
Abstract
Objective:
To characterize and compare cardiovascular disease (CVD) risk in HIV-infected and uninfected postmenopausal minority women using the Framingham Risk Score (FRS) as an assessment measure.
Methods:
A cross-sectional analysis was performed in 152 (109 HIV+, 43 HIV−) subjects from an existing study cohort of postmenopausal Hispanic and African American women. Data necessary to calculate FRS and menopause features were retrieved by retrospective chart review. Bivariate statistics was used to compare CVD risk factors. Multivariable linear regression was used to determine factors associated with FRS in HIV-infected women.
Results:
The HIV-infected group was younger, less obese, and with lower rates of diabetes versus controls. In a subset of age-matched participants, median FRS did not differ between groups (14.6 [IQR = 9.1, 21.6] vs. 15.5 [IQR = 12.3, 22.1]; p = 0.73). Fourteen percent of HIV-infected women meeting criteria for the low-risk FRS category (<10%) had a history of CVD, a similar rate as controls. HIV-infected women at intermediate/high CVD risk had higher rates of surgical menopause. According to 2013 clinical guidelines, more than half of HIV-infected women not prescribed statin therapy (52%) were eligible for treatment; however, statin therapy was similarly under-prescribed in uninfected women.
Conclusions:
In this study, CVD risk as assessed by the FRS was not significantly different by HIV status. Performance of the FRS may be compromised in postmenopausal HIV-infected minority women. HIV-infected and uninfected women may be undertreated with statin therapy. Large longitudinal cohorts and inclusion of subclinical measures of CVD are necessary to better characterize risk.
Introduction
T
In the United States, CVD results in the death of ∼400,000 women annually. 9 Risk of CVD increases profoundly during the menopause transition, 10 a time of rising follicular stimulating hormone (FSH) levels and diminished estrogen. Estrogen loss after menopause is associated with elevated levels of inflammatory mediators such as tumor necrosis factor-alpha (TNFα) and interleukin-6 (IL-6), 11 which are thought to play a role in the development of atherosclerosis. 12 An increase in traditional CVD risk factors, such as triglyceride and low-density lipoprotein (LDL) levels, was observed 1–3 years after the last menstrual period in the longitudinal multisite Study of Women's Health Across the Nation (SWAN). 13
Older HIV-infected women may be at especially high risk for CVD, due to the potentially additive effect of menopause and HIV. 14,15 HIV infection and menopause lead to some of the same metabolic manifestations, including central adiposity, adverse lipid profiles, and insulin resistance. 16 In the general population, the Framingham Risk Score (FRS) is recommended to assess CVD risk in women. 17 The FRS is a multivariable algorithm widely used to predict the risk of developing CVD over a 10-year period. 18 Previous studies have found that the FRS may underestimate CVD risk in people living with HIV because it does not account for the risk associated with chronic inflammation or ART use. 19 –21 At the same time, these studies did not include HIV-infected postmenopausal minority women, where CVD risk might be expected to be greater. Therefore, the purpose of this analysis was to characterize CVD risk in HIV-infected, postmenopausal minority women compared to an uninfected control group using the FRS as an assessment measure.
Methods
Study design and sample
After approval by the Institutional Review Board of Columbia University Medical Center, cross-sectional data were extracted from longitudinal cohorts of two existing datasets (R01AI065200, PI: Shane): 187 subject records (92 HIV+, 95 HIV−) from a cohort recruited in 2002–2007 22 and 248 (148 HIV+, 100 HIV−) from a cohort recruited in 2009–2014, both with a scheduled baseline and 12-month follow-up of patients. Participants were postmenopausal African American and Hispanic women ≥40 years of age recruited from infectious disease clinics and general internal medicine clinics at four medical centers in New York City. Blood samples were collected to confirm HIV status. Postmenopausal status (either spontaneous or surgically induced) was defined as amenorrhea for ≥12 consecutive months associated with either a single serum value for FSH of >30 mIU/mL or an FSH value >20 mIU/mL combined with an estradiol value <30 pg/mL. Women with metabolic bone disease, cancer, renal insufficiency (serum creatinine >1.5 mg/dL), osteoporosis, current glucocorticoids or menopause hormone therapy (HT) use, or past treatment for osteoporosis were excluded.
For the purposes of this study, additional data on menopause features and variables needed to calculate the FRS were collected from all available data in the medical record (i.e., inpatient, outpatient, and progress notes). Subject records were excluded from this analysis if data necessary to determine CVD risk were missing. As in a previous report, 23 participants were not excluded if they had a history of CVD; instead, this was used as an endpoint to assess the performance of the FRS as a CVD risk measure in HIV-infected women. After exclusions, the final sample included 152 (109 HIV+, 43 HIV−) subject records.
The primary independent variable, HIV infection, was confirmed by a positive test for either the antibody to HIV-1 or presence of HIV-1 RNA in the plasma. 22 To assess the impact of menopause-related factors, information on last menstrual period, age at menopause, years since menopause, and past use of menopause HT was obtained from the existing datasets. Natural menopause was defined as the spontaneous (natural) cessation of menses for at least 12 consecutive months. Surgical menopause was defined as menopause induced by the surgical removal of the ovaries (hysterectomy with bilateral oophorectomy). 24
Covariates available from the original medical record included: race/ethnicity, body mass index (BMI), chronic comorbidities (e.g., Hepatitis C infection, dyslipidemia, and diabetes), alcohol consumption, and injection drug use. 22,25 Information on HIV-1 RNA levels, current and nadir CD4, ART use (ever), ART regimen at time of enrollment, age at HIV diagnosis, and years since HIV diagnosis was also retrieved from the same datasets. Other covariates, including depression diagnosis, lipid values, and CVD diagnoses, were assessed by retrospective chart review.
Information on statin therapy prescription rates, including whether participants met the treatment guidelines recommended by the 2013 American College of Cardiology/American Heart Association (ACC/AHA), was retrieved from medical charts. According to ACC/AHA guidelines, the following types of patients qualify for therapy: age ≥21 years with LDL levels ≥190 mg/dL, age 40–75 years with diabetes and LDL 70–189 mg/dL, and individuals at risk for or with the clinical presence of CVD events (i.e., myocardial infarction, coronary artery disease, and nonfatal and fatal stroke). History of CVD (i.e., myocardial infarction, coronary artery disease, cerebrovascular disease, heart failure, and peripheral vascular disease) was determined using the International Classification of Diseases, Ninth Revision (ICD-9) codes for these diagnoses.
CVD risk ascertainment
The primary dependent variable was CVD risk, which was assessed using the FRS, a sex-based risk prediction model that estimates the 10-year risk of a cardiovascular event (e.g., myocardial infarction, coronary insufficiency, angina, stroke, transient ischemic attack, peripheral artery disease, and heart failure). 26 The individual's score ranges from 0% to 100% and is typically categorized as low (FRS <10%), intermediate (10%–20%), or high (FRS >20%) risk in non-HIV study populations. 27 In line with earlier HIV investigations, participants were grouped into low risk (FRS <10%) or intermediate/high risk (FRS ≥10%), 28 –30 given the high sensitivity (∼80%) of the FRS at a “cutoff” value of 10% observed in previous analyses. 31,32
The FRS was determined with the following set of variables: sex (male/female), age (years), systolic blood pressure (mmHg), treatment for hypertension (yes/no), current smoker (yes/no), diabetes (yes/no), total cholesterol (mg/dL), and high-density lipoprotein (mg/dL). 18 Information on blood pressure, hypertensive treatment, and lipid profile was retrieved from clinical and laboratory data closest to the screening visit. In the majority of cases (53%), the blood pressure measurement was calculated as the average of two blood pressure readings. 19,28
Statistical analysis
Data were analyzed using SPSS 22.0 software. Continuous variables were examined for normality with the Shapiro–Wilk normality test. Between-group differences were performed using the Student's t-test or the Mann–Whitney U test for continuous variables and χ 2 or Fisher's exact tests for categorical variables.
Using χ 2 tests, we compared the ratio of HIV-infected women with and without a history of CVD across these FRS groups. To determine predictors of FRS in the HIV-infected group, variables with p < 0.20 in between-group comparisons among HIV-infected women were entered into a linear regression model. Collinearity was assessed and redundant variables removed from the final model. All statistical tests were performed at a level of significance of p < 0.05.
Results
Sample characteristics
Sample characteristics are presented according to HIV status in Table 1 (n = 109 HIV+, 43 HIV−). Both groups of women were predominantly Hispanic and overweight-obese according to BMI criteria. Compared to the uninfected group, HIV-infected women were younger, more likely to be African American, had lower BMI, and were earlier in postmenopause. Age at menopause in both groups was similar (HIV+: 46.2 years vs. HIV−: 46.2 years), but the HIV-infected group had lower rates of surgical menopause (4% vs. 19%; p < 0.01). In terms of medical history, HIV-infected women demonstrated higher rates of alcohol use (≥1 drink/day) and clinical depression, but a lower rate of diabetes (26% vs. 49%; p < 0.01). While rates of current smoking and dyslipidemia were similar between groups, median triglyceride and total cholesterol levels were higher in HIV-infected women. Among HIV-infected women, ∼79% had previous ART exposure, with the majority (58%) receiving a protease inhibitor (PI)-based therapy.
Student's t-test or Mann–Whitney U test for continuous variables and χ 2 or Fisher's exact tests for categorical.
History of CVD was determined using International Classification of Diseases, Ninth Revision (ICD-9) codes for the following: coronary artery disease, myocardial infarction, cerebrovascular disease, peripheral vascular disease, and heart failure.
Calculated using the following variables: age, blood pressure, lipid profile, smoking status, diabetes status, and whether on hypertension treatment. FRS was calculated among individuals regardless of statin treatment.
Bold values are statistically significant.
ART, antiretroviral therapy; CVD, cardiovascular disease; FRS, Framingham Risk Score; HDL, high-density lipoprotein; IVDU, intravenous drug use; LDL, low-density lipoprotein; NRTI, nucleotide reverse transcriptase; NNRT, non-nucleotide reverse transcriptase; PI, protease inhibitor; SD, standard deviation.
History of CVD was similar between groups (25% vs. 33%; p = 0.33). Median (IQR) FRS was lower in HIV-infected than uninfected women (9.2 [IQR = 5.9, 16.3] vs. 13.5 [IQR = 8.3, 17.7]; p = 0.03). In a sensitivity analysis excluding women with a history of CVD, median FRS remained lower in the HIV-infected group, although not statistically significant (HIV+ = 8.6 [5.4, 15.8] vs. HIV− = 13.4 [7.6, 19.7]; p = 0.07). Given the group differences across several CVD risk factors (e.g., age, BMI, and diabetes), a post hoc analysis was conducted to compare FRS in an age-matched sample of HIV-infected and uninfected women aged >55 years (n = 40 HIV+, 40 HIV−). In this subsample, mean age (HIV+ = 60.1 ± 5.5 vs. HIV− = 60.3 ± 6.4; p = 0.76) and mean BMI (HIV+ = 28.3 ± 5.6 vs. HIV− = 30.9 ± 7.0; p = 0.07) were similar between groups. Although the rate of diabetes was still higher in HIV women, the difference was no longer statistically significant (HIV+ = 32.6% vs. HIV− = 47.5%; p = 0.17). In the post hoc analysis, there was no significant difference in median (IQR) FRS between the HIV-infected and uninfected groups (13.4 [IQR = 8.1, 17.1] vs. 14.0 [IQR = 8.3, 22.5]; p = 0.49).
Performance of the FRS in HIV-infected women
Using our subsample of age-matched HIV-infected and uninfected groups, we compared the proportion of women with a history of CVD in each FRS category (Fig. 1). Thirty-seven percent of the HIV-infected group was judged as low risk according to the FRS, compared to 30% of the uninfected controls (p = 0.49). Compared to 8% of the control group, 13% of HIV-infected women meeting criteria of the low risk category had a history of CVD (p = 0.72).
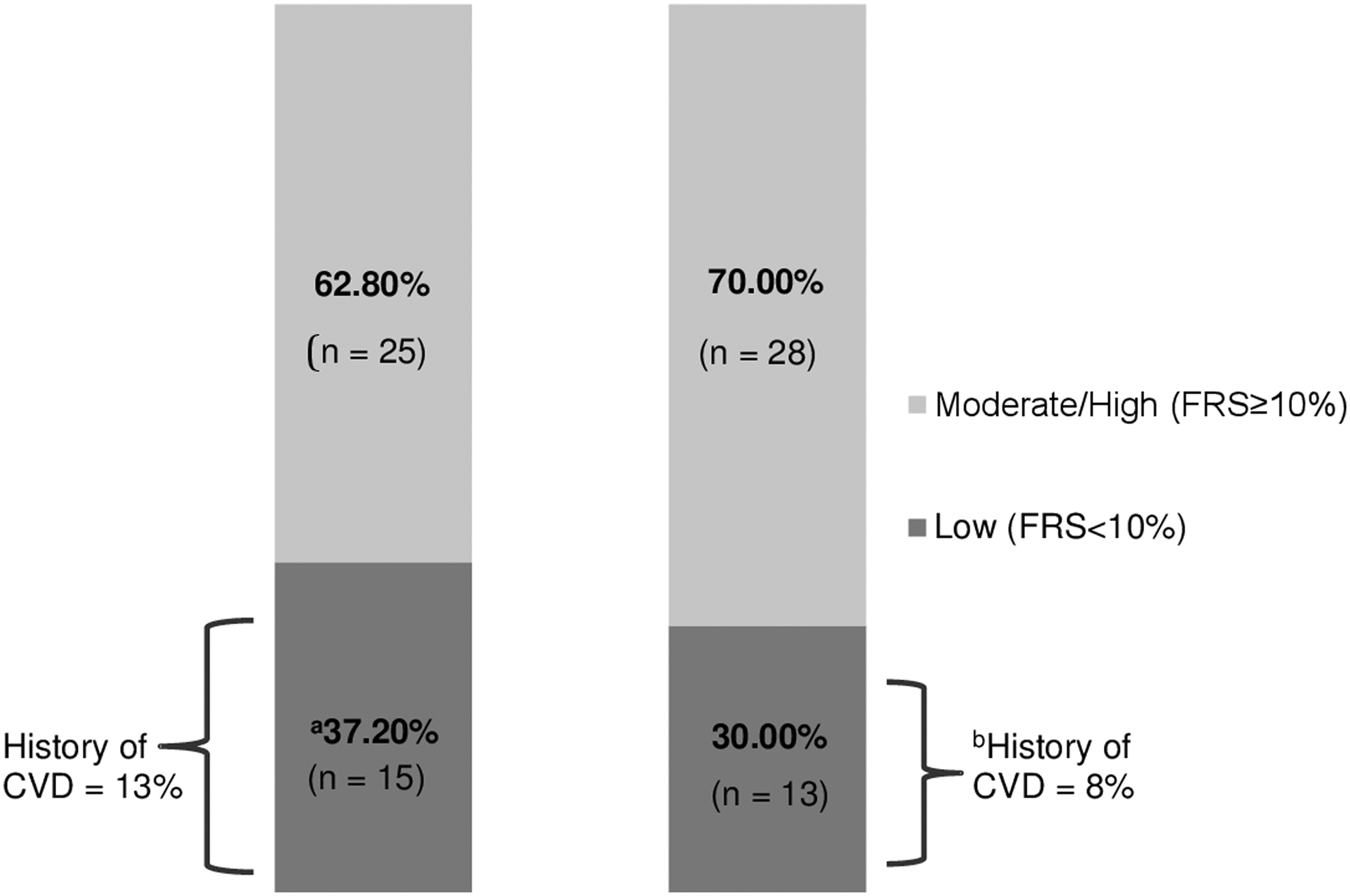
Using an age-matched (range 56–70 years) subsample of the HIV-infected and uninfected groups, the proportion of women with low (<10%) versus moderate/high (>10%) FRS was compared. The proportion of HIV-infected and uninfected women with a history of CVD in each FRS category was also compared. aBased on chi-squared analyses (37% vs. 30%; p = 0.49). bBased on chi-squared analyses (13% vs. 85%; p = 0.72). CVD, cardiovascular disease; FRS, Framingham Risk Score.
Factors associated with FRS in HIV-infected women
Table 2 presents characteristics of all HIV-infected women when grouped according to the low and intermediate/high FRS categories. HIV-infected women with FRS ≥10% were significantly older and later in postmenopause. History of surgical menopause and exposure to menopause HT did not differ by FRS category. Current CD4 cell counts were significantly lower among women with FRS <10%, but HIV-1 RNA and ART exposure were similar between groups. The intermediate/high risk group was significantly older at the time of HIV diagnosis and spent fewer years with HIV infection before menopause. Variables with p < 0.20 in bivariate analyses (Table 2) were entered into linear regression analyses. After removing redundant variables, and those strongly correlated with variables used to calculate FRS, older age at HIV diagnosis and higher CD4 cell counts were independently associated with worse FRS (Table 3). When time on ART was forced into the model, it attenuated the association between current CD4 cell counts and FRS. Past menopause HT approached significance (p = 0.08) in the multivariable model. In sensitivity analyses excluding patients with a CVD, older age at HIV diagnosis remained associated with FRS. However, the effect was attenuated after adjusting for current age (p = 0.07).
Between-group differences were performed using the Student's t-test or the Mann–Whitney U test for continuous variables and χ 2 or Fisher's exact tests for categorical variables.
Bold values are statistically significant.
BMI, body mass index; FSH, follicular stimulating hormone.
In the model, the dependent variable, FRS (%), was normalized using a log transformation. HIV-infected women were categorized into low FRS (<10%) versus intermediate/high FRS (≥10%) and group differences determined using chi-square tests for categorical variables and t-test or Mann–Whitney U for continuous variables. Variables with p < 0.20 were entered into regression model. Collinearity diagnostics were assessed and redundant variables removed (current age, time on ART). Multivariate model presented in this study adjusted for all factors listed.
Bold values are statistically significant.
Statin therapy
Only 31% (n = 31/109) of the total HIV-infected group was prescribed a statin compared to 58% of the uninfected group (p < 0.01) (Table 4). Despite this difference, the proportion of women not currently on statins with dyslipidemia meeting criteria for statin therapy according to the 2013 ACC/AHA guidelines 33 was similar between groups (52% vs. 67%, p = 0.26).
Based on chi-square analyses.
Recommendation based on the 2013 American College of Cardiology/American Heart Association guidelines. 33
Among those with dyslipidemia.
Bold values are statistically significant.
Discussion
This study is the first to examine CVD risk in HIV-infected postmenopausal minority women. Our hypothesis that the HIV-infected group would have higher (worse) FRS versus controls was not supported, either in the full sample or in the subanalysis of an older age-matched group. Among HIV-infected women, mean FRS was 9% in the full sample and 13% in the subanalysis scores higher than observed in other studies of middle-aged individuals, perhaps due to the older age, higher BMI, and postmenopausal status of our study population. 19,34
Moreover, a similar proportion of women with FRS <10% in the HIV-infected (13%) and uninfected groups (8%) had a history of CVD, indicating that the FRS may misclassify a similar percentage of postmenopausal minority women as low risk, regardless of HIV infection. This finding is consistent with earlier reports, mostly in younger HIV-infected men, in which more than half of the HIV-infected group at low risk for CVD by FRS (<10%) met criteria for atherosclerosis based on carotid intima-media thickness. 20,21 A potential explanation for the misclassification of HIV-infected women as low risk for CVD is that the FRS does not incorporate factors associated with HIV infection and therapy. Prior studies of CVD in HIV-infected individuals suggested that excess risk of CVD was associated with ART, 8,35 possibly due to its adverse metabolic effects, such as lipodystrophy. 36 Recent studies on the relationship between CVD and ART have conflicting results. While several observational studies have reported an increased risk of myocardial infarction with ART exposure, 37,38 others, such as an 8-year retrospective study of cardiovascular and cerebrovascular events in HIV-infected men and women, have found no such link. 39 This is similar to our analysis where ART was not associated with history of CVD. Conflicting evidence of the association between CVD and ART may, in part, be due to many studies in this field being short term and underpowered, 40 as in our analysis. In addition, because the majority of HIV-infected women in this study were ART experienced, it may have been difficult to fully assess the role of ART on CVD.
Immunologic factors, such as elevated serum cytokines or inflammatory markers, or CD4 counts have also been associated with CVD in HIV-infected individuals. 41,42 Among HIV-infected women (mean age 44 years) in the Veterans Aging Cohort Study, a recent analysis found that lower CD4 cell counts and higher HIV-1 RNA were associated with incident CVD. 43 Surprisingly, in our analysis, higher CD4 cell counts were associated with higher (worse) FRS. This relationship was attenuated when time on ART was entered into the model, suggesting that current CD4 was a surrogate marker for longer time on ART. While the impact of ART regimen in CVD remains uncertain, longer duration on ART has been correlated with a higher rate of coronary atherosclerotic plaques in HIV-infected men. 44
Older age at HIV diagnosis was independently associated with higher CVD risk as measured by the FRS, perhaps due to its association with current age, an important factor in the calculation of the FRS. Because this analysis was limited to cross-sectional data, we cannot determine whether women in the intermediate/high CVD risk group were already at elevated risk for CVD before HIV infection or whether HIV infection itself accelerated risk of CVD. In HIV-infected individuals, hypertension and diabetes have been observed at an earlier age than uninfected controls, 45 perhaps contributing to earlier CVD events in this population.
A notable finding in this investigation was the similarly low prescription rate for statin therapy in the records of both HIV-infected and uninfected women. Using the 2013 ACC/AHA guidelines, we found that more than half of the women not prescribed a statin were eligible for treatment. Although we were not able to ascertain provider treatment rationale, this observation is consistent with studies that found under-prescription of statin therapy for patients at high CVD risk in the general population 46 and among HIV-infected individuals. 47 In the general population, barriers to statin prescribing include provider concerns about cost, increased workload, and patient adherence to treatment. 48 For HIV-infected patients, concerns about potential drug-drug interactions between statins and ART regimens, specifically PIs, 49,50 may also influence provider behavior.
With regard to menopause features, our analyses revealed that HIV-infected women with intermediate/high FRS were later in the postmenopause stage and had higher rates of “ever use” menopause HT. The negative effects of estrogen withdrawal on cardiovascular health have been well established in the general population, 51 but less is understood about the menopause transition in HIV-infected women and the interaction between estrogen and HIV infection. Although evidence suggests that hysterectomy with or without bilateral oophorectomy may increase risk for CVD, 52,53 in the current study, surgical menopause did not predict FRS in HIV-infected women after adjusting for age. It is important to note that few HIV-infected women in this study had a bilateral oophorectomy (4%), thus limiting our ability to speculate about the significance of these findings.
There are several limitations to our analysis. First, given the cross-sectional nature of the study design, we could not assess the accuracy of the FRS at prediction of incident CVD events. Self-report of age at menopause/years since menopause was a limitation in this study, particularly given the association between HIV-related factors and amenorrhea. 54 We were also limited by the modest sample size and scope of the dataset, which precluded additional assessments of CVD risk, such as subclinical measures of atherosclerosis to better assess CVD risk and the predictive ability of the FRS. Another potential limitation is the use of the ACC/AHA 2013 criteria to assess statin therapy, given that some participants were enrolled before the release of these guidelines. Although the inclusion of those with a CVD history provided a measure of FRS performance, this also may have contributed to higher scores. In addition, to better compare CVD risk in HIV-infected versus uninfected women, more equivalent comparison groups would be necessary.
A particular strength of our design is that the comparison group of uninfected women was in some ways a positive “high-risk” control for the simultaneous comorbidities often seen in HIV patients that potentially confound results. While HIV-infected women in previous investigations had higher rates of smoking and substance abuse, 43,55 rates of these CVD risk factors were similar in our study groups. Another strength was that eligibility for inclusion was restricted to postmenopausal women and confirmed with reproductive hormone levels, permitting a more precise characterization of CVD risk associated with postmenopause status.
Conclusions
This study has shown that CVD risk in postmenopausal women, as assessed by the FRS, does not differ significantly by HIV status. Performance of the FRS may be compromised in postmenopausal women with HIV, but further longitudinal analyses in larger cohorts are necessary to appropriately assess the utility of the FRS in this population. This study also found that under-prescription of statin therapy is relatively common in both HIV-infected and uninfected women.
Investigations that compare the performance of all current CVD risk assessment tools (e.g., FRS, PROCAM, DAD, and ASCVD) are necessary to determine which, if any, best predicts CVD in this population. The use of a HIV-tailored CVD risk-prediction tool and recommendations for the administration of statins in HIV-infected individuals may help reduce risk of CVD in postmenopausal women with HIV. Future studies of CVD in this population would benefit from inclusion of subclinical vascular measures, as well as the use of inflammatory and immunologic markers to better characterize CVD risk and its association with HIV infection.
Footnotes
Acknowledgments
This work was supported by Grant R01AI065200 (PI: Shane). During the study period, Y.I.C. was supported as a predoctoral trainee by the National Institute of Nursing Research, National Institutes of Health (Training in Interdisciplinary Research to Prevent Infections, T32 NR013454). Y.I.C. is currently supported as a postdoctoral trainee by National Heart, Lung, and Blood Institute, National Institutes of Health (Cardiovascular Epidemiology Training Program, T32 HL083825). The authors thank the staff and participants of Columbia University Medical Center and Bronx-Lebanon Hospital Center.
Author Disclosure Statement
No competing financial interests exist.