times vs. ≥4 times). The clinical characteristics were compared between the two groups. Women with early menarche were younger than those with later menarche. The other clinical parameters were not significantly different between the two groups (Supplementary Table S1; Supplementary Data are available online at
Discussion
The present study assessed etiologic associations of a wide range of reproductive factors with the presence of obstructive CAD using data of Korean women who were referred for ICA. It showed that older age at menarche and increased number of pregnancies are independently associated with CAD. Other reproductive factors investigated, including menopausal age, duration of reproductive capacity, HRT, and history of twin pregnancy, were not associated with CAD in these analyses.
Many studies on the association between women's reproductive history and cardiovascular disease (CVD) with a large sample size have been conducted. However, studies using ICA in this scope have been scarce. Although ICA has been considered the gold standard in the diagnosis of CAD, invasiveness and cost limit its use in clinical practice. To our knowledge, there is only one ICA study of reproductive factors related to CVD. This same study analyzed 108 elderly Greek women and demonstrated that the severity of CAD and the development of angina or myocardial infarction correlated with time since menopause. 16 However, the sample size was relatively small, and the authors did not analyze the other reproductive factors. In this context, our study using ICA and considering a wide range of reproductive factors of 687 women is valuable and deserves attention. The results of our study may help understand the important role of hormonal status in the development of obstructive CAD in women, leading to better prevention and management of CAD.
Most of the prior studies have assessed the risk of reproductive factors in a separate report. Studies investigating multiple reproductive factors responsible for cardiovascular risk have been limited and yielded mixed results. A cross-sectional study of 568 postmenopausal women conducted in The Netherlands by Atsma et al. showed that the number of pregnancies and births and irregular menstrual cycle lengths are related to coronary artery calcification. 17 That result is consistent with ours. However, conversely, Gallagher et al. investigated 267,400 female textile workers in China and they showed that oral or injectable contraceptive use or induced abortion is not consistently associated with the development of ischemic heart disease or stroke. 9 These discrepancies among studies may be attributed to the difference in study population and assessment methods.
Results from previous studies regarding relationships between age at menarche and CVD are still inconclusive. Some previous studies have shown an increased cardiovascular risk with early age at menarche. A study by Jacobsen et al. with a large sample size of 19,462 American women showed an inverse relationship between age at menarche and mortality from ischemic heart disease. 6 A one-year delay in menarche was associated with 6.0% lower mortality from ischemic heart disease in that study. 6 Mueller et al. followed 34,022 Chinese women for 13.5 years and demonstrated that age at menarche is inversely correlated with risk of CVD mortality in nonsmoking women. 12 However, some other studies have shown no association between age at menarche and CVD. Colditz et al. investigated 119,963 American women with a 12-year follow-up and showed that there is no significant association between age at menarche and the development of coronary heart disease. 13 A study by Palmer et al. analyzed 858 cases of first myocardial infarction and showed that age at menarche is not related to the risk of myocardial infarction. 14 On the other hand, positive correlation between age at menarche and the risk of CVD has been reported. Cui et al. analyzed 37,956 Japanese postmenopausal women and showed that later age at menarche is associated with increased risk of mortality from stroke. This finding is in line with our results indicating that late menarche may be an unfavorable factor for CVD. 10 The mechanism underlying this association is still unclear. Our hypothesis is that the protective effect of estrogen may play a role in the prevention of the development of obstructive CAD. 8,16 However, our results should be viewed with caution in relation to aforementioned studies. The primary focus of our study was not the age at menarche, but a wide range of reproductive factors responsible for CAD. More important, our study population consisted of high-risk older women with suspected CAD, but not women selected from the general population. In addition, CAD was assessed using ICA, and analyses were adjusted for many confounders, including CVD risk factors. The potential risk of later age at menarche for the development of CAD requires further investigation.
Our results are in agreement with those of previous studies showing a positive association between the number of pregnancies and CVD. 7,18,19 Pregnancy is associated with increased incidence of traditional cardiovascular risk factors, such as hypertension, diabetes mellitus, and dyslipidemia. 19 –21 In addition, normal physiologic responses to pregnancy, such as upregulation of the renin–angiotensin–aldosterone system, increased insulin resistance, and endothelial dysfunction may result in cumulative derangements with repeated pregnancies that eventually lead to increased CVD risk. 7,19 Another possible mechanism behind the association between parity and CVD in women is reduced lifetime exposure to estrogen by pregnancy because pregnancy resets ovarian function. 22 Furthermore, complications associated with pregnancy, including preeclampsia, preterm delivery, and low birth weight, have been suggested as factors for maternal cardiovascular risk. 23
Several studies demonstrated that premenopausal women have a lower incidence of CVD than men and postmenopausal women, suggesting the cardioprotective role of endogenous reproductive hormones. 8,16 However, as for exogenous hormones, it is generally accepted that HRT increases risk of CVD, especially in elderly women with cardiovascular risk factors. 24,25 Although our study showed that HRT is likely to have a protective effect on the development of obstructive CAD (p = 0.101), it should be considered that there was a possibility that women who have risk factors did not take exogenous hormones according to the recommendations of current guidelines. 26 In addition, ethnic differences in the biological effect of exogenous hormone between Asian and Western women could not be ruled out because most of studies on this issue have been performed in Western coutries. 24,25 Further studies are needed to examine the effect of HRT on cardiovascular outcome in postmenopausal Asian women.
Old age, diabetes mellitus, and low HDL cholesterol levels were other independent risk factors of obstructive CAD in our study (data not shown). These results are similar to those of men in terms of traditional risk factors, which are consistent with those of other reports. 27
In our study, the mean age at menarche was 15.9 years, which is similar to those of other Korean studies of middle-aged or elderly women. 28,29 However, the age at menarche of old Korean women was somewhat later compared with that of other similar studies of women conducted in other countries. 6,12,13,30 This difference may be attributed to cultural difference in calculating the age. There is an idea known as Korean age, which basically adds one or two more years to what is considered a person's birth date in Western societies, depending on the time of the year. In Korea, a baby is one year old at birth and two years old on the first day of the new year regardless of what month the baby was born the previous year. Essentially, the entire Korean population ages one year on New Year's Day. In our study, the mothers recalled their age at menarche based on the Korean age. Therefore, age at menarche may have been one or two years later in our study compared with that of studies conducted in other countries. In addition, there may be racial differences in age at menarche, which tends to be later in Asian women 12,30 than American women. 6,13
The present study has several limitations. First, this is a cross-sectional study and may be affected by selection bias, and the cause–effect relationship was not ascertained. Second, data on the reproductive factors were obtained through a questionnaire, and response rates to each questionnaire were different, which may have contributed to recall errors. 31 Third, our study can only establish associations of reproductive factors with the presence of obstructive CAD, but not clinical outcomes. Fourth, since our study was performed specifically on elderly women referred for ICA, generalization of our results to other populations is difficult. Last, the possibility of interactions between independent variables that may have influenced study results cannot be ruled out because we attempted to adjust as many variables as possible in our multivariable models.
Conclusions
The results of the present study using a nationwide registry of elderly Korean women demonstrated that later age at menarche and the increased number of pregnancies may be independently associated with the presence of obstructive CAD, suggesting an important role of hormonal status in the development of CAD.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.