
Abstract
Objective:
Compared to heterosexuals, sexual minority women (SMW) have higher rates of the metabolic syndrome risk factors (e.g., obesity, smoking, heavy drinking, and depression). Yet, no published research has examined whether SMW have higher rates of the metabolic syndrome. The aim of this study is to describe the prevalence of the metabolic syndrome and its individual factors in a sample of heterosexuals and SMW, and identify whether SMW are at greater risk of having the metabolic syndrome.
Materials and Methods:
Data are from the Epidemiologic STudy of HEalth Risk in Women (ESTHER), a cross-sectional convenience sample of 479 SMW and 400 heterosexual women from Pittsburgh, Pennsylvania. Participants provided self-report questionnaire data, clinical data, and blood work.
Results:
Compared to heterosexuals, SMW had higher mean waist circumference, fasting glucose, and systolic and diastolic blood pressure. Nearly one-quarter (24.3%) of SMW had the metabolic syndrome compared to 15.6% of heterosexual women (p = 0.002). After controlling for demographic and risk factors, SMW had a 44% higher risk of having the metabolic syndrome than heterosexuals (p = 0.031).
Conclusions:
To our knowledge, this is the first study to identify this health disparity in SMW. Future studies should explore differential risk of mortality and metabolic health between SMW and heterosexuals.
Introduction
B
The distribution of the metabolic syndrome across the population is not uniform. Population-based samples investigating the metabolic syndrome have found that prevalence is higher among certain racial/ethnic groups, such as Mexican Americans 2,5 or Hispanics in general, 6 and other research shows that the metabolic syndrome is more prevalent among women compared to men within certain racial/ethnic groups. 1 Rates of the metabolic syndrome among women increase over age 50, providing evidence that hormonal protection against developing the metabolic syndrome is reduced once women reach menopause. 5,7
Several psychosocial and behavioral risk factors for the metabolic syndrome have been identified. A meta-analysis found that current smoking was associated with a 26% higher risk of the metabolic syndrome. 8 Depression is also strongly associated with the metabolic syndrome. 9,10 While light or low-risk drinking seems to be protective against the metabolic syndrome, 11 heavy drinking is a significant risk for having the metabolic syndrome. 12,13
Compared to heterosexual women, sexual minority women (SMW) have demonstrated higher rates of obesity, 14 smoking, 15 heavy drinking, 16 and depression. 17 Yet, no published research has examined whether SMW have higher rates of the metabolic syndrome. The aim of this study is to describe the prevalence of the metabolic syndrome and its individual factors in a sample of heterosexual and SMW, and identify whether SMW are at greater risk of having the metabolic syndrome.
Materials and Methods
Data for the study are from the Epidemiologic STudy of HEalth Risk in Women (ESTHER), a cross-sectional cardiovascular risk study of a convenience sample of women recruited from Pittsburgh, Pennsylvania, and surrounding areas from 2003 to 2006. Participants were recruited through newspaper and radio advertisements, community health events, LGBT events, and the University of Pittsburgh broadcast phone-message system. A total of 1084 women were initially recruited; approximately half were SMW. Due to challenges related to recruiting African American women in a city that is not racially diverse and issues of outlier data, the original study team selected a random sample of black heterosexuals to be approximately equivalent to the number of black SMW and excluded women older than 65 years of age. The final sample available for analysis consisted of 479 SMW and 400 heterosexual women.
During a first clinic visit, participants' weight, height, and blood pressure were measured and they provided a blood sample to measure data, including fasting glucose, cholesterol, and triglycerides. At this visit, they also completed a battery of written questionnaires that assessed a number of psychosocial and demographic variables, a physical activity interview, and a 2-week medicine history. At a second visit, participants reviewed a 3-day diet and exercise diary and underwent a Dual Energy X-ray Absorptiometry (DEXA) scan of the hip, spine, and whole body. Participants were offered a $50 incentive for their time. The research was approved by the University of Pittsburgh Institutional Review Board (approval No. 0404147).
Measures
Sexual orientation
Women were classified as sexual minority if they (1) identified as anything other than heterosexual and (2) reported either being only or primarily emotionally, physically, and romantically attracted to women in the past 5 years or having only or primarily female sexual partners in the past 5 years. Heterosexual women were those who identified as “heterosexual/straight” and reported only male sexual partners since the age of 18. Women who reported attraction to men and women and/or male and female sexual partners in the past 5 years were excluded. Sexual orientation was a dichotomous variable.
Metabolic syndrome
The presence of the metabolic syndrome was assessed using the 2004 revised National Cholesterol Education Program's (rNCEP) definition. 4,18 To meet the criteria for the metabolic syndrome, participants had to meet at least three of the following criteria for females: fasting glucose of 100 mg/dL, or above or receiving treatment for diabetes; triglycerides of 150 mg/dL or above, or currently receiving treatment for high triglycerides; blood pressure of ≥130/85 mmHg, or currently receiving treatment for high blood pressure; waist circumference of 88 cm or greater; and HDL-C <50 mg/dL, or currently receiving treatment for high cholesterol.
Race
Participants reported their race as black, Native American, Asian or Pacific Islander, white, or other. After removing Native American, Asian or Pacific Islander, or other respondents due to small numbers (n = 32), race was recoded into a dichotomous variable.
Age
Age categories were calculated using participants' dates of birth and were entered as dummy variables.
Education
Education was assessed using a 5-point scale and collapsed to a dichotomous variable.
Relationship status
Because marriage was not legal for sexual minority participants at the time, relationship status was instead self-reported as in a committed relationship, not in a committed relationship, or other. Responses of other were collapsed into the “not in a committed relationship” category to create a dichotomous variable.
Menopausal
Menopause was defined as not having a period within the past 12 months. 19
Current smoking
Respondents who answered “yes” to “Do you currently smoke cigarettes” were coded as current smokers.
Hazardous drinking
Hazardous drinking was assessed with four types of questions that assessed drinking behaviors over the past 12 months. Participants were asked about the following: heavy episodic drinking (“During the last 12 months, how often did you have six or more drinks of wine, beer, or liquor in a single day?”); intoxication (“About how often in the last 12 months did you drink enough to feel drunk”); consequences of drinking (driving drunk, accident in the home, harmful effect on housework, partner/spouse, friends or relatives complained about drinking, hurt chances of getting a job or promotion, people annoyed you by criticizing your drinking, guilt about drinking, and not remembering things done/said while drinking); and possible alcohol dependence (drinking fast for quicker effect, morning drinking, inability to stop drinking before intoxication, inability to quit or cut down drinking, and surreptitious drinking). Responses were summed and dichotomized for each of the four types of questions (0 = no behaviors, 1 = any behaviors) to create an index of 0–4. Hazardous drinking was dichotomized using a cutoff of 2 or more on the index. 20
Depression
Depression was assessed using the CES-D 10 scale (Cronbach's alpha = 0.86). 21 The scale has the same reliability for lesbian and bisexual women compared to heterosexuals. 22 Depression was a dichotomous variable where any participant who scored over 10 was coded as reporting depressive symptoms.
Body–mass index status
Height and weight were measured by a standardized research protocol at the first clinic visit. Body–mass index (BMI) was categorized using the following formula: weight (lb)/(height [in])2 × 703. 23 Using the National Heart, Lung, and Blood Institute (NHLBI) standards, we categorized BMI as <18.5 = underweight, 18.5–24.9 = normal weight, 25–29.9 = overweight, and >30 = obese 24 and created dummy variables. Due to the small number of underweight individuals (n = 6), they were collapsed into the normal weight category.
Analysis
The analysis was limited to women who had complete data on all the components of the metabolic syndrome. Data were analyzed using SPSS version 21.0. We ran descriptive statistics to assess the entire sample and conducted chi-square tests (for categorical variables) and independent sample t-tests (for continuous variables) to examine differences between heterosexuals and SMW. We attempted to obtain RRs using generalized linear models with a binomial distribution with a log link, but the model failed to converge. Therefore, we obtained RRs using Cox regression with a time constant. 25,26
Results
After removing the four participants who did not have complete data to allow us to identify the metabolic syndrome, the final analytic sample was 875 women (397 heterosexuals and 478 sexual minorities). Sample characteristics are shown in Table 1. In terms of demographic and psychosocial variables, heterosexuals and SMW were largely similar, except that SMW were significantly more likely to be in a committed relationship, depressed, and current smokers. Heterosexuals and SMW were not significantly different on mean triglyceride levels or HDL-C, but SMW had higher mean waist circumference, fasting glucose, and systolic and diastolic blood pressure. Figure 1 shows the number of risk factors for the metabolic syndrome for heterosexuals and SMW. On average, SMW had more risk factors for the metabolic syndrome compared to heterosexuals (1.46 vs. 1.16, respectively, p < 0.001). The overall prevalence of the metabolic syndrome in the sample was 20.3%, although nearly one-quarter (24.3%) of SMW had the metabolic syndrome compared to 15.6% of heterosexual women (chi-square = 10.015, p = 0.002).
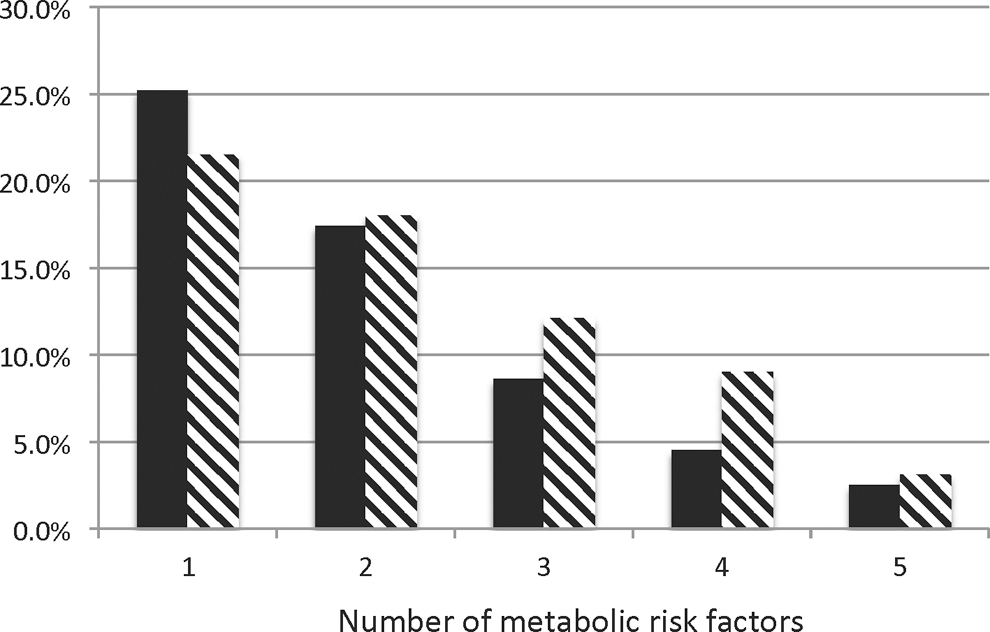
Distribution of metabolic risk factors among heterosexual women (solid) and sexual minority women (hatched).
BMI, body–mass index; BP, blood pressure; HDL-C, high-density lipoprotein cholesterol; SD, standard deviation; WC, waist circumference.
The unadjusted RR for the metabolic syndrome among SMW compared to heterosexual women was 1.55 (95% confidence interval [95% CI] 1.14–2.12, p = 0.005) (Table 2). After controlling for race, age, education, relationship status, menopause, current smoking, hazardous drinking, depression, and BMI status, the RR for SMW decreased slightly to 1.44 but remained significantly higher compared to heterosexual women (95% CI 1.03–1.99, p = 0.031). In the adjusted model, overweight (RR = 3.88, p = <0.001) and obesity (RR = 8.85, p < 0.001) also carried a higher risk for the metabolic syndrome. Conversely, higher education was associated with a reduced risk (RR = 0.69, p = 0.018).
95% CI, 95% confidence interval; RR, risk ratio.
Discussion
In this sample of women, SMW had a 44% greater risk of having the metabolic syndrome compared to their heterosexual counterparts. To our knowledge, this is the first study to identify this health disparity among SMW. The greater risk of the metabolic syndrome was evident even after controlling for several risk factors that are associated with the metabolic syndrome, including overweight and obesity, one of the most significant health disparities between SMW and heterosexuals. 27,28 The higher risk of the metabolic syndrome for SMW in this sample seems to be driven by the fact that, compared to heterosexual women, SMW had higher mean waist circumference, fasting glucose levels, and blood pressure.
Given the metabolic syndrome's association with CVD or all-cause mortality, this study's findings suggest that SMW are at higher risk of mortality compared to heterosexual women. Research is limited, but two studies have found evidence that SMW have a higher prevalence of CVD risk factors compared to heterosexual women. 29,30
The concept of metabolic health is an avenue of research that would be useful to explore in the context of sexual orientation. Research suggests that metabolic health (e.g., the absence or presence of metabolic risk factors) is more predictive of CVD and all-cause mortality than obesity. 31 Thus, future studies should examine whether there is a disparity in prevalence of metabolic health among SMW compared to heterosexual women.
In addition, research should examine a link between experiences of stigma and/or discrimination and the metabolic syndrome among SMW. The allostatic load hypothesis suggests that repeated exposure to stressors disrupts the hypothalamus–pituitary–adrenal axis, which is responsible for modulating cortisol levels in response to stress to maintain allostatis. 32 Given the evidence in the extant literature of the relationship between discrimination and cortisol, 33 and the relationship between cortisol, abdominal adiposity, and the metabolic syndrome, 34,35 we might hypothesize that excess prevalence of the metabolic syndrome and/or mortality in sexual minority populations is due to biological responses to social stressors. Data from the prospective Whitehall II study in England show an association between prevalence of the metabolic syndrome and both socioeconomic status (SES) and chronic work stress, providing further evidence for this hypothesis. Indeed, one study reported a link between community-level LGBT stigma and higher all-cause mortality rates among sexual minorities. 36
Given that these results are from a convenience sample obtained from a limited geographical area, results cannot be generalized and there are several limitations to our findings. The convenience sampling strategy likely missed subpopulations of sexual minorities who were unaware of the existence of the study because they were not connected to the community groups through which the study was advertised or who were unwilling to participate in this research. This sample of women was highly educated (65.1% had a college degree or higher), which could be due, in part, to the recruitment methodology and/or the possibility that SMW of higher education status were more willing to participate. 37 We note that, however, the prevalence of the metabolic syndrome is inversely correlated with SES. 38,39 Future studies should examine whether the risk of the metabolic syndrome among SMW is different by educational level.
The racial makeup of Pittsburgh at the time of this study, in particular, the small number of black SMW, and the resulting decisions that led to the small number of black SMW in the sample limit our ability to explore the nuances associated with the metabolic syndrome and race 40 among heterosexuals and SMW. Continuing this line of inquiry with more racially diverse samples is a critical future task.
The fact that this study did not find higher rates of depression, binge eating, or hazardous drinking among SMW compared to heterosexuals, which is inconsistent with the broader literature, 17,41,42 could be an artifact of the methods by which the sample was obtained. We do note that the hazardous drinking measure used in our study is based on the work of Hughes et al. in the Chicago Health and Life Experiences of Women study, which is a longitudinal sample of lesbian women. 20 This measure is a stricter definition of heavy episodic drinking than is typically used for women, 43,44 and the use of another measure might have highlighted drinking differences between the heterosexual women and SMW in our sample. In addition, bisexually behaving women were excluded from the sample, although recent studies have shown that bisexual or mostly heterosexual women report risk behaviors and health disparities that are as great or greater than lesbians. 15 Finally, women with preexisting diseases such as angina or heart disease were not included due to the focus of the original study.
However, this sample has many strengths compared to other convenience or population-based samples. The presence of an equivalent heterosexual comparison group among convenience samples is a weakness in the existing literature 27 but significantly strengthens our ability to assess disparities. The quantity of the information collected by ESTHER is much greater than that could be obtained by population-based samples seeking to answer the same questions. Clinically measured data reduce self-report bias, and the breadth of psychosocial measures enhances our ability to test predictors associated with health outcomes.
Unfortunately, there has been little research funding directed at SMW health disparities over the years. 45 Given the growing evidence that SMW are at significantly higher risk of having the metabolic syndrome and other CVD risk factors, additional funding and research are needed to determine possible mediators between sexual orientation and CVD risk, as well as to determine if SMW are at higher risk of CVD or all-cause mortality compared to heterosexuals.
Footnotes
Acknowledgments
The authors acknowledge the ESTHER study participants for their participation and time, as well as Dr. Edmund Ricci and Dr. John Marx for their assistance and support of this research. This article is dedicated to the memory of Dr. Deborah J. Aaron.
Author Disclosure Statement
No competing financial interests exist.