
Abstract
Background:
Sexual dysfunction is common among US women of reproductive age, many of whom use contraception. Various contraceptive methods have been associated with changes in sexual function.
Methods:
In this narrative review, we selected key articles based on our collective clinical experience. We summarized findings and best practice recommendations for addressing a woman's contraception and its potential relationship to sexual function.
Results:
Although some hormonal contraception is associated with sexual dysfunction, studies show mixed results based on route of administration and progestin component. Interestingly, nonuse of contraception also appears to be associated with sexual dysfunction and dissatisfaction. Low-dose vaginal estrogen, lubricants, and moisturizers may be used for treating vaginal dryness in the setting of hypoestrogenic states in reproductive-age women.
Conclusion:
A review of current contraception is appropriate for women presenting with sexual health concerns. Sexual dysfunction chronologically associated with a contraceptive may be addressed by trial of an alternative method. A multidisciplinary approach to treatment is recommended, including sex therapy, pelvic floor physical therapy, and consultation with a women's health specialist as needed.
Introduction
A
Overall, 27% of reproductive-age US women (aged 18–44 years) report sexual dysfunction, with low sexual desire being the most common, and 10.8% of these women also experience related distress. 3 Contraception may affect female sexual function both positively and negatively. However, relatively few recent studies have summarized the relationship of currently available combined hormonal contraceptive formulations, both oral and nonoral, as well as progestin-only and nonhormonal contraception, on female sexual functioning.
This is a narrative review of the impact of various contraceptives on female sexual function based on available evidence. We did not systematically review and summarize data from all existing epidemiologic or clinical studies, nor did we perform an exhaustive review of the literature to include all relevant studies. We selected articles on the basis of their applicability to US women and practical relevance to US clinicians. We provide clinical recommendations regarding the care of women with sexual health concerns potentially related to contraception. We hope to heighten clinician awareness and recognition of contraceptive methods as a factor affecting female sexual function and outline clinical management recommendations.
Summary of Evidence
Hormonal versus nonhormonal contraception
Findings from studies comparing women using nonhormonal contraception with those using hormonal methods have shown mixed results. A recent systematic review of 36 studies involving more than 13,000 women reported no significant change in sexual desire with use of oral combined hormonal contraception (CHC). 4 However, multiple studies have associated the use of oral CHC with adverse effects on sexual function, particularly sexual desire. 4 Smith et al., 5 in their retrospective study of about 1,100 women, reported that those using hormonal contraception of any type had less frequent sexual activity, arousal, pleasure, and orgasm and more difficulty with lubrication. Another study showed decreased measures of sexual interest and arousal 3 months after starting oral CHC, but no change in the enjoyment of sexual activity. 6 In a study involving 2,612 healthy medical students, CHC use was associated with a higher rate of female sexual dysfunction (FSD) than use of nonhormonal contraception. 7
In contrast, Spanish women attending a family planning clinic reported increased sexual desire at 12 months with the use of either oral CHC or copper IUC. 8 No significant differences were observed in Female Sexual Function Index (FSFI) scores between the groups. 8
The lack of consistency in findings highlights the complex and multifactorial nature of female sexual function and focuses on the need for a comprehensive approach to management.
Nonuse of contraception
The use of no contraception was associated with a higher rate of FSD than the use of either CHC or nonhormonal methods. 7 Furthermore, lower rates of sexual dysfunction were noted among women using either copper IUC (21%) or a levonorgestrel intrauterine system (LNG-IUS) (10%) than among women using no contraception (35%). 9 Another study 10 noted that the frequencies of sexual activity and sexual enjoyment were positively correlated with contraceptive satisfaction. Among other reasons, diminished sexual function perceived to be related to contraception may lead to nonuse of effective contraception, and conversely, nonuse of contraception may in itself be a factor in sexual dysfunction, perhaps owing to concerns about unintended pregnancy.
Oral CHC, androgens, and sexual function
Oral CHC has been linked to vaginal dryness and decreased lubrication, in addition to decreased arousal, sexual pleasure, and orgasm frequency and increased sexual pain. 5 These findings may be related to decreased circulating androgen levels with oral CHC use. This occurs by two mechanisms as follows: (1) Oral CHC increases sex hormone–binding globulin (SHBG) and decreases free testosterone, and (2) androgen production from the ovary is suppressed with oral CHC. 11 This antiandrogenic effect may be magnified with oral CHC containing an antiandrogenic progestin. 12
Although some studies have shown no change or improvement in sexual function with oral CHC use, both with drospirenone-containing 13,14 and levonorgestrel-containing formulations, 15 other studies have associated oral CHC use with adverse effects on sexual function, particularly sexual desire. 16 –19 One study showed decreased sexual interest and arousal 3 months after patients started oral CHC therapy, but no change in the enjoyment of sexual activity. 6 Interestingly, this study also found that 74% of study participants had a significant decrease in free testosterone without impairment of sexual interest or response.
Although evidence shows that testosterone has a role in sexual function for women, this conclusion is derived primarily from studies involving postmenopausal women reporting sexual dysfunction. Testosterone therapy in postmenopausal women has been associated with improvement in multiple dimensions of sexual function, including sexual desire, subjective arousal, vaginal blood flow, and frequency of orgasm. 20 However, the relevance of changes in androgen levels for an individual woman is unclear, and some women may be more sensitive to androgen level alteration than others. Most of the studies included in the previously mentioned systematic review 4 showed alterations in SHBG and testosterone levels, despite the overall lack of association between CHC and sexual desire.
The density of androgen receptors is greater in the external genitalia than in the vagina, 21 and androgens are thought to be necessary for glycoprotein synthesis in the formation of mucus. 22 Thus, a relative androgen deficiency could contribute to vulvar and vaginal dryness in addition to decreased arousal, sexual pleasure, orgasm frequency, and increased sexual pain 5 associated with oral CHC. Oral CHC has also been associated with vestibulodynia (vestibular pain) in several but not all studies. 23 –26 Longer duration of oral CHC use and younger age at initiation have been associated with higher relative risk of vestibulodynia. 23 The mixed study findings about the relationship between the use of oral CHC and sexual function do not allow for clear-cut recommendations, although the potential association begs a review of contraception in any reproductive-aged woman presenting with FSD.
The relationship of progestin androgenicity and sexual function
Any antiandrogenic effect may be magnified when the contraceptive contains a progestin with lower androgenicity. 12 Among the contraceptive progestins available in the United States, norgestrel and levonorgestrel are most androgenic; norethindrone and norethindrone acetate are less androgenic; and desogestrel, etonogestrel, norgestimate, dienogest, and drospirenone are the least androgenic. 27
With the potential effect of CHC on androgens in mind, investigators have focused on the relative androgenicity of CHC, as well as the addition of androgen to some CHC, to ameliorate the negative effect of CHC on sexual function. In a randomized controlled trial of drospirenone-containing OC followed by the addition of dehydroepiandrosterone (DHEA) or placebo to the same OC, the combination of DHEA and OC was not associated with improvement in sexual function and further negated the benefit of OC on acne. 28 Davis et al. 29 described improved sexual arousal and desire (using the FSFI) in women taking an antiandrogenic (dienogest) or an androgenic (levonorgestrel) progestin-containing oral CHC. These findings challenge the idea that an androgenic progestin is needed in oral CHC to improve FSD.
Nonoral hormonal contraception (non-LARC) and sexual function
Recent trends favor nonoral contraception for its convenience and efficacy, and a number of studies have examined the effect of oral compared with nonoral methods on sexual function. For example, in a comparison of the vaginal ring, oral CHC containing a third-generation progestin, subdermal contraception, and no hormonal contraception (control group), the three groups using hormonal contraception had increased positive indicators of sexual function (sexual interest and fantasies, orgasm number and intensity, and satisfaction) and decreased negative indicators (anxiety and discomfort). 30 In a comparison of levonorgestrel- and gestodene-containing OCs with the vaginal ring, authors noted that while women using either OC reported decreased sexual desire, ring users experienced a 75% increase in desire from baseline. 31 In a small prospective study, women using a vaginal ring in an extended manner experienced improvements in sexual function and reduced sexual distress on the FSFI and Female Sexual Distress Scale after 60 days and improvement in all quality of life (QOL) variables after 120 days. 32 Improvement was noted in sexual desire of women using a vaginal ring compared with a desogestrel-containing combined OC and a desogestrel-only OC. 33
In contrast, one study 34 reported similar sexual function scores for women using oral CHC and vaginal ring, whereas another 35 reported a slight decrease in libido with the ring compared with drospirenone-containing OC. Yet another study 36 noted a slight decrease in sexual function when women switched from oral CHC to a vaginal ring compared with a contraceptive patch. Notably, concerns were ring related rather than hormone related, and neither difference was thought to be clinically significant. 36 Therefore, the ring appears to be a reasonable alternative to oral CHC for women with sexual function concerns.
Among women using depomedroxyprogesterone acetate (DMPA), 5.8% experienced a decrease in libido. 37 Yet, in a comparison of DMPA and oral CHC, no difference was found in desire, arousal, and total FSFI scores despite lower testosterone levels in the women taking oral CHC. 38 Similarly, sexual interest was unchanged among adolescents taking DMPA compared with CHC over 41 months 39 and in adolescents using DMPA compared with nonhormonal contraception. 40 These findings support a lack of association with relative progestin androgenicity and sexual function. DMPA is unlikely to be associated with sexual function in women.
LARC and sexual function
LARC is gaining acceptance in the United States. In the Contraceptive CHOICE study, LARC was noted to be several-fold more efficacious than non-LARC and was more frequently selected by women when cost was not a factor in decision-making. 41 LARC has received endorsement by the American College of Obstetricians and Gynecologists as first-line contraception for women throughout their reproductive lifespan. 42
The results of studies involving LARC effects on sexual function are encouraging thus far. Authors of one study 9 noted lower rates of sexual dysfunction in women using either the copper IUC (21%) or LNG-IUS (10%) compared with no contraception. Moreover, they reported a significant positive association between LNG-IUS use and sexual desire, arousal, orgasm, and overall sexual function compared with no contraception. Of note, LNG-IUS was associated with greater desire, arousal, and overall sexual function than the copper IUC. Another study 43 likewise reported high satisfaction rates with both LNG-IUS and copper IUC, but no difference in sexual function overall and within psychological domains.
One study of the etonogestrel implant showed improvement in arousal, orgasm, satisfaction, and pain during sexual intercourse, 44 whereas another 30 reported increased positive indicators of sexual function (interest and fantasies, orgasm number and intensity, and satisfaction) and decreased negative indicators (anxiety and discomfort) in implant users compared with women using nonhormonal methods. In contrast, in another recent study, 45 no association was found between any LARC method and sexual satisfaction scores.
LARC methods appear to be a reasonable alternative for women experiencing sexual dysfunction while using CHC, especially oral formulations.
Vasectomy, tubal ligation, and sexual function
Many couples choose either male or female sterilization when childbearing is complete and sexual function may change for one or both partners after this intervention. A prospective study evaluated 76 couples using vasectomy as contraception with the International Index of Erectile Function, as well as the FSFI. 46,47 Although the International Index of Erectile Function scores were unchanged, the FSFI showed marked improvement in the domains of desire, arousal, orgasm, lubrication, and satisfaction. In another study, 48 Derogatis Sexual Functioning Inventory scores 49 were unchanged after 3 to 4 months among groups using oral CHC, injectable CHC, or IUC, while sterilized women had improved scores.
In contrast, FSFI scores were lower in all domains for 150 Iranian women using tubal ligation compared with 150 using condoms. 50 Not surprisingly, FSD rates were higher among women who regretted tubal ligation compared with those who did not. Furthermore, 12-Item Short Form Health Survey 51 scores likewise differed between the two groups, with the tubal ligation group having lower QOL scores. The study authors recommended counseling about the potential impact of tubal ligation on sexual function, although the study's generalizability may be limited. 50
In a study of men and women, sexual satisfaction did not differ by contraceptive method for women. 45 However, men reported the highest satisfaction when their partner used DMPA or tubal ligation, whereas condom use was associated with the lowest satisfaction rates.
As a nonhormonal contraceptive method, the effect of sterilization on sexual function extends beyond a simple hormonal effect into the psychological aspects of permanent pregnancy prevention, whether positive (i.e., relief and comfort in the knowledge that sexual activity will not result in pregnancy) or negative (i.e., regret that pregnancy is no longer possible).
Evaluation and Management Approach
Evaluation approach
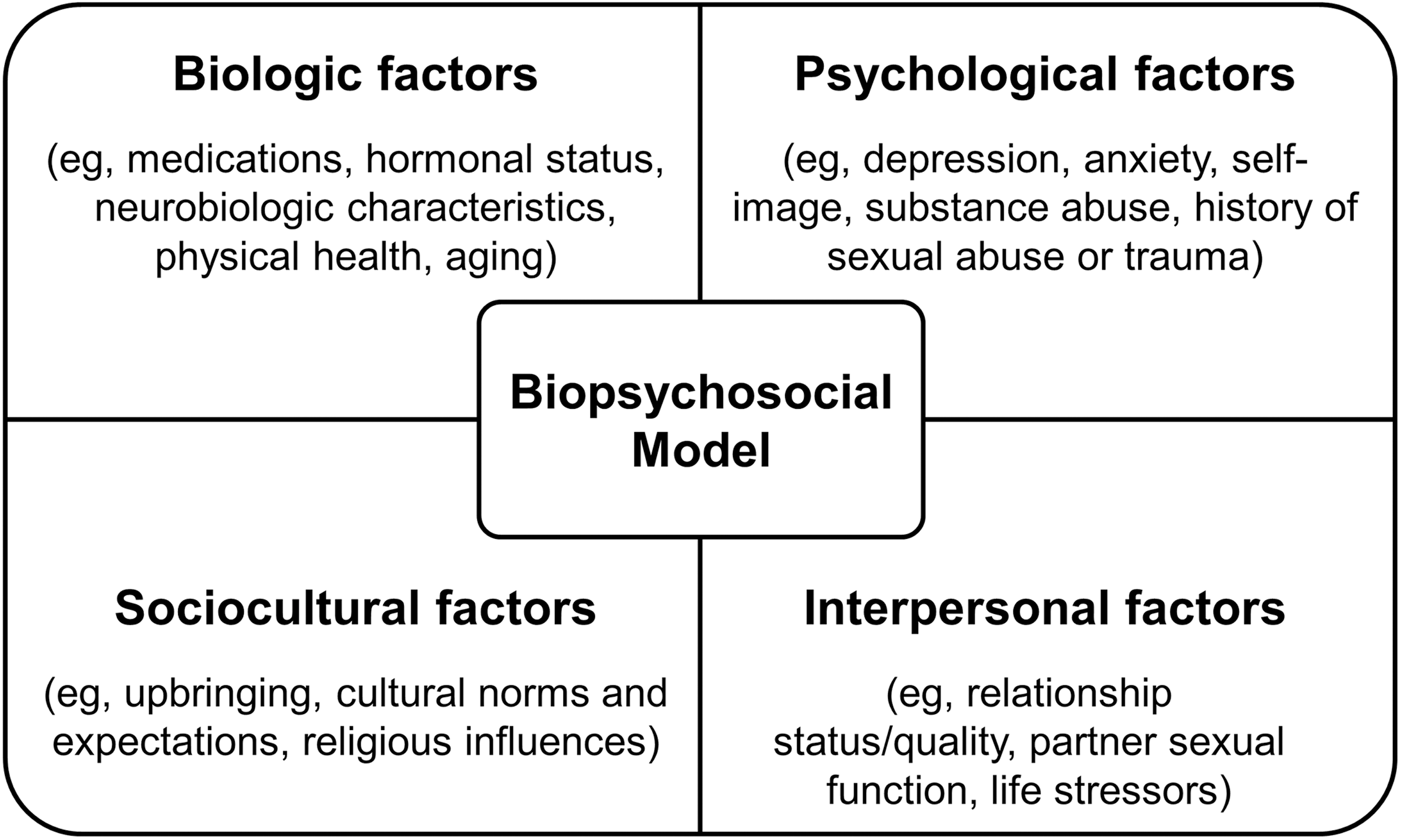
Sexual function in women is complex and multifactorial and is influenced by many biologic, psychological, and sociocultural factors. A directed history (Box 1) and physical examination are important for identifying all potential contributors. Identifying the timing of FSD onset may be helpful. If a problem with sexual function antedates initiation of CHC, for example, CHC is less likely to be the sole issue. However, if secondary vestibulodynia or decreased sexual desire develops while a woman is taking CHC, the CHC may be a contributing factor. Likewise, the biopsychosocial model (Fig. 1) can provide a framework for identifying the elements contributing to sexual dysfunction in women. 52 –54 For example, in the biologic domain, it is useful to review the medical history for contributing factors (e.g., history of pelvic surgery, diabetes mellitus, and cardiovascular or neurologic disease) and other medications that might be contributing (e.g., antidepressants, opioid pain medications, and some antihypertensive medications). Factors in the psychological domain that may have a role include stress, anxiety, depression, substance abuse, and body image concerns. Relationship factors that should be assessed include relationship quality, communication, and partner sexual function. In the sociocultural domain, societal or religious views and lack of sex education may contribute to sexual dysfunction. Consultation with a sex therapist may be helpful for women with sexual pain, low sexual desire, or relationship concerns. If a woman has difficulty with nonrelaxing pelvic floor dysfunction and has tender, tight pelvic floor muscles, working with a physical therapist who specializes in the pelvic floor may be particularly helpful. 55 A multidisciplinary approach to management is most effective. 52
Therapeutic approach
When CHC-related FSD is suspected, the recommended therapy is discontinuation of CHC with consideration of an alternative method of contraception, such as LNG-IUS, copper IUC, etonogestrel implant, or permanent sterilization of either partner when future fertility is not desired. The contraceptive ring may be an option for women who prefer CHC for cycle control and noncontraceptive benefits, but who experience FSD with oral CHC.
In a preliminary study, compounded topical estradiol-testosterone has been associated with subjective improvement in vestibular pain and normalization of SHBG and free testosterone levels. 11 This option may be a consideration in addition to discontinuing CHC.
First-line treatment of vaginal dryness and consequent dyspareunia includes the use of vaginal lubricants and moisturizers. Vaginal lubricants may provide temporary relief of discomfort from vaginal dryness associated with sexual activity. In the 2012 National Survey of Sexual Health and Behavior, 65.5% of 1,021 US women aged 18 years or older endorsed lubricant use; the reason cited most often was “to make sex more comfortable”. 56 The majority of women participating in a daily diary study reported positive perceptions of lubricant use, including increased pleasure and comfort. 57 Sharing information on the high frequency of use and positive results experienced across age-groups may be helpful in counseling reproductive-aged women about using lubricants. 57
In addition to lubricant use with sexual activity, vaginal moisturizers may be applied several times per week to help maintain vaginal moisture. 58 Strong evidence exists for the effectiveness of low-dose vaginal estrogen to treat genitourinary syndrome of menopause (GSM), which includes symptoms of vaginal dryness and lack of lubrication with intercourse, along with urinary tract symptoms. 59,60 The 2013 North American Menopause Society guideline on management of symptomatic GSM further acknowledges that hypoestrogenic states and subsequent GSM may occur in women of childbearing age, including lactating women. 59,61 The guidelines do not include specific recommendations for low-dose vaginal estrogen in reproductive-aged women with contraception- associated vulvar and vaginal dryness. However, topical estrogen has been successfully used for lactation-induced hypoestrogenism, often concurrently with various contraceptives, and we consider it a reasonable treatment option. 61
Conclusion
Given the prevalence of both FSD and contraception use, healthcare providers need to openly query women about FSD, evaluate sexual function concerns, and consider alternative contraceptive options when needed. While existing evidence for an association between sexual dysfunction and contraception is inconsistent and additional study is needed, women may present with concerns about sexual function associated with their method of contraception, particularly hormonal contraception. Review of a temporal relationship between the onset of FSD and initiation of contraception is warranted, as is an assessment with the biopsychosocial model of other potential contributing factors to FSD.
A multidisciplinary approach to the management of FSD is suggested, particularly when multiple contributing or complicating factors are identified (e.g., sexual pain, relationship discord, multiple comorbid medical conditions, and a history of sexual abuse) and may consist of consultations with a sex therapist, pelvic floor physical therapist, and sexual health specialist as indicated.
No clear guidelines exist for management of sexual dysfunction potentially associated with CHC in reproductive-aged women. A nonoral CHC, progestin-only, or nonhormonal LARC may be options for women with FSD associated with oral CHC. However, several studies have associated the use of any contraception with improvements in sexual function compared with no contraception, highlighting the multifaceted nature of the female sexual response. In addition to consideration of an alternate means of contraception, the use of vaginal lubricants for sexual activity and vaginal moisturizers used on a regular basis may be useful for women experiencing vaginal dryness and discomfort with sexual activity. Low-dose vaginal estrogen is appropriate for reproductive-age women with vaginal dryness due to hypoestrogenic states.
Footnotes
Author Disclosure Statement
P.M.C. receives research grant support from Merck and Co, Inc. K.L.M. and S.S.F. report no relevant financial interests.