
Abstract
Background:
Ovarian reserve (OR) testing with serum anti-Müllerian hormone (AMH) can provide information about a woman's fertility potential. The aim of this study was to assess interest and knowledge about OR testing and investigate the utility of measuring AMH in women of reproductive age deferring pregnancy.
Methods:
Women ages 27–37 years currently delaying childbearing were invited to take a survey regarding attitudes and knowledge about OR testing before and after an AMH measurement with explanation of their results.
Results:
Of 121 women who took the pre-test survey, 96% believed OR testing was beneficial. The median AMH of the 97 women who underwent testing was 3.3 ng/mL (IQR 1.9–5.4 ng/mL). Nineteen percent of women had AMH <10th percentile for age and 3% had an undetectable AMH. Although 83% of these women were using hormonal contraception, none had known risk factors for diminished ovarian reserve. Seventy-eight percent of women with low AMH levels for age planned to seek fertility preservation or pregnancy, while those with AMH levels within established age normograms were reassured. On the post-test survey, 100% reported benefit in knowing their AMH level. Follow-up testing, 6–8 months after the initial measurement, showed stable AMH levels for most participants.
Conclusions:
Women are interested in OR testing. Most women will be reassured by knowing their AMH level, whereas those with a lower AMH can be counseled on fertility preservation options or may attempt pregnancy earlier.
Introduction
S
AMH is a glycoprotein produced by granulosa cells and it reflects the activity of early growing follicles up to the small antral stage. 2 AMH has been found to be an accurate measure of OR, 3 especially when used in conjunction with antral follicle count (AFC). While there may be small variations throughout the menstrual cycle, 4 it is widely accepted that an individual's AMH level is relatively constant throughout the menstrual cycle and can be measured on any cycle day. AMH may be impacted by hormonal contraceptive use, with studies finding minimal to up to 50% decreases in AMH levels during use. 5 –8 Continuous suppression or shorter hormone-free intervals are associated with more significant decreases in AMH, given the higher inhibition of small antral follicles. 6 Similarly, pregnancy leads to a transient decrease in AMH, with return to baseline value after delivery. 9,10 Smoking has been found to negatively impact AMH values, while factors such as alcohol use, exercise, and socioeconomic status are not thought to be associated with AMH levels. 5 Body mass index (BMI) has not been found to directly correlate with AMH in the general population but may be associated with lower AMH levels in those with DOR or polycystic ovary syndrome. 11,12
Currently, the American College of Obstetricians and Gynecologists Committee Opinion on OR testing acknowledges that AMH is a “useful screening test in women at high risk of DOR and in women undergoing IVF but has limited benefits in someone at low risk of DOR.” 13 While DOR can be a result of age, smoking, and certain personal and family medical risk factors, DOR is often idiopathic. In addition, defining DOR in different age groups is difficult. While there are published normograms of AMH values 14,15 and AFC, 16 most of these data come from the infertile population. The data available from the presumed “healthy” population are limited and can be difficult to interpret, as there is often no outcome data to assist in interpretation. 17,18 While there have been attempts to predict the natural decrease in AMH as a woman ages, 19 the conflicting data regarding the relationship between decreased AMH and earlier menopause suggest that the rate of decline varies and some women may have a lower but stable AMH for longer periods of time. 20 –22
The possibility of using AMH as a screening test for the general population has been raised, especially given the increasing age of women desiring pregnancy. As OR tests such as AMH can be predictive of fertility potential, they may be useful in the general population to identify women at risk for DOR who are otherwise asymptomatic. Once identified, these women may elect to take action earlier or at least seek out more information regarding their fertility status. A recent analysis of OR screening looking at both ethical and scientific arguments suggests that OR testing should be offered to women and proposes an algorithm for offering such screening. 1
The objectives of our study were as follows: (1) to assess interest and knowledge about OR testing in reproductive age women deferring pregnancy with an online survey; (2) to determine if an AMH level and counseling for women not currently attempting pregnancy can impact reproductive and career decisions such as fertility preservation, timing of pregnancy, and career pace; and (3) to determine if an AMH level can assist in identifying DOR in asymptomatic women without personal or family risk factors. We hypothesized that women would be interested in OR testing and would use their AMH level to make life decisions, especially if a low AMH level was detected.
Materials and Methods
Women ages 27–37 years (years) were invited to participate in the Level Study, a study to assess knowledge and attitudes about OR testing in women currently deferring pregnancy, as well as determine serum AMH for participants interested in further testing. Women were recruited to enroll in the Level Study via alumni listservers, social media, and flyers in gynecology offices from October 2014 to March 2015. Pregnant women, women attempting pregnancy, and women being treated by a Reproductive Endocrinology and Infertility specialist were excluded. Interested women were directed to the Level website (
Following survey completion, participants were invited to take a free AMH blood test. During the office visit, written informed consent was obtained and intake data, including demographic, medical history, and family history information, were recorded. From October 2014 to April 2015, AMH testing was performed in 97 women, accounting for 79% of survey participants.
Serum AMH concentrations were measured with the AMH Gen II enzyme-linked immunosorbent assay (Beckman Coulter) according to the manufacturer's specifications. Inter-assay and intra-assay coefficients of variation ranged from 3% to 13% and from 3% to 11%, respectively. AMH of 0.17 ng/mL was the lowest level detectable by the assay. Results were released through password-protected accounts on the Level website and included a basic explanation of how to interpret AMH results. Each participant's AMH value was compared to women of the same age (below average, within normal range, or above average) and placed in the context of egg freezing success, specifically, the likelihood of response to stimulation. Average AMH was defined as 50th percentile for age ±0.25 ng/mL in accordance with AMH normograms for presumably healthy women of reproductive age. 18 All participants were offered a physician consultation by phone to further discuss their results. Participants with AMH values <10th percentile for their age 18 were offered repeat AMH testing and a transvaginal ultrasound to assess AFC, which was defined as the number of antral follicles between 2 and 10 mm in both ovaries. The repeat AMH test and transvaginal ultrasound were free of charge. The combined AFC and confirmed AMH levels were discussed with a focus on the potential impact of hormonal contraceptive use on OR testing. 8
After receiving their AMH results, participants were encouraged to take a post-test survey that assessed the attitudes and actions they planned to take. Sixty-four percent of participants completed the post-test survey (Supplementary Data, Survey 2). A 6-month follow-up AMH measurement was offered free of charge and 49% of participants completed AMH testing within 6–8 months of their initial test. At the follow-up AMH test, the patient's history was reviewed for any changes in contraceptive use, body weight, and/or medical and social history. If the follow-up AMH was substantially changed from the baseline, a repeat AMH measurement was done for confirmation. All AMH testing costs were covered by Level Health, Inc.
Nonparametric statistical analyses, including Mann–Whitney U tests for numerical variables and two-sided Fisher exact tests for categorical variables, were completed using SAS 9.4 Software (SAS Institute, Inc.). Statistical significance was defined as p < 0.05.
Results
Pre-test survey
The median age of women who took the survey was 31.5 (IQR 29–34) years. Most were white (66%), had no children (99%), held a master's or higher degree (64%), and identified themselves as not religious (74%) and politically liberal (65%) (Supplementary Table S1). The majority of participants were in relationships (23% spouse, 36% partner) and using hormonal contraception (56%).
On the pre-test survey, 45% reported knowledge of OR testing. Although 99% would want access to testing and 96% agreed that there was benefit to knowing about their OR, only 36% had spoken to a doctor about fertility in the last 2 years. Women who had discussed fertility (36%) and those who had not (64%) were of similar ages [33 (IQR 31–35) vs. 31 (IQR 29–33) years, p = 0.19]. Of those who had spoken with a doctor, the 39% who were “told to do something soon” were significantly older than 52% who were “told not to worry as there was still time” [35 (IQR 34–36) vs. 31 (IQR 29–32) years, p = 0.001]. The most common reasons for not having a conversation about fertility were as follows: (1) the doctor had not initiated the discussion (55%); (2) the participant had not seen a doctor recently (23%); and (3) the participant had not thought much about fertility (21%). When posed the question of what she would do if her AMH level was “low,” most women reported they would take action, with 83% reporting they would have children earlier and consider freezing eggs (83%) or embryos (53%). When asked if she would seek testing if insurance did not cover it, 51% reported that she would pay out-of-pocket.
Before the study, the majority of women knew basic information about OR (Table 1), including the approximate age when fertility declines; that women are born with all of their eggs; smoking reduces OR; and that birth control pills do not preserve fertility. There were some misconceptions, however, including the belief that OR testing gives information about egg quality (76%) and the likelihood of future pregnancy success (50%), and that egg freezing (74%) or IVF (81%) ensures pregnancy.
OR, ovarian reserve.
AMH testing
The median AMH was 3.3 (IQR 1.9–5.4, range <0.17–18.4) ng/mL (Fig. 1). The majority of participants who tested (64%) were using hormonal contraception. Twenty-five percent reported smoking at some time, although only 2% reported current social smoking. No women reported a confirmed endometriosis diagnosis, although one woman had a history of a unilateral oophorectomy due to a large ovarian cyst. Nine percent reported personal history of autoimmune disease, including thyroid disorders and alopecia, while 19% reported family history of autoimmune diseases, including thyroid disorders and rheumatoid arthritis or a maternal menopause age of <40 years. In terms of a potentially increased AMH, three women reported having been diagnosed with polycystic ovary syndrome.
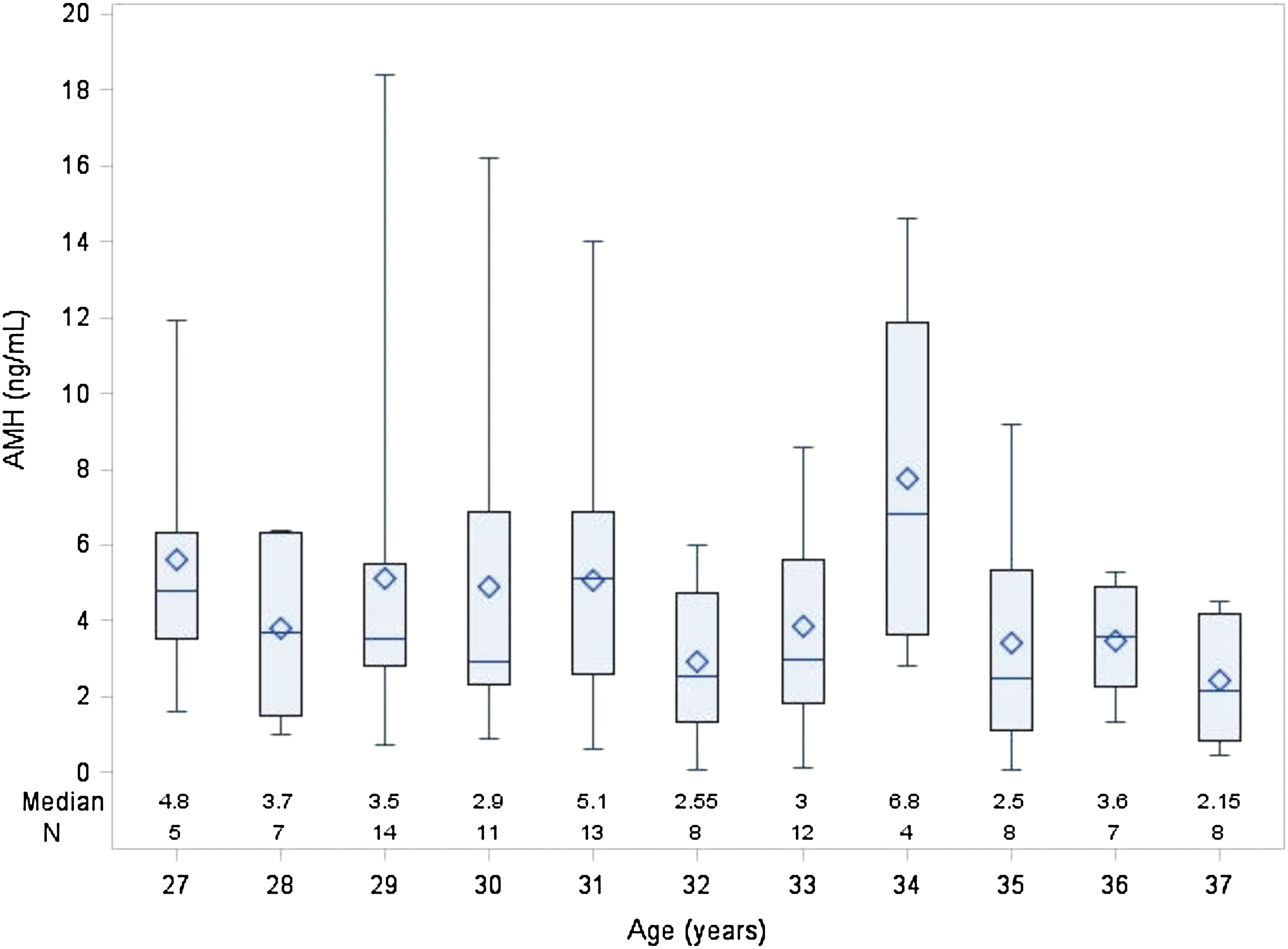
AMH levels by age. Median AMH values and interquartile ranges at each age from 27 to 37 years are presented. Median AMH decreased with age. N = number of participants. AMH, anti-Müllerian hormone.
Of participants, 19% had AMH levels <10th percentile for their age (median 0.88, IQR 0.61–1.06, range <0.17–1.37 ng/mL); three women had undetectable AMH levels (<0.17 ng/mL). On repeat testing, performed within 8 weeks to confirm low AMH levels, 12/13 still had AMH <10th percentile based on normograms published by Shebl et al. 18 The median change in AMH was 0.14 (IQR −0.21 to 0.23, range −0.65 to 0.66) ng/mL. AFC performed on 11/18 women revealed median AFC 8 (IQR 6.5–10, range 2–14) follicles, with 7/11 women having a lower than the expected AFC for their age based on published normograms. 16
We compared participants with AMH <10th and AMH ≥10th percentile for age (Table 2). There was no difference in age, current or past smoking, history of autoimmune disease, or family history of autoimmune disease/early menopause in these two groups. However, there was a significantly higher BMI in the low AMH group. The difference in hormonal contraceptive use between these groups was not statistically significant. Post-testing, 10/18 women scheduled appointments with an infertility specialist and 14/18 said they will either attempt pregnancy or freeze their eggs in the upcoming year (Supplementary Table S2). None of the 18 participants had planned to do oocyte harvesting and freezing or attempt pregnancy before receiving their AMH results.
Statistical significance with p < 0.05.
Reported medical history that may impact OR included history of unilateral oophorectomy (n = 1), autoimmune disorders (n = 8; thyroid disorder (n = 7), and alopecia (n = 1).
Reported family history that may impact OR included history of early maternal menopause (n = 3), autoimmune disorders (n = 15; thyroid disorders (n = 14), and rheumatoid arthritis (n = 1).
AMH, anti-Müllerian hormone; BMI, body mass index; IQR, interquartile range.
Post-test survey
On the post-test survey, 100% reported benefit from knowing their AMH levels, with 97% reporting the results were helpful and 65% wanting to receive another AMH test in the future. In comparing actions women had considered before receiving their AMH result to actions they planned to take after AMH testing, most women were reassured by knowing their AMH levels (Table 3). Participants were less likely to feel pressure to have children (34%), freeze eggs (40%) or embryos (27%), or change their career pace (66%) at this time compared to the actions they reported before the AMH test.
Statistical significance with p < 0.05.
Follow-up AMH testing
Of 97 participants, 49% returned for follow-up AMH testing 6–8 months after their initial AMH test. Most women had similar AMH levels compared to their baseline AMH, with a median change in AMH of 0.005 (IQR −1.05 to 0.53, range −5.1 to 5.2) ng/mL (Supplementary Figure S1). Fifteen women had a change of >2 ng/mL, although 13/15 of these women had an elevated AMH ≥4.7 ng/mL at baseline, which is suggestive of polycystic ovary syndrome. 23 Of the 9/13 women with an initially high AMH that decreased, none had a follow-up AMH value that was considered low for her age. 18
Half of the participants (9/18) with AMH <10th percentile for their age presented for follow-up testing and had a median change in AMH of 0.31 (IQR 0–0.7, range −0.1 to 3.25) ng/mL compared to their baseline. Interestingly, one woman with an AMH of 1.05 ng/mL while on continuous oral contraception had an AMH of 4.3 ng/mL after she switched to an intrauterine device for contraception. Her AMH values were repeated for confirmation.
Discussion
This study found that women are interested in OR testing and will use their results for future reproductive planning. Furthermore, we found 19% of asymptomatic women were at risk for DOR. Taken together, these data support previous articles advocating for expanding the use of AMH testing. 1,22,24,25
Prior studies have demonstrated interest in assessing current OR. Bavan et al. performed a study among female university students with a mean age of 22 years and found that 79% were interested in knowing their OR. 26 Azhar et al. surveyed both female and male health providers with a median age of 29 years regarding OR testing for themselves or their partners and found similar interest. 27 In both studies, participants were asked what they would do if they had a theoretical “low” OR. Our study adds to the literature in that we assessed attitudes and interest as well as measured AMH as a marker of OR. Thus, we compared a theoretical action to the actual or planned action. Most participants in our study were reassured by their AMH results, with significant decreases in the number of women who said they would have children earlier, freeze eggs or embryos, or change their career pace.
Despite the interest in OR testing and the important impact testing may have on a woman's reproductive planning, our results suggest that many doctors do not talk about fertility. In our study, only 36% of participants reported speaking to a doctor about fertility in the past 2 years, with the most common reason for not having a conversation about fertility being that the doctor had not initiated the discussion. With increasing delay in childbearing and misleading portrayal of fertility potential in the media, discussions of fertility by doctors are critical. Some general obstetrician gynecologists have begun to offer AMH testing. We suggest that generalists who may not feel comfortable testing for and interpreting AMH levels should start a discussion about female fertility and offer referrals to those women who are interested in learning more.
The interpretation of AMH levels and counseling in the context of women not currently attempting pregnancy are critical as an AMH value can be impacted by various factors. 25 A practitioner must know the “normal” values for the patient's age and history and for the specific AMH assay that is used so that appropriate counseling can be offered that does not lead to undue anxiety or false reassurance. In addition, blood for AMH measurement must be collected and processed correctly as conditions such as hemolysis and temperature impact results. 28,29 As hormonal contraception can suppress the AMH levels, 6,8 this becomes an important part of the conversation for women with lower than expected AMH values. 8 In those with low AMH, the possibility of switching to a nonhormonal contraceptive method and then repeating an AMH level in a few months may be considered. In addition, long-term decreases in AMH over time are still being studied. In women who completed a 6- to 8-month follow-up AMH in our study, most had stable values, including those with low AMH values. Thus, patients with lower values must be counseled that while reproductive life span may be decreased, the time course is unknown.
In our study, 19% of participants had AMH levels <10th percentile for their age and 3% had undetectable AMH, with levels validated by repeating the AMH test within 8 weeks. We recognize that as 83% of women in this subset of women were using hormonal contraception, some may not actually have AMH levels <10th percentile for their age when off hormonal contraception. However, the difference in hormonal contraceptive use between this subset and the whole cohort was not statistically significant, and so, this factor alone does not likely explain the low AMH levels in users. In addition, the low AMH levels were consistent with low AFC findings, except for the one woman on continuous oral contraception previously discussed. When compared to the whole cohort, this subset of women had no increased risk factors for DOR such as age, personal or family medical history, or smoking history. This subset of women did have a higher median BMI, which may also support a potential DOR diagnosis as other studies have found increased BMI associated with decreased AMH levels in women with DOR or infertility but not in the general population with normal OR. None of the women had considered oocyte freezing or attempting pregnancy before receiving their AMH results. After testing and counseling, 78% planned to take immediate action and an additional 17% planned to take action if AMH significantly decreased within the year. These findings support the use of AMH as a screening test for DOR and are in concert with previous literature advocating for such use. 1
There are limitations to this study. There is potential for bias in the views and actions of the women in our small sample size. Many were self-recruited from professional and alumni listservers, which is reflected in their relatively similar demographics and suggests they may have previously considered OR testing. While these data may not be generalizable to the reproductive population at large, we believe that our findings represent the attitudes and beliefs of many professional women who often delay childbearing longer for career opportunities. In addition, as this study offered free testing, the women who chose to participate may be different than those who would seek OR testing if there was a cost associated with testing. There was some loss to follow-up in completing the post-test survey, and so, there is a potential for bias. However, we personally contacted women with low AMH values to ensure we had complete information on their plans. Also, while our laboratory runs quality control samples and low AMH samples were repeated in this study, there could be differences in the number of women reported to have a low AMH for their age in our study if samples were run in other laboratories or using different assays. Also, as previously stated, given the high percentage of women on hormonal contraception, the number of women with values truly <10th percentile for their age may be overstated if hormonal contraception was partially responsible for lower AMH values. The three women with undetectable AMH levels, however, would not likely be impacted by differences between laboratories and assays or hormonal contraception. A larger study with longer follow-up will add to the data on this important topic.
Conclusions
As women continue to defer childbearing until later ages, OR screening with AMH can assist women in making reproductive decisions. Proper counseling on the meaning of AMH for current OR and future fertility is an essential component of AMH testing. Based on our findings, most women will be reassured by knowing their AMH levels and the increased knowledge and education may assist with future reproductive and career planning. Asymptomatic women without risk factors who may be identified as having AMH <10th percentile for age, and those women with an undetectable AMH, can be further evaluated, counseled, and educated on fertility options, likely leading to more reproductive success.
Footnotes
Acknowledgments
The authors thank Kimberly Hamroff, MS (Special Research Scientist, Columbia University Medical Center), Nancy Cotui (Lab Supervisor, Columbia University Medical Center), and Michel Ferin, MD (Lab Director and Professor of Physiology and Cellular Biophysics, Columbia University Medical Center), for their technical assistance with the AMH assays and insightful discussions. The authors thank Tammy Hepps (Chief Technology Officer, Level Health, Inc.) for her assistance with the online surveys and website development and insightful discussions.
Author Disclosure Statement
This work was supported by Level Health, Inc. C.W.C. is CEO of Level Health, Inc. No conflicts of interest exist for any of the other authors.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.