
Abstract
Background:
One caregiver relationship that has been neglected in caregiver depression research is the daughter-in-law. Compared with Western countries, in which those who are closer in familial relationships such as the spouse or child usually take care of the patient, in many Asian countries, the daughter-in-law often assumes the caretaker role. However, not much research has been done on how this relationship may result in different caregiver outcomes. We sought to identify whether the association between patient characteristics and caregiver depressive symptoms differs according to the familial relationship between caregiver and patient.
Materials and Methods:
Ninety-five daughter (n = 47) and daughter-in-law (n = 48) caregivers of dementia patients were asked to report their own depressive symptoms and patient behavioral symptoms. Patients' cognitive abilities, daily activities, and global dementia ratings were obtained. Hierarchical linear regression was employed to determine predictors of depressive symptoms.
Results:
Daughters-in-law had marginally higher depressive scores. After adjusting for caregiver and patient characteristics, in both groups, greater dependency in activities of daily living and more severe and frequent behavioral symptoms predicted higher caregiver depressive scores. However, greater severity and frequency of behavioral symptoms predicted depression to a greater degree in daughters compared with daughters-in-law.
Conclusions:
Although behavioral symptoms predicted depression in both caregiver groups, the association was much stronger for daughters. This suggests that the emotional relationship between the daughter and patient exacerbates the negative effect of behavioral symptoms on caregiver depression. The familial relationship between the caregiver and dementia patient should be considered in managing caregiver stress.
Introduction
T
It is well established that patient characteristics, such as dependency on activities of daily living and behavioral symptoms, are key predictors of caregiver depression. 8,9 However, less research has been done on characteristics of the caregiver that determine caregiver depression. A recent meta-analysis on predictors of depressive symptoms in caregivers of dementia patients reported that certain features of caregivers, such as being female, were associated with severer depression. Caregivers were also affected by different types of care-related problems. For example, older caregivers were stressed because of the physical strains of caregiving, whereas younger caregivers were under the weight of both providing care and having to work at their jobs. 8 Therefore, identifying how different caregiver characteristics stress caregivers in disparate ways is essential for understanding how caregiving affects well-being and for developing better interventions.
One caregiver characteristic that is related to caregiver well-being, but has not been studied extensively, is the type of relationship between the caregiver and the patient. Studies on this subject have found associations between the relationship type and caregiver depressive symptoms. For example, spouse caregivers tend to be more depressed than other caregivers, including sons, daughters, or other relatives. 8,10 –12 One study found that the perception of the patient's quality of life was most negative in daughter compared with spouse and son caregivers, and this perception predicted the caregiver's mental health and burden. 13 A meta-analysis on depressive symptoms of adult children and children-in-law caregivers showed that children-in-law had higher depression and perceived fewer uplifts of caregiving compared with children caregivers. However, children-in-law also reported lower strain in their jobs due to caregiving demands compared with children. 12
One caregiver relationship that has been neglected in the research on caregiver depression is the daughter-in-law. In the United States and Western Europe, many dementia patients are reported to be taken care of by the spouses, daughters, or sons of the patient, but less by daughters-in-law. 14,15 However, in many Asian countries, the majority of dementia patients tend to receive the care by daughters-in-law or daughters. 3,16,17 This is because cultural factors, such as Confucian virtues of caring for the husband's family, heavily influence caregiving practices in these countries.
For example, a study done in 2007 found that in South Korea, most caregivers are women (73.7%) and of those women, the daughter-in-law was the most frequently (40.5%) reported relationship. 18 This is in contrast to Western countries, in which those who are closer in familial relationship such as the spouse or child take care of the patient. In many Asian countries, one with a weaker familial tie to the patient such as the daughter-in-law has an important role in caregiving. This weaker familial tie may result in different outcomes to the caregiver's well-being. Therefore, there is a need for research to identify the characteristics and outcomes of the daughter-in-law caregiver relationship.
As of now, there are few studies on the caregiving of daughters-in-law and even fewer quantitative investigations, despite the fact that they constitute a significant percentage of caregivers in many Asian countries. 3 One study compared the experiences of daughter and daughter-in-law caregivers in Korea and found that emotional and physical health outcomes did not differ in the two groups. 19 However, this study did not look specifically into how predictors of caregiver depression differ according to the caregiver relationship.
Our article addresses these limitations of the current literature on caregiver relationship and caregiver depression by collecting data on daughter and daughter-in-law caregivers of dementia patients and by assessing how the associations between predictors and depressive symptoms differ according to caregiver relationship type. The objective of the current study was to identify whether depressive symptoms differ between daughter and daughter-in-law caregivers and whether those symptoms are predicted by different factors. We were especially interested in how the patient's behavioral symptoms and daily functioning predict the caregiver's depressive symptoms and whether the associations of these variables differ between daughters and daughters-in-law.
Materials and Methods
Participants
Ninety-five caregivers (47 daughters and 48 daughters-in-law) of patients with mild to severe dementia participated. Participants were the caregivers of dementia patients in a general hospital. By accessing the hospital database and calling each household, we were able make a list of patients who had been diagnosed with having dementia, assessed on cognitive functioning, and whose primary caregiver was the daughter or daughter-in-law. This led to identifying 145 caregivers. Of those, 132 agreed to participate in the study, yielding a 9.6% refusal rate. Eight caregivers did not return the surveys, and 29 did not meet our caregiver criteria of providing care for at least 3 hours a day and for at least 3 days per week. The patients of the participants were diagnosed with having dementia based on the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition (DSM-IV), 20 by geriatric physicians of the hospital. Among the 95 patients, 68 had been diagnosed with having Alzheimer's disease, 18 with vascular dementia, 5 with Lewy Body dementia, 3 with frontotemporal dementia, and 1 with dementia otherwise not specified.
Participants were asked to fill out a questionnaire packet containing the survey materials. They either completed it when they visited the hospital or through postal mail. All participants provided written informed consent and were paid for their participation. The Seoul National University Boramae Hospital Institutional Review Board approved this study.
Measures
Caregiver characteristics
Caregivers self-reported on their age, education level, marital status, and relationship to the patient. They completed the Korean version of the Center for Epidemiological Studies Depression scale (CES-D; scale range 0–60, with higher scores indicating greater depression) 21,22 to indicate the level of their depressive symptoms, our main construct of interest.
Patient characteristics
Data on patients were both collected through the hospital's database and provided by caregivers. We used scores on the Korean version of the Neuropsychiatric Inventory (NPI) 23,24 to calculate a measure of behavioral symptoms. For each of the 12 symptom categories (delusions, hallucinations, agitation, depression/dysphoria, anxiety, euphoria, apathy, disinhibition, irritability, aberrant motor behavior, sleep and nighttime behavior disturbances, and appetite and eating disorders) on the NPI, we multiplied the frequency (1 = less than once per week, 2 = about once per week, 3 = several times per week, 4 = daily) and the severity (1 = mild, 2 = moderate, 3 = severe) scores, and then added the 12 scores to create a total Neuropsychiatric Inventory Frequency-Severity (NPI-FS) score. Scores on the Korean version of the Mini-Mental State Examination (MMSE) 25,26 were used as an indicator of patients' cognitive function. Global scores on the Korean version of the Clinical Dementia Rating Scale (CDRG) 27,28 were used to indicate the clinical severity of patient's illness. The patient's dependency in activities of daily living was measured by the Korean version of the Barthel Index of Activities of Daily Living (BADL). 29,30 These scores were obtained through the hospital database, and we only used scores from assessments within 6 months of the time of study. Table 1 displays information on demographics for caregivers and patients, including age, sex, education level, the CES-D scores of the caregivers, NPI-FS scores, MMSE scores, CDRG scores, and BADL scores of the patients.
The values are represented as mean ± standard deviation.
t and p-values represent those from independent samples t-tests unless specified with a χ 2, which represents a chi-square test.
BADL, Barthel Index of Activities of Daily Living (range 0–20); CDRG, Global Clinical Dementia Rating (range 0–3); CES-D, Center for Epidemiological Studies Depression scale (range 0–60); MMSE, Mini-Mental State Examination (range 0–30); NPI-FS, Neuropsychiatric Inventory frequency and severity (range 0–144).
Statistical analysis
To see if there were any differences in demographics and patient/caregiver characteristics between the daughters and daughters-in-law, we conducted t-tests to compare patient age, patient education years, patient NPI-FS scores, MMSE scores, CDRG scores, BADL scores, caregiver age, and caregiver education years. In addition, we performed chi-square tests to see differences in patient sex and caregiver marital status.
To see the associations between caregiver relationship type, patient characteristics, caregiver characteristics, and caregiver depressive symptoms, we conducted hierarchical linear regression analysis with caregiver depressive scores as the dependent variable. In the first step of the hierarchical analysis, we included caregiver relationship (coded as daughter-in-law = 0, daughter = 1). The second step included patient characteristics such as patient age, patient sex (coded as male = 0, female = 1), patient education years, patient NPI-FS scores, MMSE scores, CDRG scores, and BADL scores. In the third step, we included caregiver age, caregiver marital status (coded as nonmarried = 0, married = 1), and caregiver education years. In the fourth step, we included the two-way interaction term for caregiver relationship and NPI-FS scores.
Results
The t-tests showed that the two groups significantly differed in patient age, t(93) = −2.93, p = 0.004, and caregiver marital status, χ 2(1, N = 95) = 13.33, p < 0.001. A greater percentage of daughters-in-law were married and their patients were older. Additionally, daughters-in-law had marginally higher depression scores, t(93) = −1.94, p = 0.056 (Table 1).
Results of the hierarchical linear regression showed the first model to be marginally significant, p = 0.056, and the next three models significant (ps < 0.001, 0.001, <0.001, respectively). The final model accounted for 35.3% of the total variance (R 2) in depressive scores. In itself, caregiver relationship marginally significantly predicted depressive scores, B = −4.79, t(93) = −1.94, p = 0.056, in that daughters-in-law had greater depressive symptoms. However, this association became nonsignificant from the second model when other variables were controlled for. No other predictors, such as MMSE scores, were significant.
In the second model, NPI-FS scores positively predicted depressive symptoms, in that the higher the NPI-FS score, the higher the depressive score, B = 0.24, t(85) = 4.37, p < 0.001. BADL scores negatively predicted depressive scores, in that the higher the BADL score, the lower the depressive score, B = −0.66, t(85) = −2.62, p = 0.01. No other predictors were significant. In the third model, the pattern and significance level of those predictors were the same [with statistics for NPI-FS being B = 0.23, t(82) = 4.21, p < 0.001, and BADL being B = −0.66, t(82) = −2.53, p = 0.01].
In the fourth model, the association of NPI-FS scores with depressive scores was qualified by a significant interaction between NPI-FS and caregiver relationship, B = 0.31, t = 2.46, p = 0.02. Probing the interaction using an online calculator by Preacher et al. 31 showed that in daughters, the simple slope of the NPI-FS scores was 0.49 [SE = 0.12, t(81) = 4.14, p < 0.001], whereas in daughters-in-law, the simple slope of NPI-FS scores on depressive scores was 0.18 [SE = 0.06, t(81) = 3.19, p = 0.002]. This indicates a stronger positive association between NPI-FS scores and depressive scores in daughters compared with daughters-in-law (see Fig. 1 for a graphical depiction of the interaction). An additional model, which included the two-way interaction term of caregiver relationship type with BADL, did not show any significant association with the dependent variable (Fig. 2). Table 2 shows the regression coefficients and their significance for all four regression models.
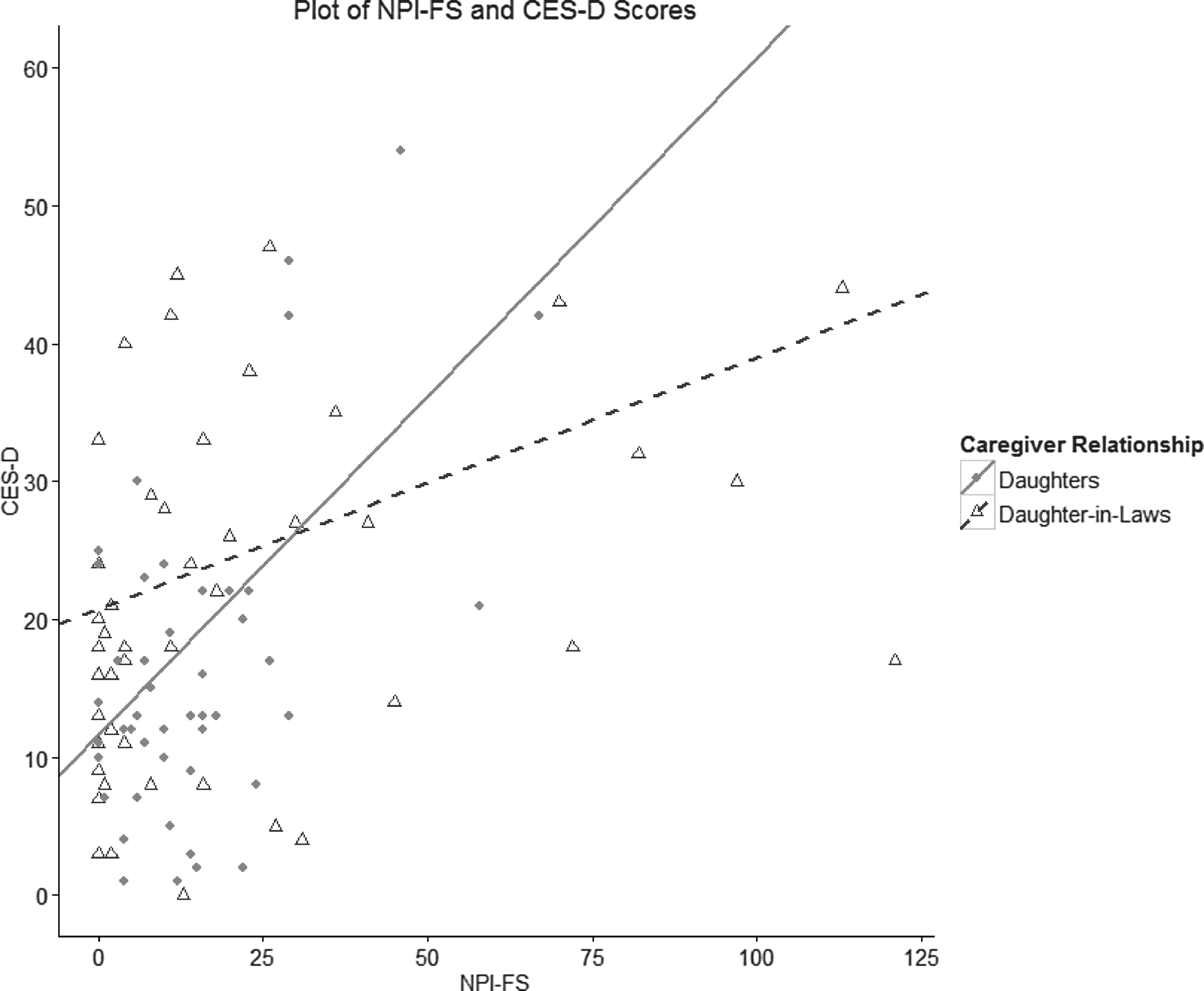
Regression analysis was conducted to determine the association between patient behavioral symptoms and caregiver depression in 47 daughter and 48 daughter-in-law caregivers of dementia patients. Featured are the scatterplot and simple slope regression lines of NPI-FS (range 0–144) scores and the CES-D (range 0–60) scores according to caregiver relationship. CES-D, Center for Epidemiological Studies Depression scale; NPI-FS, Neuropsychiatric Inventory Frequency-Severity. Solid line and circles refer to daughters, and dashed line and triangles refer to daughter-in-laws.
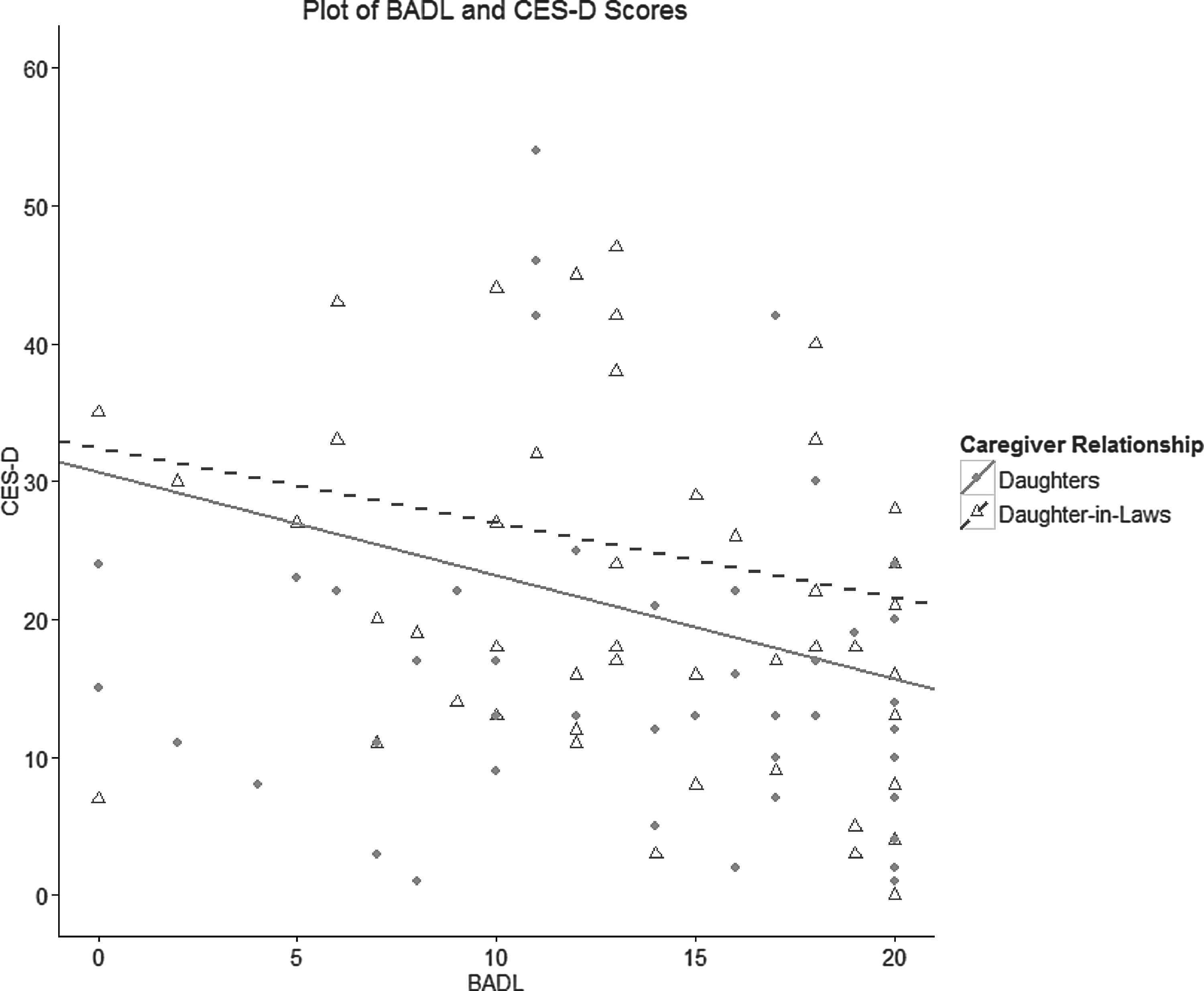
Regression analysis was conducted to determine the association between patient dependency in activities of daily living and caregiver depression in 47 daughter and 48 daughter-in-law caregivers of dementia patients. Featured are the scatterplot and simple slope regression lines of BADL (range 0–20) scores and the CES-D (range 0–60) scale scores according to caregiver relationship. BADL, Barthel Index of Activities of Daily Living. Solid line and circles refer to daughters, and dashed line and triangles refer to daughter-in-laws.
Unstandardized regression coefficients are shown as they are recommended for models with categorical predictors. 42
* p < 0.05, ** p < 0.01, *** p < 0.001.
We also conducted additional analyses to ensure the quality of our results. First, we ran a stratified analysis, modeling depression on predictors (patient and caregiver characteristics) for daughters and daughters-in-law separately. Results of the regressions on the two separate groups corroborated our previous analysis: in both groups, NPI-FS scores positively predicted depression, and the effect was stronger for daughters compared with daughters-in-law. The stratified analysis also showed that MMSE positively predicted depression for daughters, but not for daughters-in-law. BADL scores were negatively associated with depression for daughters, but not for daughters-in-law. However, only a regression with interaction terms can statistically test if the slopes of those predictors are significantly different between the two groups. To test this, we ran a regression with the three interaction terms of caregiver relationship with NPI-FS scores, with MMSE scores, and with BADL scores. Results showed only the interaction term of NPI-FS scores to be significant, B = 0.37, t(79) = 2.76, p = 0.007, indicating that only the slopes of depression on NPI-FS were different between daughters and daughters-in-law.
Discussion
We collected data from daughter and daughter-in-law caregivers of dementia patients and analyzed the predictors of depressive symptoms. Compared with daughters, the daughters-in-law in our sample reported a marginally higher amount of depressive symptoms. With our data, we were able to replicate previous findings in the literature regarding patient predictors of caregiver well-being. First, the better the patients were able to function daily, the lower the caregivers' depression was. This finding corroborates past research showing that higher daily functioning in patients predicts better mental health in caregivers. 8 In addition, patient's cognitive function did not predict the amount of depressive symptoms, which also follows previous research. 32 This indicates that despite dementia being a cognitive disease, the level of decline in cognitive function does not affect caregiver depression. Finally, more frequent and severe behavioral symptoms in patients predicted greater caregiver distress. This also goes in line with studies demonstrating how patients' behavioral symptoms are closely tied to caregivers' mental health. 8,9,33
Importantly, our data showed that the association between behavioral symptoms and caregiver depression depended on the type of caregiver relationship, which is a novel finding. Although both caregiver groups showed an increase in their depressive symptoms as the frequency and severity of patient behavioral symptoms heightened, the amount of this increase was different. For daughters, the behavioral symptoms of the patient were more strongly associated with caregiver depression levels compared with daughters-in-law.
We also tested whether the association between patients' daily functioning and depressive symptoms differed according to caregiver relationship type. However, this interaction term was not significant in our data. This implies that there is something particular about behavioral symptoms so that they more strongly associate with depression in daughter caregivers compared with daughters-in-law.
Why would behavioral symptoms in patients be more strongly related to the daughter caregivers' depression? Daughter and daughter-in-law caregivers have many similarities. Both groups are women and they are of similar ages. Both are taking care of a relative that is one generation above them. However, one difference between daughter and daughter-in-law caregivers is their emotional bond with the patient. Most daughters would have grown up with the patient and as such have a stronger relational bond. Daughter caregivers have been reported to have higher affection toward the patient compared with daughter-in-law caregivers. 19 Having more feelings of affection may worsen the effects of certain factors on caregiver well-being. 18
Many behavioral symptoms are focused on the patient's emotional well-being, such as depression, anxiety, mania, apathy, impulsiveness, and aggression. These problems may be stressful to a person who has strong attachment to the patient, such as the daughter. Caring about someone who is close and special may increase personal stress from the patient's behavioral symptoms. For example, one study on spouse caregivers found that the closer the couple was, the stronger the association between the patient's cognitive impairment and caregiver's depressive symptoms was. 34 In addition, a parent is not only close but also usually respected and looked up to. 35 For the daughter, it could be difficult to see someone whom she emotionally depended on exhibit behavioral symptoms that demonstrate the person can no longer provide emotional support. In contrast, the daughter-in-law likely has a different/weaker emotional relationship with the patient, which does not lead to heavy psychological strains from behavioral symptoms.
Particularly in the South Korean culture, the relationship between the daughter-in-law and mother-in-law is very complex. It is typical and still expected for the mother-in-law to be involved in the daughter-in-law's life, especially as it relates to household care, child rearing, and holiday traditions. In contrast, the father-in-law has a more distant relationship. This close relationship between the mother-in-law and daughter-in-law can not only be a source of intimacy but also of much conflict. There are many positive and negative aspects that are involved, which often result in an ambivalent attitude of daughters-in-law toward their mothers-in-law. 36 For example, some report being as close as an actual mother and daughter. Others report jealousy from their mother-in-law regarding their husband, and some complain the mother-in-law is manipulative and overcontrolling. Maintaining a healthy distance between each other has been reported to lead to positive experiences. Conflict between the two has been associated with a decrease in well-being in all family members. This relationship is an important societal issue in South Korea, where culture is still heavily influenced by traditional Confucian virtues, but is gradually adopting more individualistic Western values. 37 Our study results demonstrate that the daughter-in-law relationship has different implications for caregiver distress.
Nevertheless, although Confucian values may have led more daughters-in-law to assume the caregiver role in Korea, we presume that our results are largely due to the difference in the emotional bond between the caregiver and the patient. As such, we expect our findings to hold in any culture or country in which the daughter has a stronger bond with the parent compared with the daughter-in-law. In other words, by comparing daughters and daughters-in-law, we are essentially examining relationship quality. Daughters who have not been close to their parents or estranged may even be less impacted by the patient's symptoms compared with daughters-in-law who have a closer relationship with the patient.
More generally, our results suggest that the familial relationship between the caregiver and dementia patient should be considered in interventions such as caregiver education and management of caregiver stress. Our results indicate that in the case of generationally younger female relatives, even though they share many similar outward characteristics, they may vary in the caregiving stressors that can cause depression. Interventions for daughter caregivers would benefit by focusing on the management of both behavioral symptoms and daily functioning of patients, whereas for more relationally distal caregivers such as the daughter-in-law, daily functioning in the patient would be more important to manage. Furthermore, regarding future research, our results imply that for studies on dementia caregiver distress, grouping children and children-in-law will result in missing important differences in the factors that influence distress.
Our findings also have implications for caregiving in general, especially for those caring for close family members. Symptoms of care recipients that affect the caregiver emotionally may have a higher toll on caregivers who share a strong bond with the patient. This is important because it seems paradoxical that a close bond between the caregiver and patient may exacerbate certain negative outcomes, 34,38 especially when other studies suggest that closeness has positive caregiver outcomes. 39,40 Our findings suggest that the association between caregiver–patient closeness and outcomes is more complicated than presumed.
One limitation of our study is that all of our findings are correlational, which does not provide information on directionality and causality of the results. It could be that the depression of the caregivers influences patients' behavioral symptoms and daily functioning, although theoretically this is less likely. 8 In addition, we only compared daughter and daughter-in-law caregivers. A study comparing many different familial relationships would be able to yield a more comprehensive picture as to how relationship types are associated with caregiver depression. Although we assume that the difference between daughters and daughters-in-law is due to the emotional bond/relationship quality, we did not directly assess that construct. Future research would benefit from assessing the emotional bond and testing our explanation.
We also did not find differences in patient gender for caregiver distress. This might be because most of the patients were women (n = 67) rather than men (n = 28). Because of this gender disparity, our results might more accurately represent the difference in relationships between daughters, daughters-in-law, mothers, and mothers-in-law. Future studies might focus on collecting data from male patients to further investigate the relationship between daughters, fathers, daughters-in-law, and fathers-in-law.
Conclusions
Caregiver depression is a serious issue of which awareness is increasing. 41 Interventions target on educating caregivers and helping them manage their stress. However, not much research has been done on how predictors of caregiver distress may depend on the relationship between the caregiver and patient. In this study, we found that behavioral symptoms predict greater depressive symptoms in daughter caregivers compared with daughters-in-law. Future studies, which investigate caregiver well-being, and interventions, which aim to promote better caregiver health, would benefit from considering the role of caregiver relationship type.
Footnotes
Acknowledgment
This study was supported by a grant of the Kyujanggak Institute for Korean Studies, Seoul National University, Republic of Korea (09-03-212-13).
Author Disclosure Statement
No competing financial interests exist.