
Abstract
Objective:
This two-part study analyzed data collected from middle-aged (age 44–64) and older women (age 65+) with one or more chronic conditions who completed the National Council on Aging Chronic Care Survey.
Materials and Methods:
Part One analyzed data from 418 women to describe sociodemographics, disease types, and healthcare utilization associated with Internet use among middle-aged and older women with 1 or more chronic diseases. Part Two analyzed data from the 251 Internet-using women to identify the online self-care resources they are using (format, host organization) and for what purposes.
Results:
Approximately 31% of participants were age 65 years or older, 30% reported having three or more chronic condition types, and 65% reported using the Internet. A significantly larger proportion of older women reported multiple chronic conditions, and a significantly fewer number of older women reported using the Internet. A significantly smaller proportion of Internet users were non-Hispanic white, more educated, and employed. A significantly larger proportion of non-Internet users reported needing help learning what to do to manage their health conditions and needing help learning how to care for their health conditions. Among only Internet-using women, 18.7% participated in online discussions/chatrooms/listserv and 45.2% read about the experiences of others with chronic diseases. Interest in websites and online courses varied.
Conclusion:
Understanding Internet use among women with chronic conditions can inform targeted efforts to increase Internet availability, educate potential users about the benefits of online resources, and effectively tailor Internet-based materials to self-care needs.
Introduction
T
Self-care behaviors are important in managing chronic disease and in optimizing health, because self-care can increase self-efficacy, satisfaction, and overall quality of life. 7 Self-care behaviors draw on one's physical, social, and healthcare environments to compensate for, or delay, physical limitations and chronic conditions from progressing into more severe disabilities. However, the effects of living with one or more chronic conditions can diminish not only an individual's capacity to adequately care for themselves but also a caregiver's ability to serve as a sufficient resource. 8
As individuals are increasingly playing a larger role in managing their own health, the Internet is and will continue to be utilized as a major source of health information. 9,10 Internet-based resources can help individuals with chronic diseases to share their experiences and gather information, and they may help people to overcome traditional barriers to self-care. 11,12 Greater engagement in Internet and social media may be associated with improvements in health behaviors and health status, 13 which suggest that the Internet is an increasingly important component in health maintenance.
The Internet may especially benefit older adults seeking health information, given that they are more likely than non-elderly populations to be complex patients with aging-related health declines and other preventable morbid conditions. 14 However, older adults are less likely than their younger counterparts to utilize Internet resources to improve self-care behaviors or efficacy. 15 Research indicates that older patients rely more heavily on their healthcare providers for information than non-elderly populations, 14,16 while appearing reluctant to rely solely or heavily on the Internet for health information [and may not deem the Internet a credible, reliable, or easy-to-navigate resource]. Less Internet use among older adults for health information and self-care purposes may reflect a lack of familiarity or comfort with technology in general. 17
Women may also particularly benefit from seeking health information from the Internet, because they are more likely than men to be living with chronic disease. 6,7 Gender differences in Internet use 18 include women utilizing social networking sites more often than men, 19 and women having higher quality perceptions of eHealth searching and information dissemination compared with men. 20 We maintain that women are not only more likely to conduct e-health information searches than their male counterparts but also more interested in health-related issues overall. 16,20,21
Despite the promise of the Internet as an additional resource for current and future cohorts of women with chronic disease, 22,23 little is known about Internet use patterns among middle-aged and older women or on their preferences for Internet-based self-care resources to improve their efficacy or quality of life. In response to these gaps in the literature, the current study describes the sociodemographic characteristics, types of disease, and healthcare utilization associated with Internet use among middle-aged and older women with chronic conditions (Aim 1). Among Internet-using women, we further identify the online self-care resources most used and for what purposes (Aim 2) (Fig. 1).
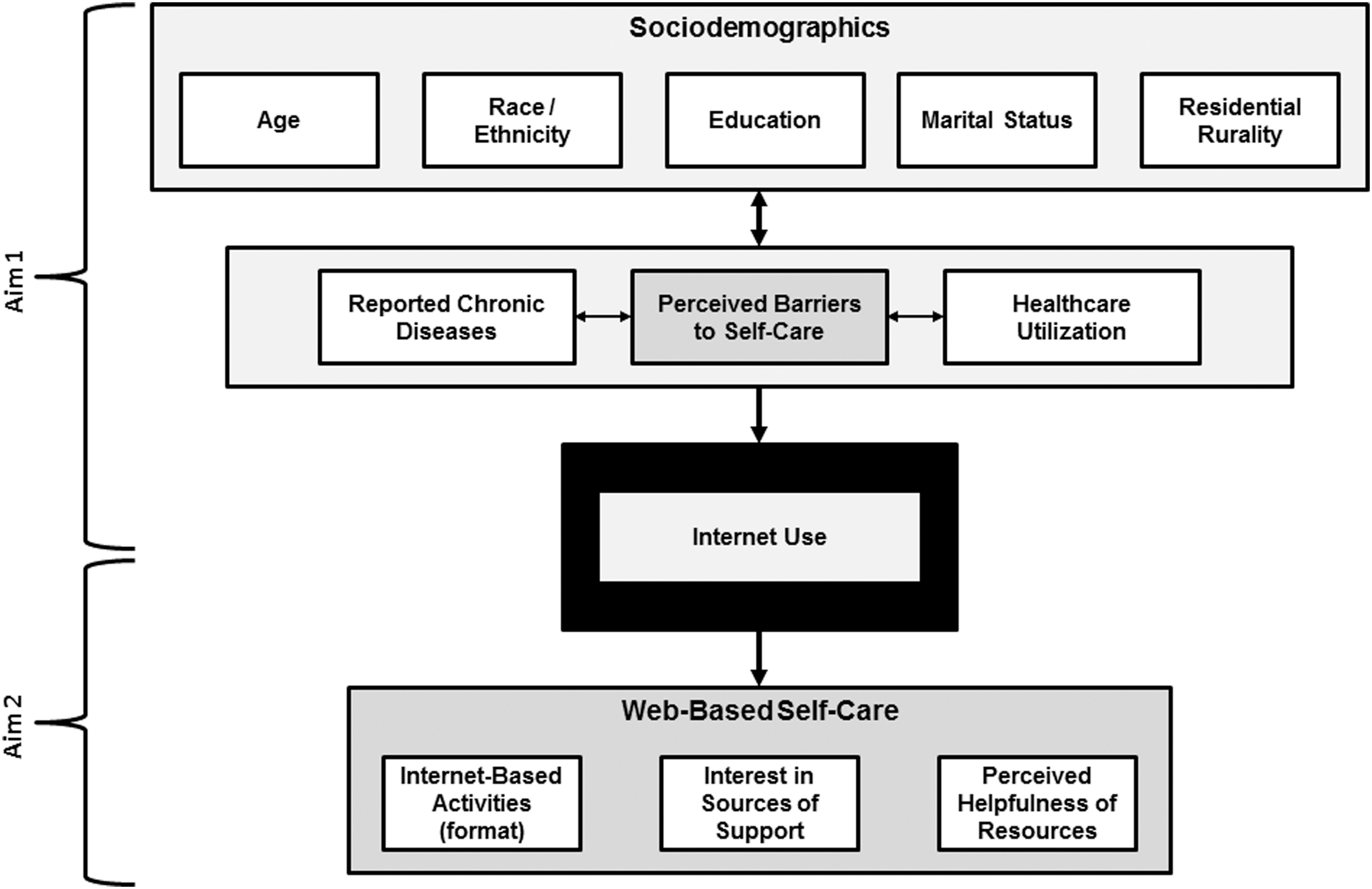
Conceptual model illustrating factors associated with Internet use and web-based self-care.
Materials and Methods
Study data
Study data are from the National Council on Aging (NCOA) Chronic Care Survey (CCS), which is a nationally representative probability survey of Americans 44 years and older with chronic conditions conducted by Lake Research Partners. 24,25 The survey employed telephone-based interviews to collect data by using random digit dialing (RDD) sampling techniques. Telephone interviews were conducted in both English and Spanish.
To be eligible for inclusion in the NCOA CCS, participants had to be 44 years of age or older, and report having at least one chronic condition at the time of the study. Participants were screened for chronic condition(s) with the following question(s): “Have you ever been told by a doctor, nurse or other health professional that you have [name of chronic condition]?” Chronic conditions in the screening process included: heart disease, cancer, stroke, diabetes, arthritis, asthma, hypertension or high blood pressure, emphysema, chronic bronchitis, depression, and anxiety. Only participants who reported “yes” to at least one of these items were included in the survey. 25
Study sample
A total of 960 community-dwelling men and women aged 44 years and older with at least one chronic condition across the United States were surveyed, with oversampling of those 65 years and older and Hispanics. Details about data weighting are reported elsewhere. 24 The survey included respondent information for 427 women (44.5% of the full sample). Based on the aims of this study, the sample of women was analyzed in two ways. The first analysis had 418 complete cases of women aged 44 years and older, which was used for Aim 1 of the study. The second analysis involved a sub-sample of 251 Internet-using women 44 years and older, which was used for Aim 2 of the study.
Data and measures
Sociodemographics
To identify personal characteristics of these women, sociodemographic variables in this study included: age group, race/ethnicity, education level, marital status, residential rurality, and work status.
Self-reported chronic conditions
Participants were asked to self-report their diagnosed chronic diseases from a list of 12 conditions. These categories were collapsed into six chronic condition types, including cardiovascular disease, diabetes, arthritis, lung disease, depression, and cancer. The number of endorsed disease types was also summed to create a continuous variable of the number of chronic conditions and then collapsed into three groups: 1, 2, or 3+ chronic diseases.
Self-care barriers
Participants were asked to self-report their perceived barriers to self-care by using two items. Participants were asked to rate their level of agreement with the following two statements: “I need help learning what I should be doing to take better care of my health;” and “I need help learning how to take better care of my health in a way that works for me and my life.” For both items, responses were scored on a 5-point Likert-type scale ranging from “strongly disagree” to “strongly agree.” Based on the frequency distribution, participant responses were then dichotomized into two categories: “disagree” and “agree.”
Internet use
Participants were asked to self-report their Internet use. Participants were asked: “How often do you use the internet?” Responses were scored on a 4-point Likert-type scale with categories of “never,” “rarely,” “sometimes,” and “frequently.” Responses for this variable were reported by using these four categories for Aim 1, and they were also dichotomized into “never” versus “rarely/sometimes/frequently” for Aim 2.
General health-related support perceptions
Participants were asked to self-report their perceptions about receiving general support to manage their health problems and their reliance on the Internet for such purposes. Participants were asked: “How often do you feel you get the help and support you need to improve your health and manage your health problems?” Responses were scored by using a 5-point Likert-type scale of “never,” “rarely,” “occasionally,” “frequently,” and “always.” Participants were also asked: “How much do you rely on the internet for ongoing help and support with your health problems?” Responses were scored on a 4-point Likert-type scale with categories of “not at all,” “a little,” “some,” and “a lot.”
Internet-related activities
Internet-using participants were asked to report their participation in certain online activities. Participants were asked to respond to two questions: “Do you ever use the internet to read or participate in an online discussion, chatroom, a listserv, or other online forum about your health problems?” “Do you ever use the internet to read about someone's experiences with health problems like yours, on an online news group, website or blog?” Response categories for both items were “no” and “yes.”
Internet-related interests
Internet-using participants were asked to report their level of interest in getting information and support from various sources by using three questions: “How interested would you be in getting information and support from…” (1) websites sponsored by health organizations?, (2) websites sponsored by the government?, and (3) Internet-based courses or discussion groups? For these items, responses were scored on a 4-point Likert-type scale of “not at all interested,” “not interested,” “interested,” and “very interested.”
Perceptions about helpful resources
Internet-using participants were asked to report their perceptions about things that might help them manage their health problems and improve their health by responding to four statements: “How helpful would it be for you to…” (1) get practical tips and advice from other people who have health problems similar to yours?, (2) learn how to exercise or eat better in a way that is realistic and works with your limitations?, (3) set goals and work together with other people who are trying to improve their health?, and (4) learn how to manage work, family, and other responsibilities and still take care of your health? For these items, responses were scored on a 4-point Likert-type scale of “not at all helpful,” “not helpful,” “helpful,” and “very helpful.”
Health status indicators
Participants were asked to self-report aspects of their current health status by using items intended to measure activity limitations, the number of prescription medications taken each day, and the number of physician visits in the previous 12 months. Self-reported health was scored on a 5-point Likert-type scale of “poor,” “fair,” “good,” “very good,” and “excellent.” Participants were asked: “Are you limited in any way in any activities because of physical, mental, or emotional problems?” Responses were scored as “no” or “yes.” Participants were asked: “How many different prescription medications do you regularly take each day?” Responses ranged from 0 to 26 for this open-ended item. Participants were also asked: “In the past 12 months, how many times have you, yourself made a doctor's visit?” Responses ranged from 0 to 10 for this open-ended item.
Data analysis
Statistical analyses for this study were performed by using SPSS (version 22). In Aim 1, frequencies were calculated for all study variables, which were initially examined by age group, number of chronic conditions, and Internet use. Pearson's chi-square tests were performed to assess the distribution of cases across response choices in each dependent variable for categorical independent variables. Independent sample t-tests and one-way analysis of variance (ANOVA) were used to examine mean differences for continuous variables based on age group, number of chronic conditions, and Internet use. In Aim 2, frequencies were calculated for Internet-related variables among Internet-using women, which were examined in relationship to respondents' age group (i.e., 44–64 years and 65+ years) and number of chronic conditions (i.e., 1, 2, or 3+). Again, Pearson's chi-square tests were performed to assess the distribution of cases across response categories for the dependent variables and for categorical independent variables.
Results
Sample
Sample characteristics of study participants are presented in Table 1. Of the 418 women participating in this study, 30.6% were 65 years and older, 58.3% had 2 or more chronic conditions (30.3% had 3+ chronic conditions), and 65.1% reported using the Internet. Respondents were disproportionately non-Hispanic white (83.5%), married (60.3%), and had an education level of some college or more (53.7%). Thirty-seven percent of participants were employed, 36.0% were retired, 14.1% were unemployed, and 12.9% were disabled. Approximately 30% of participants reported being limited from activities because of physical, mental, or emotional problems. On average, participants reported taking 3.31 medications daily and visiting a physician 3.12 times in the previous 12 months. The majority of participants reported their health as good or very good (65.1%) and that they frequently or always received help and support to manage their health problems (60.4%). Approximately 28% of participants reported needing help learning what to do to manage their health conditions, and 33.9% reported needing help learning how to better care for their health.
p < 0.05; ** p < 0.01; *** p < 0.001.
Compared with women aged 44–64 years (i.e., “younger”), significantly more women 65 years and older (i.e., “older”) were unmarried and retired, had cardiovascular disease and arthritis. On average, older women reported taking more medications daily compared with younger women. Older women were significantly more likely to receive help and support needed to manage their health problems, yet less likely to use the Internet.
Having more chronic conditions was significantly associated with having lower education levels and being unmarried. Women with more chronic conditions reported greater activity limitations and worse general health status. Women with more chronic conditions were more likely to report needing help learning what to do to manage their health conditions and how to better care for their health, yet less likely to have used the Internet.
When comparing participants based on Internet use, a significantly larger proportion of non-Internet users were older, non-white, lesser educated, married, and retired. On average, non-Internet using women had more chronic condition types, especially cardiovascular disease and arthritis. Larger proportions of non-Internet using women reported activity limitations and worse general health status. Larger proportions of non-Internet using women reported needing help learning what to do to manage their health conditions and help learning how to better care for their health.
Internet-using women
Internet-related characteristics of Internet-using study participants are presented in Table 2. Of the 251 women, 19.1% were aged 65 years and older and 50.6% had 2 or more chronic conditions (25.5% had 3+ chronic conditions). More than 70% of participants reported using the Internet frequently. Less than 20% of participants reported participating in online discussions, chatrooms, or listerv, whereas nearly half reported reading about others' experiences online. Women expressed interest in getting information and support primarily from health organization websites, followed by government websites and online courses or discussion groups. Women reported that getting emotional support from people with similar problems might help them manage their health problems and improve their health, followed by learning how to exercise or eat better, getting practical tips from others with the same problems, setting goals and working with others trying to improve their health, and learning how to manage responsibilities and still take care of their health.
p < 0.05; ** p < 0.01; *** p < 0.001.
When comparing Internet-related characteristics by age group, a significantly smaller proportion of older women relied on the Internet for help or support. A smaller proportion of older women participated in online discussions, chatrooms, or listerv and read about others' experiences online. Compared with younger women, a smaller proportion of older women reported that setting goals and working with others to try to improve their health and learning how to manage responsibilities while still taking care of their health was helpful. When comparing Internet-related characteristics based on the number of chronic conditions, having more chronic conditions was associated with less reliance on the Internet for help or support. Smaller proportions of women with more chronic conditions reported that getting practical tips from others with the same problems and learning how to manage responsibilities and still take care of their health was helpful.
Internet-related characteristics of Internet-using study participants by chronic condition type are presented in Appendix Table A1. Larger proportions of women with diabetes and depression reported needing help learning what to do to manage their health conditions, whereas a smaller proportion of women with lung disease reported this self-care barrier. Similarly, larger proportions of women with diabetes and depression reported needing help learning how to better care for their health, whereas a smaller proportion of women with cancer reported this self-care barrier. A larger proportion of women with depression reported relying on the Internet for help or support; whereas smaller proportions of women with cardiovascular disease and arthritis reported this type of reliance. A larger proportion of women with depression read about others' experiences online, whereas a smaller proportion of women with arthritis reported reading about others' experiences. A smaller proportion of women with arthritis reported interest in online courses or discussion groups. A smaller proportion of women with cardiovascular disease reported getting practical tips from others with the same problems or learning how to manage responsibilities and still take care of their health as helpful.
Discussion
This study examined how middle-aged and older women living with one or more chronic diseases use the Internet and online resources to manage their conditions. This study confirmed previous studies reporting that older adults use the Internet less than their younger counterparts. 7,26 It further confirmed that individuals who were less educated, more isolated and those who described themselves as belonging to a minority group utilized the Internet less than other subpopulations. 27 These findings confirm the gap between resources available and the variables that keep older populations from utilizing such resources.
As Stellefson et al. 13 report, greater Internet engagement may lead to improvements in both health status and health behaviors for this population. There is a need for more evidence-based online resources that can assist with disease self-management, self-care, and social satisfaction. 23,28 –30 Although research investigating the planning, implementation, and overall evaluation of web chronic disease self-management programs for this specific population do not currently exist, several studies suggest that it is possible and pertinent to reach middle-aged and older populations with Internet-based interventions—even among those of “poor health” or who report that they possess “limited or no computer experience.” 13,27
We discovered that a significantly larger proportion of Internet-using women with diabetes and depression reported needing help in both learning what to do online to manage their health conditions and how to use available web resources, compared with women with other health conditions. This finding highlights the notion that Internet resources may vary among diverse diseases and comorbidities. Incorporating disease type and comorbidity characteristics in future research can lead to a better understanding of how web utilization can assist in disease self-management and self-care and why specific diseases and comorbidities may lead to more resistance to web interaction.
Next steps include equipping healthcare providers with an awareness of the benefits of patients accessing and utilizing web-based resources for health information. Further, ensuring that providers can relay critical guidance on where to look and how to access evidence and web-based resources is a critical step if providers are to effectively facilitate patients' use of web-based health resources. For example, providing information to a patient in the form of how-to steps (e.g., how to access key websites or how to use key words to search for information) may be effective given that older generations rely heavily on their doctor's recommendations. 10 Fox 7 maintains that healthcare providers should consider making “Do you ever go online for your health information?” a standard procedural question.
Although governmental and medical databases and sites have been deemed helpful in the past, previous research reports that older adults utilize blogs and online health discussion forums more than any other web resource format or activity. 21 Although 4.2% and 26.5% of older adults in the current study reported participating in online discussions/chatrooms/listserv and reading about others' experiences online, respectively, ∼42% of participants reported at least some interest in getting information or support from online courses or discussion groups. Social engagement remains the focus and driver for increasing psychological well-being in older adults. 27 Thus, we suggest more prevalence to online counseling and therapy, increased pervasiveness of easy-to-find online support groups, and tutorials for both blog searches and blog creation and maintenance. Providing the rudimentary training focusing on the possibilities of online resources can provide older women with chronic conditions and a sense of power and control—a higher appreciation for self-efficacy. 31
Future research is needed based on age-related chronic conditions that may differ by one's age cohort and their specific disease. By providing reliable, valuable, and age-appropriate resources and effective training for middle-aged and older women living with one or more chronic conditions, it is possible to increase both disease-self management and quality of life for participants. However, having high-quality resources available is only part of the equation. For those who indicated they did not utilize the Internet, opportunities exist to increase overall access to equipment and training about evidence-based, reliable health sources. According to the American Library Association, all public libraries in the United States offer free Internet on a public computer, whereas 98% of them also offer free wireless access (Wi-Fi) to accommodate various devices such as tablets and smart phones. 32 Librarians also provide assistance in using computers and navigating the Internet. 33 In addition to public libraries, senior centers and community centers generally offer computer and Internet courses, which can make older non-Internet users feel more comfortable seeking health information online. 34,35 Improving Internet access and skills through clinical-community partnerships and referrals to different community-based organizations is the first step to encouraging middle-aged and older women to use online resources to manage their chronic diseases.
For those who indicated current Internet usage, there remains a demand for high-quality online self-care resources and the ability to find and incorporate such resources. We suggest increasing the availability and presence of such effective resources, tailoring the content based on specific disease types or comorbidities, and emphasizing skill building and interaction with healthcare providers.
Ultimately, we must ascertain that older adults with chronic conditions are both able and interested in using recommended web resources and address how best to promote these services. Healthcare professionals can help facilitate such resource retrieval and training. However, by incorporating more social awareness and promotion through senior centers, faith-based organizations, aging councils, and organizations, we can better align future efforts with optimal points of social connection. This link to health and social inclusion may be the best manner for increasing middle-aged and older adults' online utilization and ability to make more social connections, help others through their online presence, and, ultimately, increase their sense of self-worth, well-being, and disease self-management.
Limitations
This secondary dataset did not contain all variables that are necessary to fully contextualize barriers and challenges associated with chronic disease self-care among this aging population. For example, information about therapy adherence and clinical follow-up (as directed by a physician) were not collected from this sample of women. Such data should be collected in future studies to provide additional context about the Internet's role in clinical adherence for disease management and self-care behaviors. However, this dataset contained many variables of interest to address the current research gaps in knowledge about chronic disease management.
Substantial numbers of participants were lost due to incomplete data on particular scale items, resulting in an analytical sample that was systematically different from the full sample (e.g., younger, married, and more white) and potentially limited the generalizability of study findings. The reduction of cases in the analytic sample reduced the potential proportion of older adults in the study from 42.1% to 33.4%, which may especially influence the generalizability of findings to populations aged 65 years and older. Study participants reported a variety of chronic conditions, but sub-analyses based on disease type were not performed because the sample size was inadequate to make such comparisons. Although the descriptive nature of the current study could be seen as a shortcoming, these analyses provide a critical glimpse into the lives of women living with chronic conditions, which can guide future research efforts. We recommend that future studies utilize more sophisticated analytic strategies (e.g., Cochran-Armitage tests for linear trends, multivariate analyses, structural equation modeling) to build on the findings reported here. Recognizing that needed self-care behaviors may differ based on women's particular condition diagnoses, disease stage, and the number of comorbidities with which they are diagnosed, future studies should strive to compare barriers with self-care, perceived physician support, and frustrations with the healthcare system by their chronic condition profile. Further, because women's ability to cope with and adjust to their disease self-care may differ based on their available resources and socioeconomic status, future studies should examine such variables to determine their relationship with self-care disparities.
Another study limitation reducing the ability to widely generalize findings to the greater female community was the self-report and cross-sectional nature of the data. However, the sample was derived from RDD and included items that deeply explore the challenges and frustrations with chronic condition self-management, which are not typically seen in other studies that investigate correlations between self-care behaviors and other healthcare or physical health indicators. Thus, this study contributes to a fuller understanding of the complex interrelationships that exist between self-care strategies, provider–patient interactions, and policies/programs in community contexts.
Conclusions
Incorporating the reliance of older adults on their personal healthcare professionals can increase the number of older adults utilizing the Internet and appropriate self-care practices. 13,36 The opportunity to address this lack of utilization is best tailored for older women with one or more chronic conditions. Overall, we maintain that there is a need to address the current gaps and to determine how best to target this specific population and increase evidence-based Internet resources that they can access for disease self-management and self-care practices.
Footnotes
Acknowledgments
This study was made possible by the vast contributions and leadership of the National Council on Aging (NCOA), with support from Atlantic Philanthropies and the California Healthcare Foundation (CHCF). The authors recognize support from the Center for Community Health Development, which is a member of the Prevention Research Centers Program, supported by the Centers for Disease Control and Prevention cooperative agreement number 5 U48 DP000045. The findings and conclusions in this article do not necessarily represent the official position of the Centers for Disease Control and Prevention or the NCOA.
Author Disclosure Statement
No competing financial interests exist.
| Cardiovascular disease | Diabetes | Arthritis | Lung disease | Depression | Cancer | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Total, % (n = 251) | No, % (n = 120) | Yes, % (n = 131) | p | No, % (n = 195) | Yes, % (n = 56) | p | No, % (n = 144) | Yes, % (n = 107) | p | No, % (n = 188) | Yes, % (n = 63) | p | No, % (n = 176) | Yes, % (n = 75) | p | No, % (n = 213) | Yes, % (n = 38) | p | |
| I need help learning what to do (to manage my conditions) | |||||||||||||||||||
| Disagree | 76.5 | 80.0 | 73.3 | 80.0 | 64.3 | * | 75.0 | 78.5 | 72.9 | 87.3 | * | 80.7 | 66.7 | * | 75.0 | 84.6 | |||
| Agree | 23.5 | 20.0 | 26.7 | 20.0 | 35.7 | 25.0 | 21.5 | 27.1 | 12.7 | 19.3 | 33.3 | 25.0 | 15.4 | ||||||
| I need help learning how to take care of myself | |||||||||||||||||||
| Disagree | 69.6 | 72.5 | 66.4 | 74.2 | 53.6 | ** | 69.4 | 70.1 | 68.6 | 71.9 | 77.8 | 50.7 | *** | 66.2 | 86.8 | * | |||
| Agree | 30.4 | 27.5 | 33.6 | 25.8 | 46.4 | 30.6 | 29.9 | 31.4 | 28.1 | 22.2 | 49.3 | 33.8 | 13.2 | ||||||
| Frequency of Internet use | |||||||||||||||||||
| Rarely | 8.8 | 8.3 | 9.9 | 8.8 | 8.9 | 6.9 | 11.2 | 9.6 | 6.3 | 8.5 | 9.3 | 7.5 | 15.8 | ||||||
| Sometimes | 20.0 | 15.8 | 23.7 | 18.0 | 26.8 | 18.8 | 22.4 | 19.7 | 22.2 | 23.3 | 13.3 | 20.7 | 18.4 | ||||||
| Frequently | 71.2 | 75.8 | 66.4 | 73.2 | 64.3 | 74.3 | 66.4 | 70.7 | 71.4 | 68.2 | 77.3 | 71.8 | 65.8 | ||||||
| Rely on Internet for help/support | |||||||||||||||||||
| Never | 33.3 | 25.0 | 41.5 | ** | 31.8 | 38.6 | 28.0 | 40.7 | *** | 34.0 | 32.8 | 32.4 | 36.0 | * | 33.8 | 31.6 | |||
| A little | 27.0 | 23.3 | 30.0 | 26.7 | 28.1 | 32.2 | 20.4 | 25.5 | 31.3 | 29.0 | 22.7 | 25.8 | 34.2 | ||||||
| Some | 23.8 | 30.8 | 17.7 | 25.1 | 19.3 | 17.5 | 32.4 | 24.5 | 21.9 | 27.3 | 16.0 | 25.4 | 15.8 | ||||||
| A lot | 15.9 | 20.8 | 10.8 | 16.4 | 14.0 | 22.4 | 6.5 | 16.0 | 14.1 | 11.4 | 25.3 | 15.0 | 18.4 | ||||||
| Internet-related activities | |||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Participate in online discussion/chatrooms/listserv | |||||||||||||||||||
| No | 81.6 | 80.8 | 81.7 | 80.9 | 83.9 | 77.1 | 87.0 | * | 81.3 | 82.5 | 83.5 | 77.0 | 83.0 | 73.7 | |||||
| Yes | 18.4 | 19.2 | 18.3 | 19.1 | 16.1 | 22.9 | 13.0 | 18.7 | 17.5 | 16.5 | 23.0 | 17.0 | 26.3 | ||||||
| Read about others' experiences online | |||||||||||||||||||
| No | 54.8 | 51.7 | 57.6 | 53.8 | 57.9 | 48.6 | 62.6 | * | 53.2 | 58.7 | 59.7 | 44.0 | * | 55.2 | 52.6 | ||||
| Yes | 45.2 | 48.3 | 42.4 | 46.2 | 42.1 | 51.4 | 37.4 | 46.8 | 41.3 | 40.3 | 56.0 | 44.8 | 47.4 | ||||||
| Interest in getting information/support from | |||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Health organization websites | |||||||||||||||||||
| Not at all | 21.1 | 20.2 | 22.0 | 21.6 | 19.3 | 15.3 | 29.6 | 21.8 | 19.0 | 25.0 | 13.2 | 21.6 | 20.5 | ||||||
| Not very | 12.7 | 10.1 | 15.2 | 10.3 | 21.1 | 14.6 | 10.2 | 12.8 | 12.7 | 9.7 | 19.7 | 12.2 | 15.4 | ||||||
| Somewhat | 44.6 | 43.7 | 45.5 | 43.8 | 47.4 | 47.2 | 40.7 | 43.6 | 47.6 | 43.8 | 46.1 | 44.6 | 43.6 | ||||||
| Very | 21.5 | 26.1 | 17.4 | 24.2 | 12.3 | 22.9 | 19.4 | 21.8 | 20.6 | 21.6 | 21.1 | 21.6 | 20.5 | ||||||
| Government websites | |||||||||||||||||||
| Not at all | 29.5 | 31.7 | 27.3 | 31.8 | 21.4 | 25.9 | 34.3 | 28.7 | 31.7 | 28.4 | 31.6 | 31.9 | 15.4 | ||||||
| Not very | 13.5 | 11.7 | 15.9 | 11.3 | 21.4 | 13.3 | 14.8 | 15.4 | 9.5 | 15.3 | 10.5 | 14.1 | 12.8 | ||||||
| Somewhat | 40.2 | 40.0 | 40.2 | 39.5 | 42.9 | 41.3 | 38.9 | 40.4 | 39.7 | 40.3 | 39.5 | 39.0 | 46.2 | ||||||
| Very | 16.7 | 16.7 | 16.7 | 17.4 | 14.3 | 19.6 | 12.0 | 15.4 | 19.0 | 15.9 | 18.4 | 15.0 | 25.6 | ||||||
| Online courses or discussion groups | |||||||||||||||||||
| Not at all | 40.9 | 44.2 | 38.2 | 40.5 | 42.1 | 32.9 | 52.3 | ** | 38.3 | 48.4 | 40.9 | 41.9 | 43.2 | 28.9 | |||||
| Not very | 23.0 | 21.7 | 24.4 | 23.1 | 22.8 | 28.7 | 15.0 | 24.5 | 18.8 | 23.3 | 21.6 | 21.6 | 31.6 | ||||||
| Somewhat | 27.8 | 24.2 | 31.3 | 27.7 | 28.1 | 28.7 | 27.1 | 28.2 | 26.6 | 27.8 | 28.4 | 28.6 | 23.7 | ||||||
| Very | 8.3 | 10.0 | 6.1 | 8.7 | 7.0 | 9.8 | 5.6 | 9.0 | 6.3 | 8.0 | 8.1 | 6.6 | 15.8 | ||||||
| Perceived helpfulness of resources | |||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Practical tips from others with same problems | |||||||||||||||||||
| Not at all | 12.0 | 16.7 | 7.6 | ** | 13.3 | 7.1 | 8.4 | 16.8 | 10.1 | 17.5 | 15.3 | 4.1 | 14.1 | 2.6 | |||||
| Not very | 12.7 | 16.7 | 9.9 | 12.3 | 14.3 | 14.0 | 11.2 | 11.7 | 15.9 | 12.5 | 13.5 | 11.3 | 21.1 | ||||||
| Somewhat | 54.2 | 43.3 | 63.4 | 52.3 | 60.7 | 58.7 | 47.7 | 55.3 | 50.8 | 51.7 | 59.5 | 53.1 | 57.9 | ||||||
| Very | 21.1 | 23.3 | 19.1 | 22.1 | 17.9 | 58.7 | 47.7 | 22.9 | 15.9 | 20.5 | 23.0 | 21.6 | 18.4 | ||||||
| Get emotional support from people with similar problems | |||||||||||||||||||
| Not at all | 0.4 | 0.0 | 0.8 | 0.5 | 0.0 | 0.7 | 0.9 | 0.5 | 0.0 | 0.6 | 0.0 | 0.5 | 0.0 | ||||||
| Not very | 0.4 | 0.0 | 0.8 | 0.0 | 1.8 | 0.0 | 0.9 | 0.5 | 0.0 | 0.6 | 0.0 | 0.5 | 0.0 | ||||||
| Somewhat | 1.2 | 0.0 | 2.3 | 1.5 | 0.0 | 0.7 | 1.9 | 0.5 | 1.6 | 0.6 | 1.4 | 0.9 | 2.6 | ||||||
| Very | 98.0 | 100.0 | 96.2 | 97.9 | 98.2 | 98.6 | 96.3 | 98.4 | 98.4 | 98.3 | 98.6 | 98.1 | 97.4 | ||||||
| Learn how to exercise or eat better | |||||||||||||||||||
| Not at all | 13.6 | 16.0 | 11.5 | 14.4 | 10.7 | 12.6 | 15.9 | 12.8 | 17.2 | 14.2 | 12.0 | 13.6 | 13.2 | ||||||
| Not very | 4.8 | 6.7 | 3.1 | 4.1 | 7.1 | 3.5 | 5.6 | 4.3 | 6.3 | 5.1 | 4.0 | 5.6 | 0.0 | ||||||
| Somewhat | 40.4 | 34.5 | 45.8 | 40.2 | 41.1 | 42.7 | 37.4 | 42.6 | 34.4 | 39.8 | 42.7 | 40.8 | 39.5 | ||||||
| Very | 41.2 | 42.9 | 39.7 | 41.2 | 41.1 | 41.3 | 41.1 | 40.4 | 42.2 | 40.9 | 41.3 | 39.9 | 47.4 | ||||||
| Set goals and work with others trying to improve their health | |||||||||||||||||||
| Not at all | 16.7 | 17.5 | 16.2 | 17.9 | 12.3 | 12.5 | 23.1 | 15.4 | 20.3 | 16.5 | 17.3 | 18.3 | 10.5 | ||||||
| Not very | 9.5 | 4.8 | 4.4 | 8.2 | 14.0 | 9.0 | 10.2 | 10.1 | 7.8 | 8.5 | 10.7 | 10.3 | 2.6 | ||||||
| Somewhat | 53.6 | 50.8 | 56.2 | 50.8 | 63.2 | 58.3 | 46.3 | 54.3 | 51.6 | 54.0 | 53.3 | 50.7 | 71.1 | ||||||
| Very | 20.2 | 21.7 | 19.2 | 23.1 | 10.5 | 20.1 | 20.4 | 20.2 | 20.3 | 21.0 | 18.7 | 20.7 | 15.8 | ||||||
| Learn how to manage responsibilities and still take care of health | |||||||||||||||||||
| Not at all | 19.5 | 23.3 | 15.9 | * | 19.1 | 21.1 | 17.4 | 23.1 | 18.1 | 25.0 | 22.7 | 12.0 | 18.9 | 23.7 | |||||
| Not very | 13.1 | 10.8 | 15.2 | 10.3 | 22.8 | 9.0 | 18.5 | 13.8 | 10.9 | 11.9 | 14.7 | 14.6 | 2.6 | ||||||
| Somewhat | 45.0 | 36.7 | 52.3 | 48.5 | 33.3 | 48.6 | 39.8 | 44.1 | 46.9 | 41.5 | 54.7 | 44.3 | 50.0 | ||||||
| Very | 22.3 | 29.2 | 16.7 | 22.2 | 22.8 | 25.0 | 18.5 | 23.9 | 17.2 | 23.9 | 18.7 | 22.2 | 23.7 | ||||||
p < 0.05; **p < 0.01; ***p < 0.001.