
Abstract
Background:
The goal of prenatal care is to maximize health outcomes for a woman and her fetus. We examined how prenatal care is associated with meeting the 2009 Institute of Medicine (IOM) guidelines for gestational weight gain.
Sample:
The study used deidentified birth certificate data supplied by the North Carolina State Center for Health Statistics. The sample included 197,354 women (≥18 years) who delivered singleton full-term infants in 2011 and 2012.
Methods:
A generalized multinomial model was used to identify how adequate prenatal care was associated with the odds of gaining excessive or insufficient weight during pregnancy according to the 2009 IOM guidelines. The model adjusted for prepregnancy body size, sociodemographic factors, and birth weight.
Results:
A total of 197,354 women (≥18 years) delivered singleton full-term infants. The odds ratio (OR) for excessive weight gain was 2.44 (95% CI 2.37–2.50) in overweight and 2.33 (95% CI 2.27–2.40) in obese women compared with normal weight women. The OR for insufficient weight gain was 1.15 (95% CI 1.09–1.22) for underweight and 1.34 (95% CI 1.30–1.39) for obese women compared with normal weight women. Prenatal care at the inadequate or intermediate levels was associated with insufficient weight gain (OR: 1.32, 95% CI 1.27–1.38; OR: 1.15, 95% CI 1.09–1.21, respectively) compared with adequate prenatal care. Women with inadequate care were less likely to gain excessive weight (OR: 0.88, 95% CI 0.86–0.91).
Conclusions:
Whereas prenatal care was effective for preventing insufficient weight gain regardless of prepregnancy body size, educational background, and racial/ethnic group, there were no indications that adequate prenatal care was associated with reduced risk for excessive gestational weight gain. Further research is needed to improve prenatal care programs for preventing excess weight gain.
Introduction
I
Prenatal care can help prevent potential health problems during the course of pregnancy through screening and the recommendation of healthy lifestyle changes. 5 The American Academy of Pediatrics (AAP) and American Congress of Obstetricians and Gynecologists (ACOG) describe a prenatal care program as “a coordinated approach to medical care and psychosocial support … throughout the antepartum period” to promote the health of mothers and babies. 5 Pregnant women are encouraged to start prenatal care before 12 weeks of gestation and visit their designated prenatal care provider 9–11 times throughout pregnancy to regularly monitor weight, blood pressure, kidney function, blood sugar levels, and fetal growth. 5
The state of North Carolina birth certificate collects information on the infant as well as maternal demographic characteristics and risk factors. In 2010, at the behest of the National Center for Health Statistics, North Carolina revised its birth certificate to collect, among other new information, maternal height, prepregnancy weight, and weight at delivery. 6 These changes allow for the assessment of maternal weight gain relative to the IOM guidelines for her prepregnancy BMI. A deidentified file with 2011–2012 birth data was supplied by the State Center for Health Statistics (SCHS) through the Howard W. Odum Institute for Research in Social Science at UNC-Chapel Hill. Using these data, we examined factors associated with excessive or insufficient weight gain relative to the IOM guidelines.
Sample and Methods
The 2011–2012 North Carolina birth certificate data for full-term singleton births were analyzed. Potential predictors of weight gain derived from information collected on the birth certificate included maternal demographic information (age, race/ethnicity, education, and marital status) as well as Medicaid status (i.e., whether Medicaid is expected to cover the costs of the delivery) and the birth weight of the infant. Birth weight was categorized according to 500-g increments and further divided into three categories: Very low/low (≤2500 g), Normal (2501–4000), and High (>4000). 7 The quality of prenatal care was measured with the Kotelchuck index of adequacy of prenatal care. 8 This index measures the utilization of prenatal care in two dimensions. The first dimension, adequacy of initiation of prenatal care, measures initiation by using the month prenatal care began, which is reported on the birth certificate. The second dimension, adequacy of received services, is measured by determining the ratio of the actual number of visits, which is reported on the birth certificate, to the expected number of visits. The expected number of visits is based on the ACOG prenatal care visitation standards for uncomplicated pregnancies. 9 The expected number of visits is adjusted for gestational age at the initiation of care and for gestational age at delivery. The two dimensions are combined into a single summary index. The index is grouped into four categories: adequate plus (prenatal care begun by the fourth month of pregnancy and 110% of recommended visits received); adequate (prenatal care begun by the fourth month of pregnancy and 80%–109% of recommended visits received); intermediate (prenatal care begun by the fourth month of pregnancy and 50%–79% of recommended visits received); and inadequate (prenatal care begun after the fourth month of pregnancy or less than 50% of recommended visits received). 8
Our outcome was adequacy of weight gain as defined by the IOM guidelines in 2009. 1 Weight gain was computed by subtracting prepregnancy weight (self-reported on birth certificate) from weight at delivery. The IOM guidelines 1 define weight gain adequacy according to prepregnancy BMI, which was computed from prepregnancy weight and height. Women with a prepregnancy BMI of less than 18.5 (underweight) are advised to gain 28–40 lbs.; women with a prepregnancy BMI of 18.5–24.9 (normal weight) are advised to gain 25–35 lbs.; women with a prepregnancy BMI of 25.0–29.9 (overweight) are advised to gain 15–25 lbs.; and women with a prepregnancy BMI of greater than 30.0 (obese) are advised to gain 11–20 lbs. 1 Each mother's weight gain adequacy was categorized as insufficient, adequate, or excessive based on the guidelines for her prepregnancy BMI.
For this study, we included full-term (≥37 weeks) singleton births to mothers who were at least 18 years of age. Younger mothers were excluded because the IOM weight gain guidelines rely on the WHO BMI categories, which were designed for adults 18 years and older. 1
Analytic approach
Unadjusted relationships between the adequacy of weight gain (insufficient, adequate, or excessive) and potentially associated variables were examined using chi-square tests. Additionally, a multinomial logistic regression model was used to predict weight gain adequacy as a function of the available variables (Medicaid status, race/ethnicity, age, education, marital status, and adequacy of prenatal care) with the goal of identifying factors for predicting excessive/insufficient weight gain in an adjusted model. Additionally, to investigate whether the effect of prenatal care adequacy varied according to prepregnancy weight status, we developed an expanded model to include the interaction between adequacy and prepregnancy weight status. Because birth weight of the infant can be both a contributor to and an effect of pregnancy weight gain, birth weight was not included in the models. However, a model controlling for birth weight was included as a sensitivity analysis. Adequate weight gain was used as the reference group for the multinomial logistic model, and we report the odds ratios for excessive versus adequate weight gain and insufficient versus adequate weight gain. All analyses were conducted in SAS v9.3, and statistical significance was calculated for p < 0.05.
Results
After excluding 5186 births to mothers younger than 18 years of age, the registry included 203,092 singleton full-term births to mothers who were North Carolina residents during 2011 and 2012. An additional 12,009 cases (5.9%) were excluded due to missing data. Missing data were found in the mother's age (N = 11, <0.01%), prepregnancy BMI (N = 6167, 3.0%), weight gain (N = 7493; 3.7%), infant's birth weight (N = 79; 0.04%), Kotelchuck index (N = 3771; 1.9%), Medicaid status (N = 1319; 0.65%), marital status (N = 270; 0.13%), educational attainment (N = 777; 0.38%), and race/ethnicity (N = 103; 0.05%). After excluding cases with missing data, a total of 191,083 cases were studied. In this sample, 49.8% of the mothers were either overweight or obese, and 15.4% received inadequate prenatal care. See Table 1 for other characteristics.
Insufficient GWG, insufficient gestational weight gain (<28 lb. for underweight, <25 lb. for normal weight, <15 lb. for overweight, and <11 lb. for obese women prepregnancy).
Adequate GWG, adequate gestational weight gain (28–40 lb. for underweight, 25–35 lb. for normal weight, 15–25 lb. for overweight, and 11–20 lb. for obese women prepregnancy).
Excessive GWG, excessive gestational weight gain (>40 lb. for underweight, >35 lb. for normal weight, >25 lb. for overweight, and >20 lb. for obese women prepregnancy).
p < 0.0001 for a chi-square test of association with weight gain sufficiency.
Medicaid was expected to cover the costs of the delivery at the time of delivery when the family incomes were lower than 185% of the federal poverty threshold.
BMI, body–mass index; Prenatal care adequacy by Kotelchuck index of adequacy of prenatal care.
Bivariate analysis of variables by gestational weight gain adequacy
Overall, almost half of the mothers (49.6%, N = 94,728) exceeded the IOM recommendations, 30.5% (N = 58,273) met the recommendations, and 20.0% (N = 38,082) gained insufficient weight. The level of prenatal care access was adequate or adequate plus for 76.5% of the women, and 15.4% of the women received inadequate prenatal care. Table 1 summarizes the bivariate relationships between weight gain adequacy and other study variables, all of which were statistically significant (p < 0.0001 for all).
Prepregnancy BMI
Excessive weight gain was most prevalent in mothers who were overweight (63.3%) or obese (56.8%) before pregnancy (p ≤ 0.0001). Insufficient weight gain was most prevalent in mothers whose prepregnancy BMI was underweight (32.3%) (p ≤ 0.0001).
Demographic variables
Having Medicaid as the expected payment source for delivery was associated with insufficient weight gain. Excessive weight gain was highest (above 50%) in non-Hispanic white and non-Hispanic black women (p ≤ 0.0001). Older age (35+) was associated with a slight decrease in the risk of excessive weight gain (p ≤ 0.0001). Women with less than a high school education were most likely to have insufficient weight gain (p ≤ 0.0001), and women with education beyond high school were most likely to have excessive weight gain (p ≤ 0.0001). Unmarried women were somewhat more likely to have insufficient weight gain (p ≤ 0.0001).
Prenatal care and birth weight
Of the mothers who received adequate or adequate plus prenatal care (i.e., 76.5% of the women), half of the women gained excess weight (51%). The rate of excess weight gain was lower in mothers who received intermediate (49%) or inadequate (44%) prenatal care (p ≤ 0.0001). About a quarter of the women who received an inadequate level of prenatal care reported insufficient weight gain, higher than other prenatal care adequacy categories (p ≤ 0.0001). Excessive weight gain tended to be associated with high birth weight, and insufficient gain was associated with low birth weight (p ≤ 0.0001).
Multivariable analysis of adequacy of gestational weight gain
In multivariable analysis, all variables in the model were significantly associated with the adequacy of weight gain (p < 0.0001 for all). Table 2 presents the adjusted odds ratios and confidence intervals.
Compared with adequate GWG.
p < 0.001.
Kotelchuck index of adequacy of prenatal care.
p < 0.05.
GWG, gestational weight gain; IOM, Institute of Medicine; aOR, adjusted odds ratio; CI, confidence interval; BMI, body–mass index; Prenatal care adequacy by Kotelchuck index of adequacy of prenatal care.
Factors associated with insufficient weight gain
The model indicated that being underweight prepregnancy was a risk factor for insufficient gestational weight gain. Compared with having a normal weight prepregnancy, being underweight increased the odds of failing to gain adequate weight by 15%. Being obese prepregnancy increased the odds by 34%.
Less than adequate prenatal care was associated with insufficient weight gain. Prenatal care at the inadequate and intermediate levels increased the odds of insufficient weight gain by 32% and 15%, respectively.
Other risk factors for failing to gain adequate weight included older age (35+), lower educational attainment (less than high school graduation), unmarried status, expected payment for delivery from Medicaid, and race/ethnicity other than non-Hispanic white (Table 2).
Factors associated with excessive weight gain
Compared with a normal weight prepregnancy, being overweight increased the risk for excessive weight gain by 144%, and being obese increased the risk by 133%. In other words, overweight and obese pregnant women were more than twice as likely as women with a normal weight to gain excessive weight during pregnancy. Intermediate prenatal care was similar to adequate prenatal care with respect to the risk for excessive weight gain. Inadequate prenatal care, however, was associated with a 12% lower risk of excessive weight gain, and adequate plus care was associated with a 3% lower risk of excessive weight gain. Additional risk factors for excessive gestational weight gain included young maternal age (the risk appears to decrease as age increases) and unmarried status. Excessive weight gain risk also appears to increase with increasing education. Additional risk factors for insufficient and excessive weight gain, after controlling for other model variables, are summarized in Table 2.
Interaction between adequacy of prenatal care and prepregnancy BMI
Given the strong relationships of both BMI and the Kotelchuck index with weight gain adequacy, we fit a model, including the interaction between these variables, to explore whether the effect of prenatal care differed according to prepregnancy weight status. The interaction was statistically significant (p < 0.0001), and the resulting odds ratios are presented in Table 3 and Figure 1.
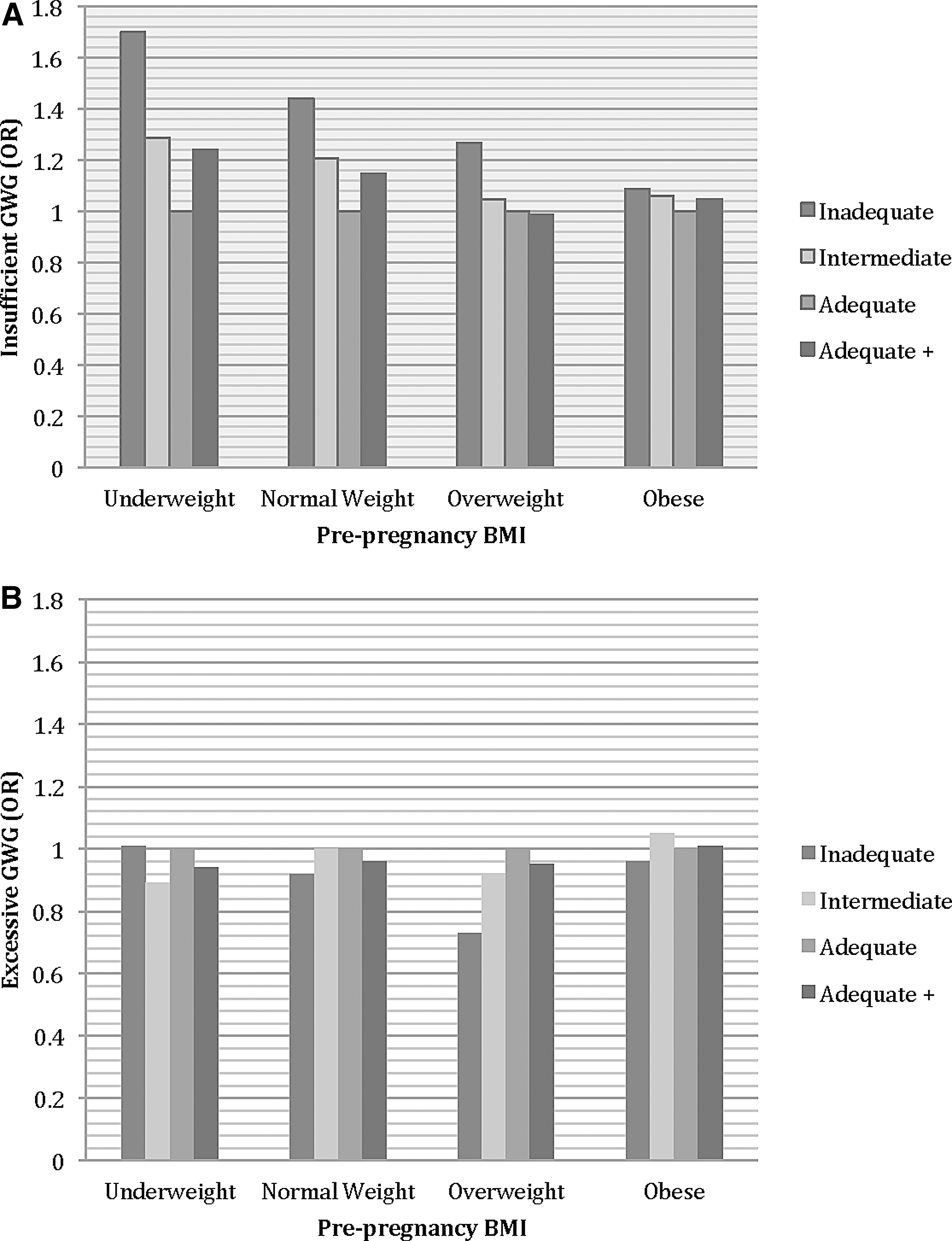
An interaction between prepregnancy BMI category and adequacy of prenatal care allows for interpretation of the effect of prenatal care within each category of prepregnancy BMI.
Kotelchuck index of adequacy of prenatal care.
Compared with adequate GWG.
p < 0.001.
p < 0.05.
Across all weight statuses, the odds of insufficient weight gain were highest in mothers who received inadequate prenatal care. The size of the effect decreases as prepregnancy weight status increases. Both underweight and normal weight women who had intermediate or adequate plus prenatal care had an increased risk of insufficient weight gain compared with mothers who received adequate care. No effects of intermediate or adequate plus care on the odds of insufficient weight gain were seen in overweight or obese women.
There was no relationship between prenatal care adequacy and the odds of excessive versus adequate weight gain for women who were underweight or obese prepregnancy. Among women who were normal weight or overweight prepregnancy, both inadequate care and adequate plus prenatal care were associated with lower odds of excessive weight gain.
A sensitivity analysis was conducted to assess the effect of birth weight in the model, and the model was expanded to control for birth weight of the infant. Similar to the unadjusted analysis, birth weight was strongly associated with weight gain. High birth weight was associated with increased odds of excessive weight gain, and very low/low birth weight was associated with increased odds of insufficient weight gain. The remaining estimates in the model were largely the same. However, there was some loss of significance in the odds ratios for the Kotelchuck index and race/ethnicity in Table 2: the intermediate level of prenatal care adequacy was associated with no higher odds of insufficient weight gain than adequate prenatal care. Mothers who were Hispanic, non-Hispanic black, or of other race/ethnicity no longer had higher odds of insufficient weight gain compared with non-Hispanic white women. Follow-up analyses indicate that this change is not surprising as both prenatal care adequacy and race/ethnicity are significantly associated with birth weight in these data.
Discussion
In 2009, IOM issued a revised set of guidelines for weight gain in pregnancy, which reflected changes in the childbearing population since the guidelines were issued in 1990. Since 1990, the rates of overweight and obesity prepregnancy have risen. 1 The revised guidelines are intended to help healthcare providers assist pregnant women, particularly women who are overweight and obese, in avoiding excess weight gain. We analyzed a large data set from a group of adult pregnant women who had a full-term singleton pregnancy. Our study confirmed that being overweight or obese prepregnancy is a risk for excessive weight gain during pregnancy. We also found that being underweight prepregnancy, particularly when the underweight status was combined with inadequate prenatal care, was significantly associated with insufficient weight gain. These outcomes support the importance of promoting women to gain the recommended amount of weight during pregnancy.
When women who were overweight or obese became pregnant, their risk for excessive weight gain was twice as high as women with normal weight. Unfortunately, we also found that adequate or adequate plus (vs. intermediate or inadequate) prenatal care was not associated with a lower risk of excessive gestational weight gain. The most intensive adequate plus care appeared to offer a small benefit, lowering the odds of excessive weight gain relative to adequate care in women who were normal weight or overweight prepregnancy.
ACOG recommends early and frequent prenatal care visits, 9 including an initial visit at 8–10 weeks, monthly visits up to 28 weeks, biweekly visits up to 36 weeks, and weekly visits through delivery. National Guideline Clearinghouse (NGC) and the Institute for Clinical Systems Improvement (ICSI) 2010 recommendations and the U.S. Department of Health and Human Services (USDHHS) Expert Panel on the Content of Prenatal Care also provide similar guidelines. 5 The results of our study suggest that frequent and timely prenatal care access was not associated with better outcomes related to excessive weight gain. Given that existing guidelines recommend nutrition and exercise counseling only at the initial visit (8–10 weeks), additional emphasis on lifestyle counseling and interventions focused on healthy eating and increases in physical activity may improve the effectiveness of prenatal care in preventing excessive weight gain.
The results of our study suggest that the current prenatal care program set forth by ACOG, NGC, ICSI, and USDHHS needs to be reexamined to improve the program effectiveness for reducing the risk of excessive gestational weight gain. Limited evidence suggests that the incorporation of a brief nutritional assessment by a specialist (e.g., a nutritionist), followed by behavior counseling during a regular prenatal care visit, 10 or a small group session during a prenatal care visit 11 may potentially reduce total weight gain. For some women, providing educational material could be effective. 11 The need for the incorporation of effective weight management counseling or intervention in prenatal care programs is pre-eminent.
ACOG recommends that pregnant women engage in 30 minutes or more of moderate exercise a day. 12 Implementing lifestyle changes and maintaining those changes require behavioral intervention protocols, including setting realistic goals and monitoring/follow-up. Prior studies suggest that clinic-based lifestyle interventions can be effective in achieving recommended weight gain. 11,13
The tenuous relationship between adequacy of prenatal care and maternal weight gain may indicate that current prenatal care recommendations are not sufficient to promote healthy weight gain. Some women, at the time of the first prenatal visit, may already be on a trajectory toward excessive weight gain and are expected to continue to gain weight. For these women, education about healthy weight before and during the first weeks of pregnancy is also important. Although the Kotelchuck index is a well-accepted index for accessing prenatal care, it was developed to detect the risk of low birth weight, not to promote healthy maternal weight gain. Investigation of prenatal care practices that are predictive of healthy maternal weight gain and development of an index to that end would be a logical next step.
Our study found that ethnic/racial minorities had increased risk of insufficient weight gain. This is somewhat counterintuitive as the prevalence of obesity is higher among racial/ethnic minority women in our study as well as existing reports, 14 and being obese increases the risk for excessive gestational weight gain. This finding, however, is consistent with an existing study, which found that African Americans and Hispanics were less likely than Caucasian women to exceed the IOM guidelines. 2 Their study did not, however, examine risk factors for insufficient weight gain. There may be a subpopulation of women who have trouble gaining weight during pregnancy due to food insecurity or competing life demands. Further research into the risk factors in the small population gaining insufficient weight is warranted.
One of the major strengths of our study is the use of a population-level database. There are, however, several limitations to this database. Prepregnancy weight is self-reported by mothers. Clinical measurements of height and weight are considered the gold standard and might supply more accurate data on prepregnancy BMI, particularly for demographic groups with poor recall. However, self-reported weight and height have been determined to be a reasonable proxy. 15 Another limitation was the report of prenatal care history at the time of delivery, which may be subject to recall/reporting error. Finally, the birth certificate does not capture information on other factors such as dietary counseling or feedback on self-monitoring of physical activity and diet that may influence the relationship between prenatal care and weight gain in pregnancy.
Conclusions
Since IOM has revised the guidelines for weight gain in 2009, there has been little report on gestational weight gain. In our study, only 30% of women achieved the recommended weight gain. Furthermore, almost 80% of the women who received an adequate level of prenatal care had excessive weight gain. Clearly, the prenatal care program needs to be examined to develop a structure that will foster healthy weight gain during pregnancy for pregnant women with diverse backgrounds in North Carolina and the United States.
Footnotes
Acknowledgment
The authors appreciate Najmul Chowdhury, MB, BS, MPH, for assisting in accessing data.
Author Disclosure Statement
No competing financial interests exist.