
Abstract
Background:
This study utilizes a life-course framework to investigate whether maternal early life forced sexual intercourse operates in conjunction with health behaviors during adolescence, young adulthood, and the prenatal period to influence offspring birth weight.
Methods:
Using data from the 1994–2009 National Longitudinal Study of Adolescent Health (Add Health), we examined whether early life forced sexual intercourse predicted offspring birth weight through a mediated pathway, including depressive symptoms, substance use, and prenatal cigarette smoking. We stratify our analysis by socioeconomic status (SES) to determine whether the proposed pathways operate similarly, or differently, according to SES.
Results:
Our findings suggest that the pathways through which forced sexual intercourse affects offspring birth weight differ by SES. Among middle-to-high SES women, we found a mediated pathway linking forced sexual intercourse to offspring birth weight with prenatal cigarette smoking predicting lower offspring birth weight. Among low SES women, however, we did not find a mediated pathway linking forced sexual intercourse to birth weight. Findings suggest that prenatal cigarette smoking was not a mechanism of influence in the pathway between maternal early life forced sexual intercourse and offspring birth weight for low SES women.
Conclusions:
Our findings suggest that forced sexual intercourse may influence infant birth weight in the next generation. Infants born with a low birth weight are at increased risk for a myriad of adverse outcomes across the life-course. Study results suggest the importance of interventions designed to reduce behavioral risks and to support health promoting behaviors among survivors in the short term, in an effort to prevent long-term consequences among later-born offspring.
Introduction
F
Forced sexual intercourse is associated with both immediate and long-term adverse physical and mental health outcomes. 1,3 In the immediate aftermath of forced sexual intercourse, female survivors may experience physical injuries 1,4 and/or sexually transmitted diseases. 5 Long-term physical effects may include gynecological problems, such as chronic pelvic pain. 6 Psychological problems reported by survivors of forced sexual intercourse include generalized anxiety, eating disorders, sleep disorders, depression, and post-traumatic stress disorder. 7 –9
Given the high prevalence of forced sexual intercourse among women less than 18 years of age, studies have examined the behavioral health consequences among young survivors. Data from the Youth Risk Behavioral Study, a nationally representative, cross-sectional survey of U.S. high school students, revealed that adolescent women who had experienced forced sexual intercourse were more likely to report heavy smoking, binge drinking, feeling sad/hopeless, and suicidality. 5,10 –13
Despite our growing understanding of the prevalence and adverse outcomes associated with early life forced sexual intercourse, less is known about the consequences of early life forced sexual intercourse on the health of the next generation. From a life-course perspective, offspring birth weight is a consequence of maternal differential health trajectories that result from maternal early life risk exposures (including fetal) and the cumulative impact of risk exposures on maternal health across the lifespan. 14 Thus, infant birth weight is not only more than a combination of genetic factors and the prenatal environment but also a function of exposures to biopsychosocial and physical factors experienced by mothers across the lifespan. 15
There is consensus that early life risk factors are important in understanding outcomes in childhood and adulthood. 16 Using data from the Adverse Childhood Experiences (ACE) Study, researchers have found that adverse childhood events, including childhood abuse, household substance abuse, household mental illness, parental separation, and divorce are associated with an increased risk of substance use, mental health problems, and premature death in adulthood. 17,18
Research has shown a higher prevalence of adverse health behaviors, including depressive symptoms and substance use among women who experience forced sexual intercourse compared with their counterparts. 4,8,19 Similarly, early life risk factors have also been linked to an adverse birth outcome—defined here as infant low birth weight (less than 2500 g). In turn, low birth weight has been shown to adversely affect physical and mental health outcomes across the life-course. 20 Studies demonstrate that maternal early life adversity, such as low socioeconomic status (SES) in childhood, exposure to violence in childhood, and parental mental health problems in childhood, affect infant birth weight. 21,22 In addition, adverse health behaviors correlated with forced sexual intercourse also effect infant birth weight. 23,24 Given these studies, researchers examined mediated pathways linking maternal early life risk factors with offspring birth weight. 25,26 Using Add Health data, researchers found partially mediated pathways linking child maltreatment to offspring birth weight via adolescent substance use, prenatal smoking, adolescent depressive symptoms, and adult SES. 25
To date, there are no published empirical studies that examine pathways linking maternal early life forced sexual intercourse to offspring birth weight. To improve the well-being of survivors and to safeguard the health of the next generation, mechanism studies from a life-course perspective are needed to identify effective interventions that are designed to address the behavioral health needs of survivors. These studies have the potential to expand our understanding of birth disparities, which has implications for population health across the life-course.
Therefore, we expand on previous research to investigate whether maternal early life forced sexual intercourse, in conjunction with adverse health behaviors during adolescence, young adulthood, and the prenatal period, influenced offspring birth weight. Among women, economic disadvantage is associated with adverse outcomes, including rape 27 and offspring birth weight. 28 In addition, economic differences are present for behavioral risk consequences of forced sexual intercourse, such that low SES women are more likely to report depressive symptoms, substance use, and cigarette smoking compared with higher SES women. 29,30 Given these SES differences, we stratified our analysis by low and middle-to-high SES to determine whether the life-course pathways linking early life forced sexual intercourse to infant birth weight operate similarly, or differently, according to SES. Using this approach, we posit that low SES women compared with middle-to-high SES women who experience early life forced sexual intercourse are at an increased risk to deliver later-born low-birth-weight offspring.
To our knowledge, no study has examined the potential mechanisms linking early life forced sexual intercourse and offspring birth weight. In addressing this limitation, we highlight the importance of addressing behavioral risks among survivors to promote infant health.
Materials and Methods
Sample and procedure
We used data from the 1994–2009 National Longitudinal Study of Adolescent Health (Add Health), an ongoing nationally representative study beginning in grades 7 through 12, following respondents into adulthood. Add Health was designed to explore the social and environmental causes of health-related behaviors and health trajectories. 31 A systematic, random sample of 80 high schools and 52 associated feeder schools from across the United States was selected and then stratified according to region, urbanicity, school type, ethnic composition, and school size. During the 1994–1995 school year, more than 90,000 students aged 12–20 years responded to an in-school questionnaire in Wave I. From April 1995 to December 1995, Wave I in-home interviews were completed by 20,745 students aged 11 to 19 years (79% response rate).
From April 1996 to August 1996, all adolescents in grades 7 through 11 in Wave I were re-interviewed in 1996 at the Wave II in-home interview; of these, 16,706 students were selected for a second interview in 1996, and 13,568 students completed the interview. The response rate for Wave II was 88.2%. In 2001 and 2002, more than 15,000 Add Health respondents, 18 to 28 years old, were re-interviewed in Wave III. In 2008–2009, a fourth in-home interview of respondents aged 24 to 32 included a comprehensive personal interview where information on key life events was collected (response rate of 80.3% of eligible sample members). 29
Add Health study procedures were approved by the Human Subjects Review Committee at the University of North Carolina, Chapel Hill. For the present study, our sample consisted of 1903 nulliparous women (e.g., women who have no previous births) who participated in Waves I–IV and gave birth to a live singleton between Waves III and IV.
Measures
Offspring birth weight
Maternal self-reported birth outcome data were obtained from the Wave IV interview. An eligible birth was defined as singleton live birth delivered between 2003 and 2008, following the Wave III interview. Low birth weight was defined as less than 2500 g (1 = yes, 0 = no).
Early life forced sexual intercourse
In Waves I–II, female respondents were asked, “Were you ever physically forced to have sexual intercourse against your will?” Similar to previous studies, we chose to code respondents who answered “yes” (1 = yes, 0 = no) to forced sexual intercourse at either interview as having experienced early life forced sexual intercourse. 5,19
Adolescent and young adult substance use
In Waves II and III, respondents were asked questions about the frequency of their substance use. Based on these data, we measured adolescent and young adult substance use by using binary constructs as follows: 30-day cigarette use (smoked ≥1 day in the past month [vs. 0 days]); 30-day marijuana use (used marijuana ≥1 day in the past month [vs. no days]); binge drinking (≥5 drinks in a row in the past year [vs. never]); and illegal drug use (use of cocaine, crystal meth, or other illegal drugs [excluding marijuana] since month and year of previous interview [vs. never]). We did not use a gender-specific cutoff for binge drinking (e.g., ≥4 drinks for women), as only one question about ≥5 drinks was asked at both waves. The four substance use measures were then summed to create a composite score, ranging from 0 (no substance use) to 4 (use of all substances).
Depressive symptoms
Add Health included modified versions of a 20-item Center for Epidemiologic Depression Scale (CES-D). 32 In Wave II, adolescent depressive symptoms were assessed by a 19-item CES-D. Each item was rated on a scale of 0 (never or rarely) to 3 (most or all the time). CES-D scores in our sample ranged from 0 (no symptoms) to 47 (maximum depressive symptoms). Scores were summed to create a composite score and then standardized. In Wave III, young adult depressive symptoms were evaluated by using a 9-item version CES-D. CES-D scores in our sample ranged from 0 (no symptoms) to 25 (maximum depressive symptoms). Scores were summed to create a composite score and were then standardized. We elected to use a continuous rather than binary variable, because the former has been shown to greatly reduce the variation observed in the data. 33 The Cronbach's alpha for the CES-D was 0.88 in Wave II and 0.83 in Wave III.
Prenatal smoking
In Wave IV, respondents were asked “During this pregnancy with {initials} how many cigarettes did you smoke?” We measured prenatal cigarette smoking as a binary construct of respondents having reported smoking at least “10 or fewer” cigarettes a day as smokers during the prenatal period, versus respondents who report “a few cigarettes a week” or fewer. We chose to compare “high-risk” (daily) smokers with “moderate-to-minimal risk” (non-daily smokers and non-smokers) smokers so as to compare respondents engaging in high-risk smoking behaviors against those with moderate-to-minimal risk. This coding decision is based on the dose–response relationship between heavy prenatal smoking and increased risk of low birth weight. 34 In addition, the prenatal smoking variable reflects our interest in creating a variable that did not combine women who had a few cigarettes throughout the entirety of their pregnancy with women who smoked more consistently and/or more heavily during the prenatal period.
Adult SES
We consider receipt of public assistance as a proxy for adult SES in these analyses. 35 Receipt of public assistance was selected for these analyses to better capture features of disadvantage compared with income indicators. Particularly, categorization of total household income within the Add Health data prohibits the construction of an accurate poverty threshold variable that would incorporate household size. A respondent was coded as “low-SES” if the respondent, or others in her household, received any public assistance, welfare payments, or food stamps between Waves III and IV of interviews. All other respondents are coded as “middle-to-high SES.”
Statistical analyses
The relationships between maternal early forced sexual intercourse and offspring birth weight were evaluated via a two-group model approach by using structural equation modeling (SEM) in Stata Version 12.1. The Add Health study was based on a cluster sample in which clusters were sampled with unequal probability. Therefore, sampling weights were applied in all analyses. Missing data were accounted for by using full-information maximum likelihood estimation (FILM). First, we measure the bivariate correlations among our key study variables by the SES group. Second, we assess the hypothesized structural relationships between our model constructs by using SEM split by SES. We assess model fit by using (1) a chi-square test (χ2), (2) the comparative fit index (CFI), and (3) the root mean square error of approximation (RMSEA).
Results
Descriptive statistics
Descriptive statistics of the study variables are shown in Table 1. Women of low SES reported early life forced sexual intercourse at over twice the proportion of middle-to-high SES women (13.9% and 6.1%, respectively). Low SES women reported higher proportions of depressive symptoms and higher proportions of substance use during adolescence and young adulthood (with the exception of past-year binge drinking in young adulthood), compared with middle-to-high SES. The proportion of low SES women who reported prenatal smoking was 22.8% compared with 3.9% for middle-to-high SES women.
Bivariate correlations of variables utilized in the model are presented by SES in Table 2. For low SES women, early life forced sexual intercourse was significantly associated with adolescent depressive symptoms, adolescent and young adult substance use, and prenatal smoking. For middle-to-high SES women, early life forced sexual intercourse was significantly associated with adolescent and young adult substance use, and with young adult depressive symptoms.
p < 0.05.
p < 0.001.
p < 0.01.
SES, socioeconomic status.
Structural equation model
SEM was used to assess the effect of maternal early life forced sexual intercourse on offspring birth weight by adult SES. Adolescent substance use, adolescent depressive symptoms young adult substance use, young adult depressive symptoms, and prenatal smoking were tested as potential mediators of early life forced sexual intercourse. Given that these mediators may operate differently by SES, we stratified by adult SES. Figure 1a and b present the path model and the standardized model parameter estimates. The SEM model fit indicated a good representation of the data (χ2 = 65.03 and p < 0.001; CFI = 0.932, RMSEA = 0.046).
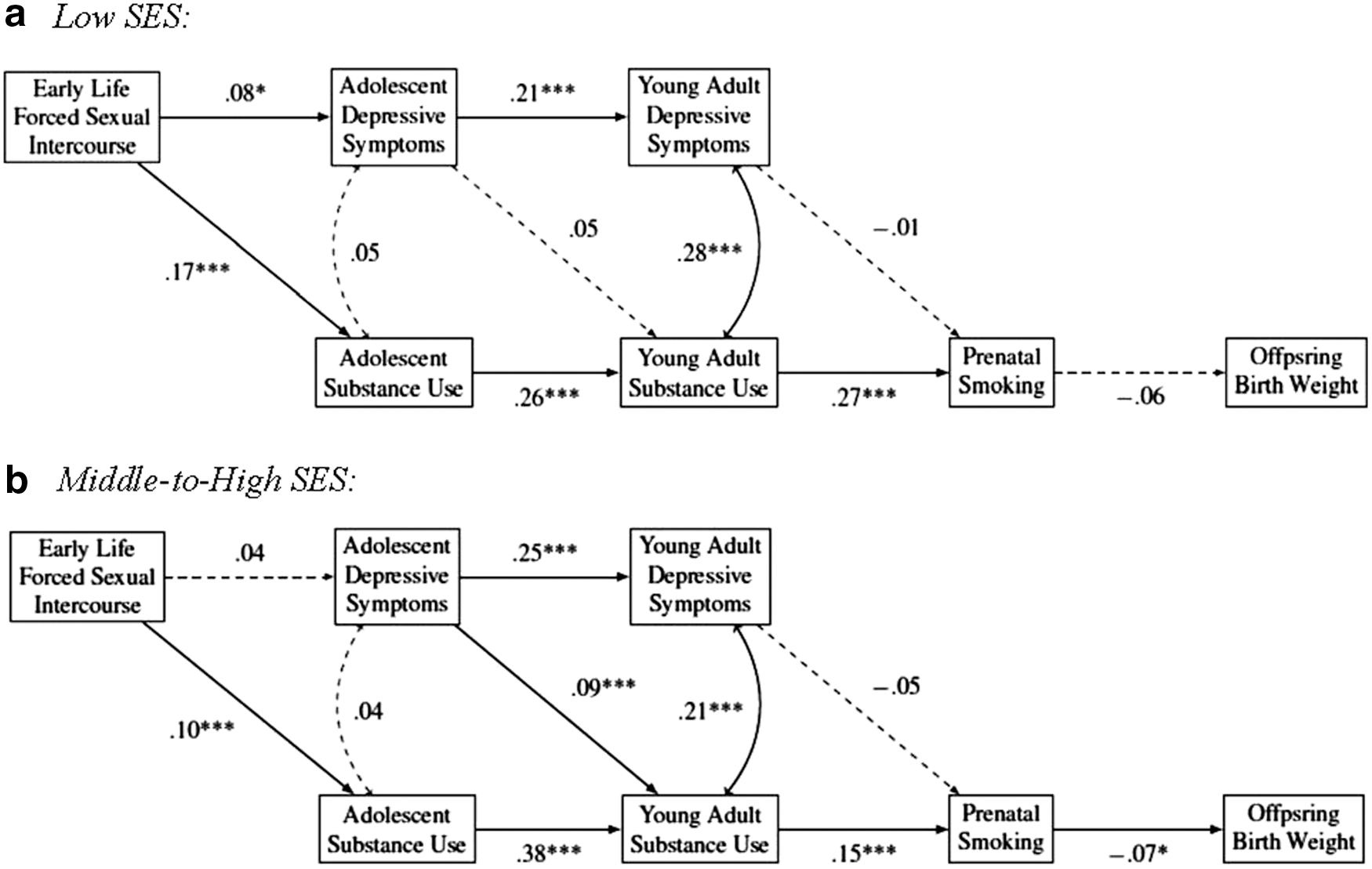
Early life forced sexual intercourse significantly predicted more adolescent depressive symptoms (β = 0.08, p = 0.019) for low SES respondents, but it had no significant effect on adolescent depressive symptoms for middle-to-high SES respondents (β = 0.04, p = 0.175). Early life forced sexual intercourse significantly predicted more substance use in adolescence for both SES groups (β = 0.17, p < 0.001 and β = 0.10, p < 0.001, respectively). Adolescent depressive symptoms significantly predicted more substance use in young adulthood for middle-to-high SES women (β = 0.09, p = 0.001), but not among low SES respondents (β = 0.05, p = 0.208). Adolescent substance use significantly predicted more young adult substance use among low- and middle-to-high SES respondents (β = 0.26, p < 0.001 and β = 0.38, p < 0.001, respectively). Adolescent depressive symptoms significantly predicted more young adult depressive symptoms for both SES groups (β = 0.21, p < 0.001 and β = 0.25, p < 0.001, respectively).
Young adult substance use significantly predicted prenatal smoking among low- and middle-to-high SES respondents (β = 0.27, p < 0.001 and β = 0.15, p < 0.001, respectively). However, young adult depressive symptoms did not significantly predict prenatal smoking for either SES group (β = −0.01, p = 0.694 and β = −0.05, p = 0.104, respectively). Prenatal smoking significantly predicted lower birth weight for middle-to-high SES respondents (β = −0.07, p = 0.020), but there is a lack of statistical evidence for a strong association for low SES respondents (β = −0.06, p = 0.080).
Discussion and Conclusion
Among middle-to-high SES women, findings suggest a mediated pathway from early life sexual intercourse on offspring birth weight through adolescent and young adult substance use and prenatal smoking. With regard to the mediated pathway from early life sexual intercourse to substance use, our findings are consistent with prior studies that found a history of forced sexual intercourse among adolescent women to be correlated with substance use, including heavy cigarette smoking, 13 marijuana use, 12 binge drinking, 11 and illicit drug use. 36
In the present study, a mechanism of influence of early life forced sexual intercourse on substance use appears to be through substance use in adolescence. 36 Possible explanations for the relationship between forced sexual intercourse and substance use include distress coping (substance use to reduce distress), emotion regulation (substance use to cope with negative emotion or to enhance positive emotion), and tension reduction (engaging in substance use may reduce stress). 37 Previous studies suggest that these cognitive mechanisms, in part, explain increased alcohol-related problems among survivors of sexual violence. 37,38 We also found a mediated pathway linking substance use and prenatal smoking. Although prenatal smoking rates are lower among pregnant women compared with non-pregnant women (15.9% vs. 24.6%), 39 women were more likely to smoke during pregnancy if they engaged in prenatal substance use. 40 Prenatal substance use (e.g., alcohol, illicit drugs) concurrent with cigarette smoking reduces the likelihood of achieving abstinence from cigarettes, 41 highlighting the difficulty in attaining cessation during pregnancy. In addition, precursors to prenatal substance use include pre-pregnancy illicit drug and alcohol use, 42 which may explain the mediated pathway between adolescent and young adult substance use and prenatal smoking.
Among middle-to-high SES women, findings suggest that prenatal smoking predicted lower offspring birth weight, which is consistent with a large body of research that links intrauterine exposure to tobacco to lower infant birth weight. 43 Women's birth outcomes are greatly affected by prenatal smoking behaviors. 44 Regular smoking during pregnancy has been linked to multiple negative health effects, including restricted fetal growth and preterm delivery. 24,43 Tobacco use during pregnancy doubles the risk of having a small-for-gestational-age infant due to intrauterine growth retardation and shortened length of gestation. Intrauterine hypoxia is the most widely accepted mechanism by which tobacco smoking may result in fetal growth restriction. 24
Our findings also suggest that among middle-to-high SES women, neither depressive symptoms during adolescence or young adulthood mediated the pathway between early life forced sexual intercourse and infant birth weight. This finding is consistent with previous studies that have demonstrated adolescent depressive symptoms, and adult depression did not mediate pathways linking maternal early life risk factors and infant birth weight. 25,26 We posit that middle-to-high SES women, due to availability of resources, may have access to support systems (e.g., mental health and sexual assault services) that are designed to assist them in the aftermath of their assault. These systems may mitigate the effects of the assault, which may explain why the association between early life forced sexual assault and adolescent depression symptoms did not reach statistical significance.
Interestingly, our findings suggest that the pathways through which forced sexual intercourse affects offspring birth weight differ by SES. Among low SES women, we found less support for a mediated pathway linking early life sexual intercourse to infant birth weight. Specifically, the pathway between early life forced sexual intercourse and offspring birth weight was partially mediated through adolescent and young adulthood substance use. However, prenatal smoking was not a mechanism of influence in the mediated pathway between early life sexual intercourse and offspring birth weight. This finding was unexpected. It is clear that low SES women have a higher prevalence of prenatal cigarette smoking compared with middle-to-high SES women 29 and in the present study, we found this to be true. Further, prenatal smoking is a risk factor for low infant birth weight. 24,43 However, our models and results highlight that the life-course pathways for women after forced sexual intercourse in early life differ by adult SES.
A potential explanation for the lack of evidence of a mediated pathway may be that early life forced sexual assault possibly produces physiological responses that differ for low SES and middle-to-high SES women. For example, there is a clear linear gradient relationship between physical health outcomes and SES, but not all disadvantaged individuals experience poor health. According to Chen et al., 45 some disadvantaged individuals do not experience an excess of health problems, despite experiencing repeated and severe life stressors, because they successfully engage in strategies to adapt by reappraising the meaning of stressors in self-affirming ways, and find meaning in challenging situations while maintaining optimism about their future.
For example, shift-and-persist strategies have been shown to buffer the effects of chronic disease risk among low SES individuals. In a national sample of adults, findings suggest that shift-and-persist strategies predicted lower allostatic load among those from low SES childhood backgrounds. 46 Although this needs to be empirically tested, it is posited that shift-and-persist strategies may buffer the effects of poor health behaviors among low SES individuals. 47 Evidence suggests that low SES individuals may benefit more than high SES individuals from shift-and-persist strategies, whereas high SES individuals, given their greater resources, may benefit more from proactive strategies that focus on eliminating stressors. This highlights the importance of socioeconomic context in understanding how coping strategies influence health. 45,47 Although future studies are needed, our results may, in part, reflect the successful use of shift-and-persist strategies by low SES women in our study, which, in turn, buffered the effects of prenatal smoking on offspring birth weight.
The present study provides new information regarding the inter-generational effects of early life forced sexual intercourse and offspring birth weight in a nationally representative sample of women first interviewed when they were adolescents. However, the findings should be interpreted in light of the following limitations. First, we relied on mothers' reports of birth weight, without verification from clinical records. It should be noted that the use of maternal recollection of offspring birth weight is a valid method of obtaining data when clinical verification is unavailable. 48 Second, undesirable substance use behaviors, including prenatal smoking, may be underreported. Third, the data for this study did not include information on when the forced sexual experience occurred, how often it occurred, and information on the perpetrators. It is possible that the context in which early life forced sexual intercourse occurred may result in varied responses. In light of these data limitations, the magnitude of our findings may be biased toward the null. Fourth, data for the present study were drawn from a sample of women who were initially interviewed as high school students. Thus, our findings cannot be generalized to women who were not enrolled and/or attending school. Fifth, we stratified our models by SES in adulthood, so the role of SES across the life-course is not captured in this analysis. However, past research has documented the relative stability of SES across the life-course. 49,50 This is supported in our sample, as 67.1% of respondents whose families received public assistance in early life also received public assistance as adults. Further, in preliminary analyses, we stratified our sample according to early life SES and the substantive conclusions remained the same. Finally, data were unavailable regarding the availability and frequency by which survivors in the study accessed sexual violence support services.
Our findings highlight that early life forced sexual intercourse is a major public health concern because of its effects on survivors and their later-born children. Given this, as a society we must continually strive to support policies that are designed to eliminate sexual violence against women. Until that goal is attained, we must adopt strategies to mitigate the impact of maternal early life forced sexual intercourse on offspring birth weight. First, our findings suggest that universal screening protocols must be implemented in primary healthcare settings to screen patients for past or present experiences of sexual violence. This is paramount in prenatal care settings. Mediated pathways identified in our study highlight the need for universal screening to assess and quantify behavioral risk to determine whether survivors are in need of additional evaluation and referral to behavioral health services. 51 Second, our findings suggest that both low and middle-to-high SES women continue to smoke during pregnancy, although low SES women smoked at a greater rate. This suggests that prenatal smoking cessation strategies and interventions are needed to target modifiable risk factors based on SES. For example, interventions that are designed to address smoking among low SES pregnant women should focus on social barriers to treatment adherence; some of these factors include high cigarette use, lack of childcare, transportation, insufficient knowledge of health risks and cessation methods, and culturally relevant cessation support. 29 Among middle-to-high SES pregnant women, strategies to reduce smoking should include screening for pre-pregnancy substance use, namely alcohol use. In our study, substance use before pregnancy was a significant mediated pathway linking prenatal smoking to offspring birth weight. Although prenatal illicit drug use is relatively low, studies show that alcohol use in pregnancy ranges between 15% and 20%. 52 In addition, drinking alcohol before pregnancy is associated with drinking during pregnancy and high SES women are more likely to drink alcohol during pregnancy. 53 Taken together, healthcare providers must screen all pregnant women for prenatal alcohol use. However, special attention should be given to using screening instruments that capture alcohol use patterns of high SES drinkers. The T-ACE, a 4-item screening tool, has been validated among pregnant populations and captures a range of alcohol use, including current prenatal drinking, pre-pregnancy risky drinking (2 or more drinks per day), and lifetime alcohol use based on DSM-III-R diagnostic criteria. 54 Lastly, future studies are needed to examine whether coping strategies adopted by low SES pregnant women, such as shift-and-persist, reduce the detrimental effects of early life sexual assault on later-born offspring.
Footnotes
Acknowledgments
This research uses data from Add Health, a program project directed by Kathleen Mullan Harris and designed by J. Richard Udry, Peter S. Bearman, and Kathleen Mullan Harris at the University of North Carolina at Chapel Hill, and funded by grant P01-HD31921 from the Eunice Kennedy Shriver National Institute of Child Health and Human Development, with cooperative funding from 23 other federal agencies and foundations. Special acknowledgment is due to Ronald R. Rindfuss and Barbara Entwisle for assistance in the original design. Information on how to obtain the Add Health data files is available on the Add Health website (
Author Disclosure Statement
No competing financial interests exist.