
Abstract
Background:
Maternal glucose and weight gain are related to neonatal outcome in women with gestational diabetes mellitus (GDM). The aim of this study was to explore the influence of average third-trimester HbA1c and excess gestational weight gain on GDM neonatal complications.
Materials and Methods:
This observational study included 2037 Spanish singleton pregnant women with GDM followed in our Diabetes and Pregnancy Unit. The maternal HbA1c level was measured monthly from GDM diagnosis to delivery. Women were compared by average HbA1c level and weight gain categorized into ≤ or > the current Institute of Medicine (IOM) recommendations for body mass index. The differential effects of these factors on large-for-gestational-age birth weight and a composite of neonatal complications were assessed.
Results:
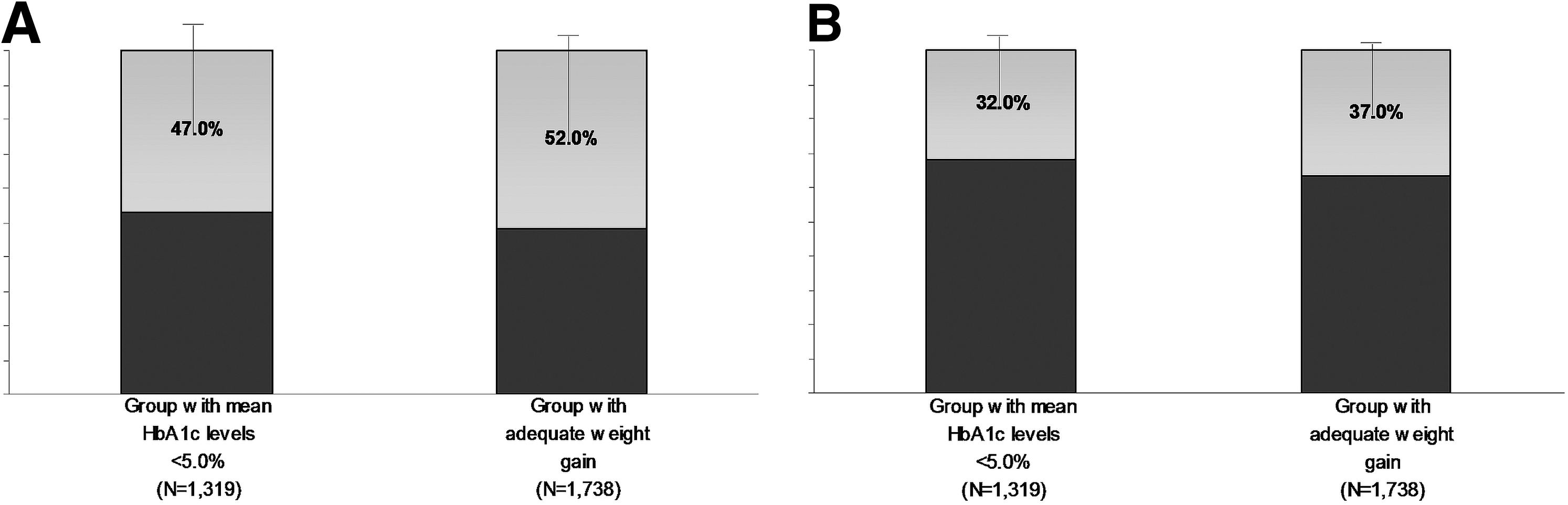
Women with an average third-trimester HbA1c ≥5.0% (n = 1319) gave birth to 7.3% versus 3.8% (p = 0.005) of large-for-gestational-age neonates and 22.0% versus 16.0% (p = 0.006) of neonates with complications. Women with excess gestational weight gain (n = 299) delivered 12.5% versus 5.2% (p < 0.001) of large-for-gestational-age neonates and 24.7% versus 19.0% (p = 0.022) of neonates with complications. In an adjusted multiple logistic regression analysis among mothers exposed to the respective risk factors, ∼47% and 52% of large-for-gestational-age neonates and 32% and 37% of neonatal complications were potentially preventable by attaining an average third-trimester HbA1c level <5.0% and optimizing gestational weight gain.
Conclusions:
Average third-trimester HbA1c level ≥5% and gestational weight gain above the IOM recommendation are relevant risk factors for neonatal complications in mothers with gestational diabetes.
Introduction
G
GDM severity at diagnosis has clearly been related to fetal overgrowth. There is also a controversial relationship between GDM severity and neonatal complications. 1 –10,15 Several approaches have evaluated the effect of glycemic control 3,7,8,15,20 on GDM neonatal complications.
Regarding weight, an at least additive effect of prepregnancy body mass index (BMI) on fetal overgrowth 2 –8,11,16,18,19 and neonatal hypoglycemia 21 has been observed. Gestational weight gain has also been related to neonatal complications. 2,4,7,13,14,16 –18
However, the definitions and measurements used have been heterogeneous. Currently, glycated hemoglobin A1c (HbA1c) testing has the advantages of preanalytic stability and assay standardization. 22 During pregnancy, interpretation of HbA1c needs to take into account that values are lowered and changes are faster because of a lowered erythrocyte life span, especially in late pregnancy. 23,24 Additionally, the updated Institute of Medicine (IOM) gestational weight gain recommendations 25 may help harmonize the definition for gestational weight gain.
For the specific group of GDM pregnancies, this study introduces the novel parameters of glycemic control and gestational weight gain to explore the effect of these factors on the risk of large-for-gestational-age birth weight and a composite of neonatal complications.
Materials and Methods
Design, setting, and subjects
An observational retrospective study was conducted. All singleton pregnant GDM women followed in a Diabetes and Pregnancy Unit in Madrid, Spain, between 1987 and 2008 (N = 2568) were included in the study. Clinical and laboratory data were prospectively entered in the Diabetes and Pregnancy Unit database. The National Diabetes Data Group (NDDG) criteria (100-g oral glucose tolerance test (OGTT): fasting glycemia, 5.8 mM; 1 h, 10.6 mM; 2 h, 9.2 mM; and 3 h, 8.1 mM) 1 were applied to diagnose GDM after universal screening in all women. The exclusion criteria were multiple pregnancies, pregestational diabetes, secondary causes of hyperglycemia (e.g., steroid treatment), pregnancies with confounding maternal morbidity factors, and incomplete data. Ethical approval to conduct this study was provided by the Hospital Ethics Committee.
All women were treated with a standard diet and received nutritional management and physical activity counseling by specialized nurses. Fasting or preprandial and 2-hour postbreakfast, lunch, and dinner capillary glucose measurements were self-obtained every other day from GDM diagnosis to delivery. Insulin treatment was started when the capillary fasting glycemia was greater than 5.3 mM and/or 6.7 mM 2 hours postprandial despite dietary treatment in at least two measurements. This treatment protocol 26 was maintained during the entire analyzed period.
Outcome and explanatory variables
Mothers with gestational diabetes were evaluated for the presence of large-for-gestational-age birth weight as a primary outcome and a composite of GDM-related neonatal complications.
GDM severity was measured by the fasting and 1- to 3-hour plasma glucose levels during a 100-g OGTT at the time of GDM diagnosis. The 100-g OGTT fasting glucose and area under the curve (AUC) were considered for baseline glucose intolerance. The trapezoidal method was applied to calculate the area. HbA1c levels were measured monthly, as a glycemic control parameter, from GDM diagnosis to delivery. High-performance liquid chromatography (Diamat and Variant autoanalyzers; Bio-Rad®, Richmond, CA) was used to obtain HbA1c values. The autoanalyzers provided exchangeable results that were calibrated to the Diabetes Control and Complications Trial normal range. Prepregnancy BMI was calculated based on self-reported prepregnancy weight and measured height. Gestational weight gain was quantified as the difference between the last weight measured before delivery and self-reported prepregnancy weight. Excess gestational weight gain was defined for prepregnancy BMI categories, as suggested by the IOM guidelines. 25
The following comparison groups of women were studied. Fasting glucose categories were defined as less than or equal to/greater than 5.8 mM at the time of GDM diagnosis (NDDG criteria). Deciles of the area under the 100-g OGTT curve and average third-trimester HbA1c levels were examined as threshold values for the primary outcome. A Fagan nomogram was used to select the threshold values that increased the odds posttest of neonatal overgrowth by at least 1.75 times. 9 Overweight (25–29.9 kg/m2) and obese (≥30 kg/m2) prepregnancy BMI categories were grouped. The upper limit of the recommended gestational weight gain range (>16 kg for normal weight, >11.5 kg for overweight, and >9 kg for obese) was defined as excess gestational weight gain.
Large-for-gestational-age birth weight was defined as infant weight >90th percentile according to sex and gestational age neonatal anthropometric standards for the Spanish population (data from the neonatal weight standards of the Spanish Society of Obstetrics and Gynecology). All GDM neonates had their glucose values monitored using a reflectance meter in heel blood. Neonatal glycemia was measured if symptoms were suspected or 2 hours after birth otherwise. Neonatal hypoglycemia was considered when glucose measurements were less than 2.2 mM. Additional tests were performed under clinical suspicion of complications following a Pediatric Unit protocol. The presence of at least one GDM-related neonatal complication (LGA birth weight, hypoglycemia, hypocalcemia, hyperbilirubinemia, polycythemia, respiratory distress, nonspecified birth trauma, and/or perinatal death) was assessed.
Statistical analyses
Associations between the studied glycemic- and weight-related parameters and neonatal outcome were assessed. Univariate associations were obtained using Student's t, Mann–Whitney U, and two-sided χ2 tests when appropriate. The threshold for statistical significance was set at p < 0.05. The parameters that did not strongly correlate (pairwise Pearson's R coefficient <0.7) and were significantly associated with the neonatal outcome were fed into a forward stepwise multiple logistic regression model along with selected covariates as plausibly related to the outcome. The effects of these factors were measured by adjusted odds ratios in 95% confidence intervals (AOR, [95% CI]). Receiver operator characteristic (ROC) curves of the combined factors that remained in the regression, with and without adjusting for covariates, were used to test the clinical usefulness of the studied parameters. The variability in the neonatal outcome that was predicted by the multivariate model was estimated by the area [95% CI] under the ROC curve.
Additional multicollinearity analyses were performed by sequentially subtracting the factors that remained in the regression model to observe variations in the area under the ROC curve. These variations would be expected from an independent influence of the factors. The attributable preventive percentage for nonexposure to a risk factor (APe% = 1 − AOR) was calculated. APe% was used to estimate the neonatal risk excess that could be preventable by nonexposure in the group of women unexposed to one risk factor. We examined the effect of the interactions among the risk factors. Statistical analyses were conducted using SPSS (SPSS, Inc., Chicago, IL) Windows version 20.0 software.
Results
Of the GDM women, eight with suspected unknown preexisting diabetes, nineteen women with renal, liver, or prothrombotic diseases, and three women with beta thalassemia were excluded. Complete data were available for 2037 (79.9%) of the eligible women. Maternal and neonatal characteristics are shown in Table 1.
Data are expressed as mean ± SD, median (interquartile range), or no. (%).
Glycated hemoglobin A1c.
Above the upper limit of the gestational weight gain recommendations (>16 kg for prepregnancy normoweight, >11.5 kg for overweight, and >9 kg for obese women) given by Institute of Medicine guidelines (2009).
Defined as a birth weight above the 90th percentile for gestational age and sex according to standards for Spanish neonates.
Including a composite of large-for-gestational-age birth weight, hypoglycemia, hypocalcemia, hyperbilirubinemia, polycythemia, respiratory distress, nonspecified birth trauma, and/or perinatal death.
100-g OGTT, 100-g oral glucose tolerance test; AUC, area under the curve; BMI, body mass index.
Gestational weight gain was more frequently above the IOM recommendations in the overweight mothers: 29.2% in the overweight and 21.2% in the obese categories compared to 7.5% in the normal prepregnancy BMI group (p < 0.001). Insulin treatment was needed for 1052 (51.7%) of the women and was more frequently prescribed for mothers of LGA neonates: 8.4% compared to 3.9% in mothers of non-LGA newborns (p < 0.001) and 23.0% of those with complicated births compared to 16.5% in mothers without neonatal complications (p < 0.001).
The best discriminatory cutoff point for LGA birth weight was an HbA1c ≥5.0% on the basis of a good sensitivity (>80%) with a balanced specificity under the ROC curve (Table 2). Higher rates for LGA birth weight and a composite of neonatal complications were present in mothers with an average third-trimester HbA1c ≥5.0% and/or in those with excess gestational weight gain (Fig. 1). Women with both conditions (n = 215) delivered 29 (13.6%) LGA and 72 (33.8%) complicated newborns compared to 57 (5.4%) and 408 (22.6%) in women with none of the risk factors (p < 0.001). The outcomes were also associated with other selected glycemic- and weight-related parameters, with the exception of a 100-g OGTT AUC threshold of 27.3 mM/min and prepregnancy overweight for both outcomes (Table 3). There were weak correlations between the predictors obtained (Pearson's R coefficients range 0.09–0.34).

Frequencies of large-for-gestational-age birth weight
Average third-trimester glycated hemoglobin A1c.
CI, confidence interval.
Statistical significance if p < 0.05.
100-g OGTT, 100-g oral glucose tolerance test at diagnosis of gestational diabetes.
Glycated hemoglobin A1c.
Prepregnancy BMI 25–29.9 kg/m2.
Prepregnancy BMI ≥30 kg/m2.
Above the upper limit of the gestational weight gain recommendations (>16 kg for prepregnancy normoweight, >11.5 kg for overweight, and >9 kg for obese women) given by Institute of Medicine guidelines (2009).
Including a composite of large-for-gestational-age birth weight, hypoglycemia, hypocalcemia, hyperbilirubinemia, polycythemia, respiratory distress, birth nonspecified trauma, and/or perinatal death.
Multivariate models revealed that an average third-trimester HbA1c ≥5.0% and excess gestational weight gain were independent predictors of LGA birth weight and a composite of neonatal complications. There was an added effect of 100-g OGTT fasting glycemia on LGA birth weight. The factor attributable preventive percentages are displayed in Table 4. The relative effect of modifiable factors is shown in Figure 2. The analyses were adjusted for maternal age and height, parity previous to index pregnancy, previous macrosomia, chronic arterial hypertension, year of GDM diagnosis, gestational age at the time of GDM diagnosis, and gestational age at birth (for large-for-gestational-age birth weight) or prematurity <37 weeks (for a composite of neonatal complications). Additional adjustment for tobacco habit was performed in the group (n = 1584) with available information. Because significantly different results were not obtained in this analysis, the definite models were used for the entire cohort (Table 4). The inclusion of insulin treatment in the multivariate models did not modify the effect of the selected glycemic- and weight-related parameters. An interaction between HbA1c and gestational weight gain was detected. There was a positive effect of this interaction on an increased rate of LGA and complicated births. The introduction of this interaction in the multivariable regression did not improve the performance of the prediction model.
Preventive percentage attributable to modifiable factors for large-for-gestational-age birth weight
Statistical significance if p < 0.05.
Odds ratio adjusted for maternal age and height, parity previous to index pregnancy, previous macrosomia, chronic arterial hypertension, year of diabetes diagnosis, gestational age at diabetes diagnosis, and gestational age at delivery (for large-for-gestational-age birth weight)/prematurity <37 weeks (for the presence of one or more neonatal complications).
Attributable preventive percentage in the exposed women.
100-g OGTT, 100-g oral glucose tolerance test at diagnosis of gestational diabetes.
Glycated hemoglobin A1c.
Above the upper limit of the gestational weight gain recommendations (>16 kg for prepregnancy normoweight, >11.5 kg for overweight, and >9 kg for obese women) given by Institute of Medicine guidelines (2009).
Including a composite of large-for-gestational-age birth weight, hypoglycemia, hypocalcemia, hyperbilirubinemia, polycythemia, respiratory distress, birth nonspecified trauma, and/or perinatal death.
The multivariate model values, not including adjustment covariates, had a 0.63 [0.58,0.69] area under the ROC curve for predicting LGA birth weight and 0.56 [0.53,0.60] for the presence of at least one neonatal complication. The model with covariates had a 0.76 [0.68,0.79] area under the ROC curve for LGA birth weight and 0.65 [0.62,0.68] for the presence of at least one neonatal complication.
Discussion
Average third-trimester HbA1c level ≥5% and gestational weight gain above the IOM guidelines are modifiable factors that influence neonatal overgrowth and neonatal complications in mothers with GDM.
When balancing the effects of maternal glucose and weight, previous research was focused on gestational diabetes severity and prepregnancy BMI. Severe GDM and prepregnancy obesity are related to large-for-gestational-age birth weight and a composite of neonatal complications. 2 –6,12,16,27,28 To our knowledge, this study is the first to evaluate both the effect of average third-trimester HbA1c level and weight gain above the IOM guidelines on GDM pregnancies and neonatal outcome.
Our approach was applied to GDM mothers. As a consequence, the calculation of the attributable preventive percentages of the parameters was not influenced by the factor prevalence in the general population. In general population-based studies, 2,5,6 the high impact of obesity on neonatal complications could be explained by a high prevalence of obesity.
A positive result is that around one third of the complicated births may be prevented by achieving average HbA1c level <5.0% after GDM diagnosis. However, the value of HbA1c testing every 4–5 weeks, as a glycemic control parameter during GDM pregnancies, has not previously been demonstrated 23,24,29 –31 HbA1c values reflect the average glycemia during the previous 2–4 weeks of gestation. 23 Thus, one HbA1c measurement at GDM diagnosis 23,30 does not reflect changes in glycemic control after treatment. There is a lack of HbA1c threshold values that indicate neonatal risk. HbA1c values are lower, 24 and HbA1c changes are faster in pregnant compared to nonpregnant women. The reason for these rapid changes is the gestational expansion of red cell mass. 23,24
There is a renewed debate on the effect of maternal gestational weight gain on neonatal outcome. The IOM provided revised gestational weight gain recommendations for the general population in 2009. 25 Concerning GDM pregnancies, recent studies found an effect of gestational weight gain, independent of prepregnancy BMI, on fetal overgrowth, although the impact of GDM severity and control was not assessed. 13,14,18 Taking these variables together, we estimated that 52.0% of large neonates and 37.0% of complicated births would be avoided by compliance with weight gain recommendations. Dietary GDM treatment itself may help attain this nonglycemic goal. 32 However, physicians frequently omit gestational weight gain counseling during pregnancy 33 in GDM. This aspect is important, in particular, in overweight and obese women. In these women, excess weight gain is associated with higher risks of hypertension, cesarean section, neonatal overgrowth, weight retention, and persistent abnormal glucose tolerance after delivery. 14,17 Excess gestational weight gain was more prevalent among overweight/obese women in this study.
One limitation of this study was its retrospective nature, although data were prospectively collected. Another limitation was the prepregnancy BMI assessment based on self-reported weight. In this sense, a previous validation study documented that 84% of reproductive-aged women were classified into real BMI categories based on self-reported weight and height. 34 One strength of this analysis was that a large number of studied GDM pregnancies were similarly treated at a single Diabetes and Pregnancy Unit. In our opinion, these results are relevant in a specific GDM population. The measurements being used warrant external validation and may be the basis of further intervention studies tailored to GDM women.
Considering the GDM infants' well-being, minimizing neonatal overgrowth could also have long-lasting benefits. Growing evidence support a risk of obesity and metabolic syndrome during childhood. Therefore, LGA birth weight probably reflects a cardiometabolic profile that affects one's entire life. 10,35
Conclusion
GDM treatment targets based on an average HbA1c level <5.0% and gestational weight gain adequacy to IOM are suggested in these results. This addition of a glucose- and weight-centered strategy seems promising for reducing neonatal risk in mothers with GDM.
Footnotes
Acknowledgments
The authors greatly appreciate the dedication and expertise of the nurses and technical assistants in the Diabetes and Pregnancy Unit. We also acknowledge the professional counseling received regarding statistical procedures.
Author Disclosure Statement
No competing financial interests exist.