
Abstract
Background:
Fewer than 50% of women who meet the medical/behavioral criteria for infertility receive medical services. Estimating the number of women who both meet the medical/behavioral criteria for infertility and who have pro-conception attitudes will allow for better estimates of the potential need and unmet need for infertility services in the United States.
Methods:
The National Survey of Fertility Barriers was administered by telephone to a probability sample of 4,712 women in the United States. The sample for this analysis was 292 women who reported an experience of infertility within 3 years of the time of the interview. Infertile women were asked if they were trying to conceive at the time of their infertility experience and if they wanted to have a child to determine who could be considered in need of services.
Results:
Among U.S. women who have met medical criteria for infertility within the past three years, 15.9% report that they were neither trying to have a child nor wanted to have a child and can be classified as not in need of treatment. Of the 84.9% of infertile women in need of treatment, 58.1% did not even talk to a doctor about ways to become pregnant.
Discussion:
Even after taking into account that not all infertile women are in need of treatment, there is still a large unmet need for infertility treatment in the United States.
Conclusion:
Studies of the incidence of infertility should include measures of both trying to have a child and wanting to have a child.
Introduction
B
Despite evidence that infertility is often distressing, fewer than 50% of women who meet the medical/behavioral criteria for infertility receive medical services. 11 Not all women who meet the medical/behavioral criteria for infertility, however, indicate that they are trying to or want to have a baby, 13 which suggests that some infertile women are not in need of treatment for infertility. Determining the number of women who both meet the medical/behavioral criteria for infertility and are trying to or want to have a baby is therefore a useful step to better estimate the potential need for infertility services among women in the United States. Identifying the unmet need for infertility services is important for formulating evidenced-based social policies concerning population health needs. 14 This paper therefore aims to provide an improved approach to estimating potential need for infertility services. By determining the proportion with potential need who have sought medical help, it is possible to determine the proportion with potential unmet need for infertility services.
Estimating the potential unmet need for infertility health services appears straightforward: Identify those who meet criteria for infertility, and subtract those who have already sought health services. In practice, however, the task is more complex. One reason for this complexity is that there is no scholarly consensus concerning how best to define and measure infertility. 15 –18 (See Gurunath et al. 19 for a review of issues involved in defining infertility). There is little agreement on the length of unprotected intercourse necessary before an infertility diagnosis is applied; different time frames may be appropriate depending on the research perspective, specific medical condition of interest, or discipline. Most medical professionals consider a couple to be infertile if they have failed to conceive after 12 months of unprotected intercourse (6 months if the woman is over the age of 35 years due to the greater need for prompt action). The 12- month criterion is based on evidence that 85% of noncontracepting women who regularly have heterosexual sex will conceive within a year. 20 This narrow time frame is useful in clinical settings because early detection helps maximize the effectiveness of treatment. A narrow time frame is therefore appropriate for studies of the need and unmet need for medical help. 15 Other researchers consider a couple to be infertile after two years of unprotected intercourse, arguing that the one-year interval may overestimate infertility because many “infertile” couples by the more restrictive definition will have conceived without medical help by the end of the second year. 16,21 Demographers, concerned with the prevalence of infertility in a population, take an even longer-range view, frequently using intervals of 5 or 7 years. 16,21
A second challenge involves identifying failure to conceive. From a medical perspective, the most desirable means of assessment would be clinical diagnosis, but this measure cannot be used for population estimates or for approximating the need for treatment because a clinical diagnosis is possible only if a woman has already talked to a doctor or contacted a clinic. 20 Some estimates therefore rely on “constructed” measures derived from contraception and birth histories. See, for example, the constructed “infertility” measure employed by the NSFG. 22,23 Other researchers rely on women's self-reports of periods of regular, unprotected intercourse of a certain duration. 13,22 The “duration” or “time to pregnancy” approach, recently applied by Thoma et al. 12 to a nationally representative U.S. sample, is an example of a self-report assessment method. Thoma et al. used NSFG data but based their estimate of infertility on noncontracepting women's self-reports of whether they were trying to have a baby, and if so, how long they were trying. Estimates of infertility based on self-reports have been found to be an efficient and appropriate method for estimating infertility at the community level. 20 Self-reports have also been found to be accurate when women are asked to recall past experiences of infertility. 24
A third challenge involves the meaning of potential need. One way to conceptualize need for treatment involves estimating those who seek treatment among those classified as infertile. Major surveys, such as the NSFG, measure infertility based on behavior (sex without contraception for twelve months without conception) without explicitly measuring attitudes towards pregnancy (i.e., trying to or wanting to conceive). Not all of those who meet criteria for infertility are trying to conceive, however. 13 Those who neither want to nor are trying to conceive do not have a potential need for infertility treatment even though they meet criteria for infertility. 22 Failure to include pregnancy intent may result in overestimation of unmet need for treatment because not all women classified as “infertile” by the clinical definition wish to have a child. 11,21,22,25
Some scholars have conceptualized women as infertile only if they say they are trying to become pregnant. 12,17 Restricting infertility to those who are trying to become pregnant may actually underestimate the need for fertility services because there is a substantial group of U.S. women who say they are “okay either way” rather than intentionally trying to become pregnant. 26 Many women who are “okay either way” go on to pursue infertility treatment, 13 thus implicitly expressing a felt need for fertility services. In addition, women who would like to have a child but do not perceive that they have access to treatment or have become “resigned” to infertility 15,27 may be hesitant to say that they are trying to get pregnant. Therefore, restricting potential need to only those with “intent” could underestimate need for treatment.
Demand for infertility treatment could be conceptualized as the proportion of couples who seek any kind of treatment for their fertility barriers. 13 Such a measure, however, ignores those who might want medical help but do not seek it because of financial or geographical barriers. Income, economic hardship, and access to private health insurance are barriers for some couples in the United States who want infertility services. 28 –32
Here, we propose a definition of potential need for infertility services that includes all women who meet the medical/behavioral criteria for infertility who also say they have been trying to become pregnant or who say they would like to have a(nother) child. The subset of women with potential need who have not talked to a doctor about getting pregnant constitutes those with potential unmet need for infertility services. An accurate estimate of the potential unmet need for infertility services is a first step toward creating and implementing policies that can address the unmet need for services. We use the National Survey of Fertility Barriers (NSFB) data to illustrate the utility of this approach.
Materials and Methods
Data
Our data come from a sample of 4,712 women ages 25–45 years from the NSFB, a national telephone survey designed to assess social and health factors related to reproductive choices and fertility among women in the United States. The first wave of data was collected between 2004 and 2006. Funding for the project was received from the Eunice Kennedy Shriver National Institute of Child Health and Human Development, and institutional review board approval was obtained from the Pennsylvania State University and the University of Nebraska–Lincoln. The random-digit-dial sampling of landline telephone numbers oversampled for minority women and women with a biomedical fertility barrier. The survey was conducted in Spanish and English. The sample design included a prenotification letter with a $1 or $2 cash incentive for all telephone numbers with address matches. A minimum of 10 follow-up contact calls were made to potential participants. The estimated response rate for the sample is 53%. Comparison of the NSFB and Current Population Surveys shows that the NSFB underrepresents lower educated women, and weights were adjusted accordingly when making population estimates.
33
Weighted results are nationally representative. Methodological information including the methodology report, introductory letters, interview schedules, interviewer guides, data imputation procedures, and a detailed description of the planned missing design is available at
Measures
Women were considered to have met criteria for infertility if they provided a “yes” answer to either of the following: (1) “Was there ever a time when you were trying to get pregnant but did not conceive within 12 months?” or (2) “Was there ever a time when you regularly had sex without using birth control for a year or more without getting pregnant? Women who answered “yes” to this second question were asked if they were trying to become pregnant, if they were currently trying not to become pregnant, or if they were “okay either way.” Those who said they were trying not to become pregnant were not counted as infertile and were removed from the sample. Women were also classified as ever-infertile if they reported having a pregnancy after a period of at least 12 months during which they were either trying to become pregnant or said they were “okay either way” and in which they were not breastfeeding.
Of the women in the sample, 292 (13.3%) of all ever-infertile women reported an infertility experience within 3 years of the date of their interview. The 3- year time frame was selected to make our study as comparable as possible with the NSFG. Those who said they were trying to become pregnant at the time of their infertility experience were classified as trying, Women who reported being “okay either way” were classified as not trying. “Wants another child” was measured by a single question, “Would you, yourself, like to have a(nother) baby?” (yes, 1; no, 0). Respondents were asked a series of questions about information-seeking, treatment-seeking, tests, and treatments related to infertility. From responses to these questions, we constructed variables for seeing a doctor, having tests, and receiving treatment. Anyone who meets the criteria for a higher level of medical services also meets the criteria for lower levels. Figure 1 depicts a flow chart for inclusion of women in the sample and into the various groups based on survey questions.
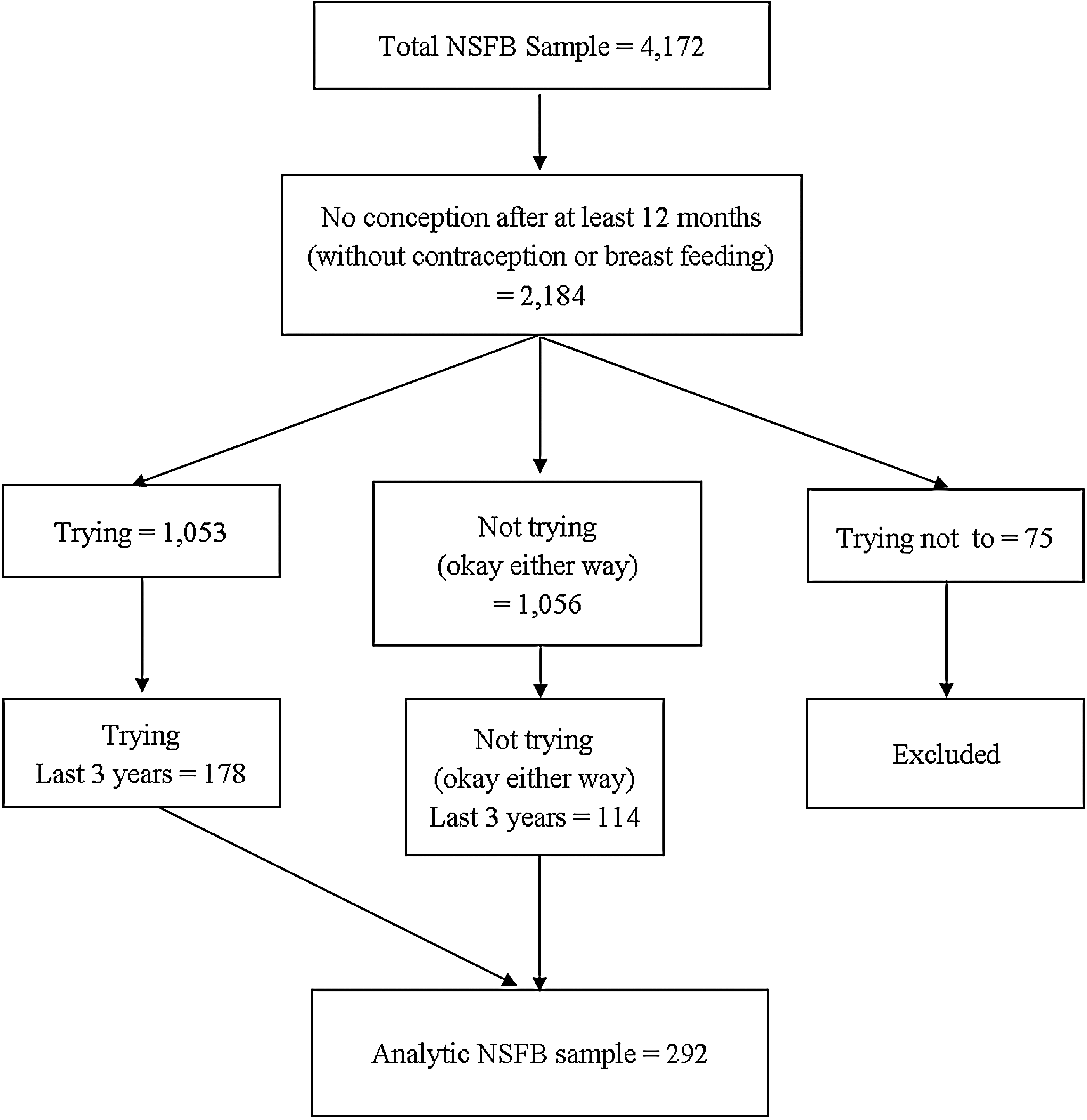
Flowchart for sample selection, National Survey of Fertility Barriers (NSFB).
Results
Table 1 displays descriptive statistics for the 292 women with an infertility experience in the last three years and compares demographics for our sample to those for the fecundity-impaired in the pooled 2002 and 2006–2010 cycles of the NSFG. The women in the analytic sample do not differ from fecundity-impaired women in the NSFG with regard to employment status, education, or residence in metropolitan areas. The analytic sample includes more women in the 25–29 and 30–34 years age ranges and more Black and Hispanic women than in the NSFG. This is not surprising, given that the NSFB oversample minorities and childless women who desired a child. The women in the analytic sample have somewhat higher family incomes than fecundity-impaired women in the NSFG. There are more married women and fewer cohabiting women in the analytic sample compared to the NSFG. Fewer analytic sample women have zero or three or more children compared with the NSFG. Note that, as other population-based studies have found, most infertile women in the United States have children. Not all women who said they were trying to have a child also said they wanted a child, and conversely, not all women who said they wanted a child indicated that they were trying to have a baby (Table 2). Of the 292 women who met criteria for infertility in the 3 years prior to the interview, 178 (61.0%) reported that they were trying to become pregnant at the time of the experience, and 202 (69.2%) reported that they desire a child. Collectively, 246 (84.2%) women indicated either that they wanted a baby or that they were trying to get pregnant and can thus be considered in potential need of services. The remaining 15.8% of women who were infertile by the medical/behavioral definition reported that they were neither trying to have a child nor that they desired to have a child and are therefore classified as not in need of services.
Significance was determined using a one-way chi-squared test with expected frequencies based on National Survey of Fertility Growth (NSFG) percentages.
Data source: National Survey of Fertility Barriers (2004–2006) and National Survey of Fertility Growth (2002–2010).
Chi-squared = 7.96, p = 0.005.
Women who said they were “okay either way.” Women who said they were trying not to become pregnant were removed from analysis.
Data source: National Survey of Fertility Barriers (2004–2006).
Table 3 shows a cross tabulation of the number of women who talked to a doctor, had tests, or received treatment by all possible combinations of “wanting another child” and “trying to become pregnant.” Of the 246 women who are in potential need of treatment (5.2% of the 4,712 women in the sample), 143 (58.1%) did not speak to a doctor, 167 (68.2%) did not have tests, and 199 (81.2%) did not receive infertility treatments and, depending on one's definition of treatment, could be considered to have unmet need for services. Using population weights based on the 2005 Current Population Survey March Supplement, we can estimate that in 2004–2006, 1,814,000 women in need of infertility services had not talked to a doctor, 2,125,000 had not had tests, and 2,534,000 had not received treatment.
Women who said they were “okay either way.” Women who said they were trying not to become pregnant were removed from analysis.
Data source: National Survey of Fertility Barriers (2004–2006).
Discussion
In 2004–2006, extrapolating from estimates based on the NSFB, 3,711,000 women in the United States had met criteria for infertility within the past 3 years. Of those women, 3,122,000 were either trying to get pregnant or indicated that they wanted a(nother) child but had not sought treatment, and can thus be identified as having potential need for infertility services. This is a smaller number than the population of women who were infertile by the medical/behavioral definition, but it is still a very large number. Our estimate that 42.9% of women had talked to a doctor is slightly higher than the 41.0% reported by NSFG, 11 likely due to the NSFG number including infertile women who were not trying to get pregnant. The findings presented here suggest a major discrepancy between the need for infertility services and accessing those services: fewer than half of infertile women who were trying to get pregnant or wanted a child had even spoken to a doctor, and only 18.8% had actually received medical treatment.
The proposed approach to estimating potential unmet need for infertility services is promising, but it also has limitations. First, the NSFB collected data only from a single cohort of women, those who were aged 25–45 years in 2004–2006, and data collection has not been continued on a regular basis. Additionally, the rapid increase of cell phone-only households raises concerns about coverage error for landline telephone surveys. 34,35 In addition, although the NSFB interviewed the partners of some of the women sampled, it does not include a random sample of men at risk for infertility. A further limitation is that, while the question about trying to become pregnant referred to the time of the infertility experience, the question about wanting a child referred to the time of the interview. It would have been preferable for both questions to refer to the same time period. Finally, the broad age range meant that most of the women met criteria for infertility before the 3-year window of this study, thus providing only a small, though representative, sample. Despite these limitations, the NSFB provided a nationally representative sample with sufficient questions to assess potential need and unmet need for infertility services.
The NSFG has been the most reliable source of data on infertility and use of infertility services for some time and has guided infertility policy in the United States for years. Unfortunately, our measure of need for services cannot be applied to the NSFG because it does not include a question comparable to the “trying to/trying not to/okay either way” question asked in the NSFB. Furthermore, the NSFB's measure of infertility is not directly comparable to the NSFG's definitions of “infertility,” “impaired fecundity,” and “current fertility problem.” Although it is possible to extrapolate to the NSFG based on our finding that 84.1% percent of women who are infertile are actually in need of services, it would be better to have a way to integrate the NSFB measure into the NSFG data because of its strengths, especially regular data collection over a long duration.
Conclusion
Incorporating intent (trying, wanting a child) into measures of potential need and unmet need for infertility services provides a more accurate assessment than previous approaches. Without incorporating childbearing intentions among infertile women, estimates of unmet need would be higher. Our estimate of unmet need in the United States, however, is still quite high. These findings have important policy implications to address unmet need, such as improved insurance coverage of patients in need of infertility services. Although some states mandate insurance coverage for infertility services, the costs of treatment remain prohibitively expensive for many couples. Future research should determine whether there are subgroups of women who are at higher or lower risk for unmet need for infertility medical services. Further investigation of the reasons women give for not seeking medical help for infertility would provide specific steps for reducing treatment barriers and thus furthering the important aim of helping infertile couples realize their reproductive goals.
Footnotes
Author Disclosure Statement
No competing financial interests exist.