
Abstract
Objective:
To evaluate the diagnostic accuracy of 10 clinical tests that can be used in the diagnosis of greater trochanteric pain syndrome (GTPS) in women, and to compare these clinical tests to magnetic resonance imaging (MRI) findings.
Materials and Methods:
Twenty-eight participants with GTPS (49.5 ± 22.0 years) and 18 asymptomatic participants (mean age ± standard deviation [SD], 52.5 ± 22.8 years) were included. A blinded physiotherapist performed 10 pain provocation tests potentially diagnostic for GTPS—palpation of the greater trochanter, resisted external derotation test, modified resisted external derotation test, standard and modified Ober's tests, Patrick's or FABER test, resisted hip abduction, single-leg stance test, and the resisted hip internal rotation test. A sample of 16 symptomatic and 17 asymptomatic women undertook a hip MRI scan. Gluteal tendons were evaluated and categorized as no pathology, mild tendinosis, moderate tendinosis/partial tear, or full-thickness tear.
Results:
Clinical test analyses show high specificity, high positive predictive value, low to moderate sensitivity, and negative predictive value for most clinical tests. All symptomatic and 88% of asymptomatic participants had pathological gluteal tendon changes on MRI, from mild tendinosis to full-thickness tear.
Conclusions:
The study found the Patrick's or FABER test, palpation of the greater trochanter, resisted hip abduction, and the resisted external derotation test to have the highest diagnostic test accuracy for GTPS. Tendon pathology on MRI is seen in both symptomatic and asymptomatic women.
Introduction
G
A number of clinical tests exist for the diagnosis of GTPS, however, there is limited analysis of their value in this condition. 12,15 –17 The commonly accepted clinical presentation is pain in the greater trochanteric region with pain on palpation of the greater trochanter, however, this has recently been redefined to include “in the absence of difficulty with manipulating shoes and socks” in an attempt to differentiate from hip osteoarthritis. 13 Pain in the greater trochanteric region during the Patrick's or FABER test is also identified as a key indicator 13,15 and a systematic review by Reiman et al. 18 demonstrated the ability to modify the post-test probability of a gluteal tendinopathy diagnosis using the resisted external derotation test. More recently, Grimaldi et al. 19 assessed the utility of numerous clinical tests and reported palpation of the greater trochanter to be highly sensitive (80%) and single leg stance of 30 seconds on the affected limb to be highly specific (100%) for the condition. 19 However, as no single test leads to a definitive diagnosis, a battery of tests is recommended for clinical assessment of hip abductor function. There is a need for further exploration of the use of clinical tests for efficient and accurate diagnosis of GTPS, and to confirm the findings of previous studies. 13,15,18,19
Despite known limitations of magnetic resonance imaging (MRI) as the reference standard in tendon disorders, 15 such imaging is used to diagnose GTPS. 16,17,20 –22 MRI can identify tendon pathology (peritendinitis, tendinosis, and partial and complete tears) and pathology in associated structures (bursal fluid, enthesopathic changes along the greater trochanteric insertion, fatty atrophy of the muscle), thought to be involved in GTPS. 16,20 MRI has a reported accuracy of 91%, sensitivity of 93%, and specificity of 92% for diagnosing hip abductor tendon tears, 17 but detection of abnormalities on MRI may be a poor predictor of trochanteric pain, as abnormalities are also present in asymptomatic patients. 12,15,21 Woodley et al. 15 reported that 82.5% of symptomatic patients had abnormal MRI findings in their study. However, 72.5% of asymptomatic patients also had abnormal MRI findings, indicating that pathology is not always reflective of clinical symptoms. Recent evidence investigating diagnostic accuracy of clinical tests with MRI as the gold standard may not provide an accurate evaluation of such tests for GTPS. 19
Greater trochanteric pain is a common complaint that presents to medical and allied health practitioners. There is limited knowledge about the accuracy of the current tests and investigations to diagnose GTPS, and this may result in misdiagnosis and ineffective interventions. The aim of this study is to estimate the diagnostic accuracy of clinical tests that can be used in the diagnosis of greater trochanteric pain syndrome in women. This study will further compare these clinical tests to MR findings in women with greater trochanteric pain syndrome.
Materials and Methods
Participants
A total of 46 female participants who responded to a community advertising flyer or who were referred by health professional practices (general practitioners, physiotherapists) were recruited for the study between May 1st and August 18th, 2014; 28 participants with greater trochanteric pain and 18 asymptomatic participants. Asymptomatic participants had no history of lower back, hip, or lower limb injury that they had sought treatment for in the 3 months before the study. Symptomatic participants had reported history of greater trochanteric pain and pain with two or more of the following activities: lying on the ipsilateral side, 23 –25 sitting, 1 moving from sitting to standing, or ascending/descending stairs or slope. 15 Participants who reported any signs of intra-articular hip pathology or osteoarthritis (locking or catching in the joint, range of movement restriction, difficulty manipulating shoes and socks) were excluded. 13,26 Those who reported seeking treatment for back or other lower limb pathologies (e.g., knee and foot injuries) in the last 3 months were excluded. The La Trobe University Ethics Committee approved all research procedures (FHEC 14/015) reported in this study and all participants gave written informed consent before participation.
To assess differences in pain and function between groups, participants completed the Victorian Institute of Sport Australian Questionnaire for gluteal tendinopathy (VISA-G). The VISA-G is the only gluteal tendinopathy outcome measure available to reliably monitor and quantify pain with tendon loading. 27 The extent of functional limitations can be quantified using the VISA-G with a higher score representing less pain and dysfunction. 27 Anthropometric data (height and weight) were recorded for each participant.
In a random order (clinical tests selected from an opaque box), hip pain provocation tests were performed in a university research laboratory, by a physiotherapist (TP), with over 15 years of experience, blinded to group allocation. Pain experienced during the tests was categorized into (1) greater trochanteric pain, the area ∼7 cm proximal and distal, and 3 cm anterior and posterior of the greater trochanter 13 and (2) nonspecific hip pain, defined as lateral, anterior, and posterior hip pain, buttock, and groin pain beyond the area defined above. 28 Ten clinical tests potentially diagnostic for GTPS were completed—palpation of the greater trochanter, 29 resisted external derotation test, 14 modified resisted external derotation test (compression and contraction components), standard and modified Ober's tests, 15 Patrick's or FABER test, 13,30,31 resisted hip abduction, 12,32 single leg stance test, 14 and the resisted hip internal rotation test 12 (Table 1). A positive test was defined as a spontaneous reproduction of greater trochanteric pain. Reports of a stretching sensation or feeling of tightness over the lateral hip were considered a negative test.
Photos used with permission from the patient and therapist.
ER, external rotation; ASIS, anterior superior iliac spine.
Magnetic resonance imaging
A sample of 17/18 asymptomatic and 16/28 symptomatic self-selected female participants undertook a MRI scan of their hip within 4 weeks of their clinical examination. Participants were asked to opt in or opt out of an MRI scan. As many of the symptomatic participants had previously had a hip MRI, 12 participants declined the offer for a further MRI scan. Standard exclusion for the use of MRI was applied in this cohort (e.g., pregnancy, internal metal work in the ipsilateral hip, and claustrophobia), however, no participants were excluded. Only one hip per participant was imaged. The symptomatic hip of those with unilateral greater trochanteric pain was imaged, the most symptomatic hip (participant self-report) of those with bilateral greater trochanteric pain was imaged, and for asymptomatic participants, the imaged hip was determined by coin toss. MR studies were performed on a 3-Tesla SIEMENS MAGNETOM Verio syngo MR B19 system using a phased array surface coil, and took ∼30 minutes to complete. The imaging sequences encompassed all structures from the ASIS to the lesser trochanter of the femur. T1 and proton density (PD) weighted images with and without fat saturation were acquired in axial, transverse, and coronal planes. Field of view, slice thickness, and TR/TE values are as indicated in Table 2.
AXPD, axial proton density; AXPDFS, axial proton density fat saturated; AXT1, axial T1-weighted image; COR PDFS, coronal proton density fat suppressed; CORPD, coronal proton density; FOV, field of view; P/E, phase encoding; SAGPD, sagittal proton density; TE, echo time; TR, repetition time.
All MR scans were independently analyzed by two blinded fellowship-trained radiologists with over 15 and 10 years of experience, respectively. Radiologists were asked to report on all pathology in the hip/gluteal region of interest and tendon was examined using methods based on those described by Blankenbaker. 21 Blankenbaker's grading system evaluates the presence of T2 hyperintensity and categorizes it as subtendinous, intratendinous, subfascia lata, or superficial to fascia lata. The grading system for this study was adapted to apply to PD and PD fat-suppressed sequences rather than T2-weighted sequences. In cases of disagreement, diagnosis was to be reached by consensus.
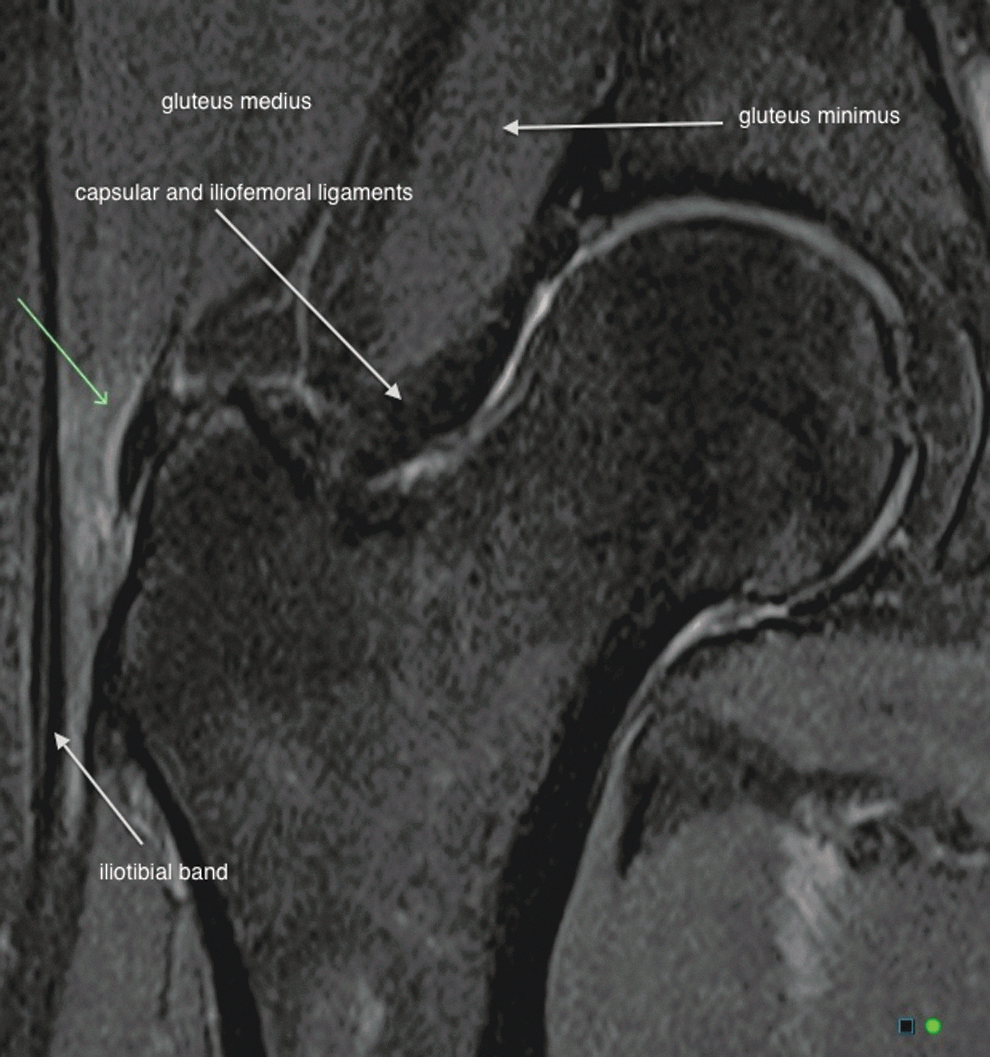
Modified from the protocol described by Blankenbaker et al., 21 intratendinous high PD signal was considered as tendinosis with a thickened tendon without any irregularity, tendon thinning, or focal tendon discontinuity. Tendinosis was then further subclassified into mild or moderate assessed by the radiologist. Partial-thickness tear was diagnosed when the tendon was irregular, thinned, or focally discontinuous and a complete tear was diagnosed when discontinuity and/or retraction of the torn tendon was seen. 12,21,33 Once reported, pathology was broadly categorized into four main groups for ease of interpretation for the reader: no pathology, mild tendinosis, moderate tendinosis or partial tear, and full-thickness tear (Figs. 1 –4).

Partial tear. MR system image (3.0T): small field of view coronal PD-weighted fat saturated image (TR 3490 TE 42) of the right hip shows a partial tear of the gluteus medius tendon. High signal intensity fluid (green arrows) is seen within the tendon fibers as the tendon attaches to the greater trochanter. PD, proton density.
Mild tendinosis. MR system image (3.0T): small field of view coronal PD-weighted fat saturated image (TR 3490 TE 42) of the right hip shows edema (green arrows), which is categorized as small sized, feathery, intratendinous with mild tendon thickening of gluteus minimus, but without tendon disruption or discontinuity.

Moderate tendinosis. MR system image (3.0T): small field of view coronal PD-weighted image (TR 2250 TE 33) of the left hip shows edema, which is categorized as medium sized, round, intratendinous with moderate tendon thickening of gluteus medius (green arrows), but without tendon disruption or discontinuity.

Full-thickness tear. MR system image (3.0T): small field of view coronal PD-weighted fat saturated image (TR 3490 TE 33) of the left hip shows a complete tear of the gluteus minims tendon with tendon discontinuity and retraction of the tendon ends (green arrows) separated by a fluid-filled gap.
Data analysis
A Kolmogorov–Smirnov test demonstrated that age, anthropometric data, and VISA-G scores were not normally distributed, so Mann–Whitney U tests were performed in IBM SPSS (Version 22, Chicago, IL) to determine differences between groups for these variables. A p-value >0.05 was considered significant.
Assessment of diagnostic accuracy relies on a comparison with a gold standard test, 34 however no gold standard exists for the diagnosis of GTPS. Imaging abnormalities can be present in asymptomatic patients, 12,15,21 thus dichotomizing data by MRI may be inappropriate. Instead, to compare the accuracy of clinical tests, groups were dichotomized into symptomatic and asymptomatic participants based on symptoms during functional tasks. Symptomatic participants were defined as having: (1) no difficulty with manipulating shoes and socks; (2) greater trochanteric pain during two of three specific functional activities—lying on the affected hip, ascending or descending stairs/slopes/ramps, and pain moving from a sitting to standing position.
A positive clinical test result was defined as the production of pain in the greater trochanteric region. Sensitivity and specificity analyses were performed 35,36 using 2 × 2 tables. Calculation and interpretation of the positive predictive value (PPV), negative predictive value (NPV), odds ratio (OR), positive likelihood ratio (LR+), and negative likelihood ratio (LR−) for each clinical test were performed in Microsoft Excel using previously described formulas. 37 A fixed value of 0.5 was added to all cells of 2 × 2 tables where a zero-cell count occurred (standard and modified Obers and resisted hip abduction), as recommended by the Cochrane Collaboration (studies with zero-cell counts). 38 The percentage of MR pathology in the asymptomatic and symptomatic groups was calculated.
Results
All 46 participants were women with a median (interquartile range) age of 50.5 (22.5) years. There was no significant differences in age, height, weight, or body mass index (BMI), however a trend toward symptomatic participants having higher weight (p = 0.065) and BMI (p = 0.076) existed. A significant difference was identified in VISA-G scores (p < 0.01) (Table 3).
BMI, body mass index; IQR, interquartile range.
Diagnostic tests evaluated in this study were good at ruling out the condition, but minimally effective at ruling the condition in Table 4. Clinical test analyses show high specificity (≥83%), high PPV (≥75%), and low to moderate sensitivity and NPV for all clinical tests. The main exception was palpation of the greater trochanter that had high sensitivity (85.7%), low specificity (61.1%), and LR-ratio of 0.2.
LR−, negative likelihood ratio; LR+, positive likelihood ratio; NPV, negative predictive value; OR, odds ratio; PPV, positive predictive value.
Patrick's or FABER test, palpation of the greater trochanter, and resisted hip abduction were the most sensitive. Modified and standard Ober's test results were less likely to indicate GTPS, demonstrating poor sensitivity and likelihood ratio confidence intervals (CIs) that contained the null value. Four tests had an OR greater than or equal to 11 for having GTPS, and a LR+ ratio of >7 (resisted external derotation test, the modified resisted external derotation test—contraction component, resisted hip abduction, resisted internal rotation test—Table 4). All other tests were found to have moderate diagnostic test accuracy.
All symptomatic participants were found to have pathology on imaging, with consistent findings between both radiologist examiners. Pathology was present in 88% of asymptomatic participants, ranging from mild tendinosis to full-thickness tear (Table 5). Pictorial examples of MRI classifications can be seen in Figures 1 –4.
FT, full thickness.
Discussion
This study evaluates 10 clinical tests of hip pathology for diagnosing GTPS, with the aim of identifying tests with superior diagnostic test accuracy, taking into account all statistical measures. From these preliminary results, the four most valuable tests for the diagnosis of GTPS are palpation of the greater trochanter, Patrick's or FABER test, resisted hip abduction test, and the resisted external derotation test. Moderately valuable tests include resisted hip internal rotation test, single leg stance test, and modified resisted external derotation test (compression and contraction components). The least valuable clinical tests were the standard and modified Ober's test. These findings should be viewed in light of variability across some of the tests with wide CIs for some sensitivity and specificity values and inclusion of the null value for OR and LR CIs for the two Ober's tests and LRs of the single leg stance test. The resisted hip abduction test, displayed considerably large CIs for OR and LR, but was still included in the four recommended tests based on reasonable specificity, PPV, and NPV values.
Excessive compression is thought to be important in the development of insertional tendinopathies. 39 Clinical tests thought to compress the gluteus medius and minimus tendons included the static component of the modified external derotation test, Ober's tests, and palpation. Pain on greater trochanter palpation is reported to be a key indicator of GTPS 1,2,5,12,14,23 –25,40 and an inclusion criterion for many GTPS studies. It is not surprising that palpation tenderness was found to be the most sensitive test in this study and in the most recent article by Grimaldi et al. 19 Direct pressure over and surrounding the greater trochanter is likely to cause compression of the tendinous insertions, reproducing symptoms in individuals with greater trochanteric pain. Pressure pain thresholds have been used in the gluteal tendons, 24 and the other tendons 41 –43 as an assessment tool to monitor effectiveness of treatment interventions. Palpation was also the most likely test to elicit pain from asymptomatic participants, increasing the number of false-positive results and lowering the PPV.
During the modified resisted external derotation test, the hip is passively taken into 90° of flexion and full adduction. Due to the widespread gluteal and lumbodorsal fascial connections, 44 this may increase compressive load of the gluteus medius and minimus tendons. Previous research has shown an increase in subligamentous forces from 4 N to 106 N 45 during 0–40° hip adduction. The combination of flexion and adduction forces may further increase this compressive load. Lower sensitivity found during resisted external derotation test and the contraction component of the modified external derotation test may be reflective of decreased compressive load through the gluteal tendons, as the leg is returned to a neutral position.
The standard or modified Ober's tests are reported to be a useful diagnostic tests in the literature. 15 This study reported low sensitivity values for both tests, however, a +LR of 5.4 (standard Ober's test) and 5.6 (modified Ober's test) would be considered to have moderate effect on posttest probability of GTPS. 46 CIs for +LR cross the null value of 1, so at this stage, these tests could not be used confidently in the diagnosis of GTPS. Also, a −LR of 0.9 for both tests, had no effect on posttest probability. 46 Although a clinical association of hip abductor dysfunction, iliotibial band (ITB) compression 47 and tensor fascia latae (TFL) relative hypertrophy has been reported, 48 results suggest the Ober's Test positioning may not provide enough tendinous compression to elicit pain. Additionally, the length of the ITB and TFL may limit the amount of adduction able to take place during these tests.
The single leg stance test might briefly mimic the gluteal tendon compression and contraction 49 that occurs particularly during walking and single leg stance activities, secondary to poor femoropelvic control. 48 However, it does not account for the dynamic element of pelvic rotation that occurs in gait. Our study allowed participants to place their fingertips on a wall on the side of the symptomatic hip for balance, potentially reducing compression that occurs with symptomatic hip adduction. This test was found to be useful for ruling out the condition, but not ruling it in. These results reflect those in a recent study by Grimaldi et al., 19 where they found 100% specificity and 38% sensitivity during a 30-second single leg stance test. In comparison, Lequesne et al. 14 showed 100% of their 17 participants to have a reproduction of pain during a single leg stance test. Differences may be due to population—Lequesne et al. 14 did not test an asymptomatic population.
More recently, a positive Patrick's or FABER test has been used to define GTPS during clinical examination. 13 In our analysis, the test showed high specificity and the second highest sensitivity. Furthermore, the likelihood ratios suggest a small increase in the likelihood of the disease with a positive finding and minimal decrease in the likelihood of the disease with a negative finding. 37 For example, if pretest probability for a postmenopausal woman presenting with localized greater trochanteric pain with no hip joint range restriction having GTPS was estimated as 60%, a positive Patrick's or FABER test would be considered to have slight to moderate effect on posttest probability, 46 increasing to 80% when using a nomogram and the LR+ of 3.0. A negative test result with an LR− of 0.6 has a slight effect on posttest probability, 46 and reduces the chance to 30% on a nomogram. Pain reproduction during this test may involve elongation and/or compression of the tendon and bursae. When passive external rotation range is completed at 90° hip flexion, gluteus minimus muscle excursion lengthens up to 30 mm when compared with external rotation at neutral hip position. 50 Anatomically, an external rotation movement opposes the internal rotator pull of the anterior gluteus medius and minimus, 51 imposing an elongation force on their respective tendons. The elongation and potential compression of underlying thickened pathological bursae may result in a pain response. However, during 0–20° of abduction (a component of the final position of the Patrick's or FABER test), they have been found to shorten 15 mm. The contrast in findings between the three movements, provides a confusing picture as to the reasons Patrick's or FABER elicits greater trochanteric pain. 50
The finding of Beck et al. 50 of lengthening muscle fibers during flexion and external rotation can also be applied to the resisted internal rotation test, and the standard and modified resisted external derotation tests. During all three tests, the gluteus minimus tendon may be exposed to increased compression over the anterior and lateral facets of the greater trochanter as they wrap around the anterosuperior aspect of the hip joint. 52 Furthermore, the gluteus medius tendon and trochanteric bursae are likely to be compressed during adduction as the tendon wraps around the posterolateral aspect of the greater trochanter.
Clinical tests that involved contraction of the deep gluteal musculature against therapist resistance demonstrated high specificity and moderate sensitivity for pain reproduction. Conversely, previous studies have reported a positive relationship between pain reproduction with resisted hip abduction and presence of GTPS 2,12 or gluteal tendon tear (sensitivity 72.7%, specificity 46.2%). 12 This is likely due to methodological differences—Karpinski 2 did not specify the method of hip abduction testing and Bird et al. 12 completed testing in supine. Additionally, Bird et al. 12 and Lequesne et al. 14 recruited participants from tertiary referral centers, unlike this study, where participants were recruited from a community population. This may influence the symptomology of the included participants—those that have presented to tertiary referral centers, may have higher levels of pain and dysfunction and increased sensitivity of these clinical tests.
Isometric internal rotation and tests that involved a dynamic contraction from an externally rotated position to hip neutral had varying results—either elevating or reducing pain response. Reduction in pain may reflect a lessening of tendon compression as the anterior portion of gluteus medius and minimus contract to internally rotate out of the compressed position. 51 Elevated pain response may be indicative of a fully ruptured tendon, whereby the primary internal rotator function is inhibited and compensatory abductor recruitment and muscle patterning may be used.
The association between tendon pathology on imaging (tendinosis) and symptomatic tendon pain (tendinopathy) on clinical examination has been challenged in the literature. Mayordormo 53 found gluteal bursal enlargement in 30% of their asymptomatic control group and Woodley 15 reported gluteus medius and minimus tendinopathy, tendon tears, bursitis, and mild osteoarthritis in the asymptomatic hips of subjects with unilateral greater trochanteric pain. Analogous to the presence of degenerative disc disease 54 –56 and rotator cuff tears 57 of the shoulder in asymptomatic populations, false-positive results for 15 of 17 asymptomatic participants in this study, reflects the lack of an association between clinical and imaging findings in this condition.
Based on the results of the current study, undertaking of a series of pain provocation tests (palpation of the greater trochanter, Patrick's or FABER, resisted hip abduction and the modified resisted external derotation test) could be useful for diagnosing GTPS. Radiological investigation with a MRI scan, may be of little value to the management of this condition, however, is an important tool to rule out more sinister pathologies (e.g., tumor, infection) 58 and other potential causes of hip pain (e.g., lumbosacral spine and sacroiliac joint pathology). Future research may consider investigating clinical prediction rules, whereby a selected number of tests must be positive before diagnosis of the condition can be made.
Study limitations
Although ultrasound and MRI are used widely to diagnose this condition, there is yet to be a gold standard identified. It remains difficult to fully assess the diagnostic accuracy of the clinical tests used in greater trochanteric pain. Despite this, the dichotomy used in this study was able to demonstrate differences in VISA-G scores between the groups. The small sample of MR images has the potential of reducing the generalizability of results, however, MRI findings were consistent across both examiners and quality of interpretation was preserved with both fellowship-trained radiologists, renowned as leaders in the field of musculoskeletal hip imaging. Very large CIs were seen in diagnostic tests (resisted hip abduction, modified and standard Ober's), where an addition of 0.5 to empty cells was undertaken. This may be ameliorated with a larger sample size, by reducing the likelihood of needing this computation to run validity analyses. Variation on therapist applied resistance for all the resistance-based tests is a risk when used in the community physiotherapy environment. In addition, no clearing tests for the lumbar spine were included in the clinical examination; however, individuals reporting treatment for back pathologies were excluded.
Conclusion
The study found the Patrick's or FABER test, palpation of the greater trochanter, resisted hip abduction, and the resisted external derotation test to have the highest diagnostic test accuracy for GTPS. All other tests were found to have moderate diagnostic test accuracy. The use of standard Ober's and modified Ober's, to diagnose the condition is not supported. The study identified that all symptomatic participants and 88% of asymptomatic participants had pathological gluteal tendon changes on MRI. Further research may investigate if these clinical tests are accurately able to differentiate GTPS from other hip pathologies in a mixed population.
Footnotes
Acknowledgments
C.G. acknowledges the Australian Postgraduate Award scheme and the Graduate Assistantship program at La Trobe University for her PhD scholarship funding. J.C. acknowledges an affiliation with the Australian Center for Research into Sports injury and its Prevention, which is one of the international research centers for Prevention of Injury and Protection of Athlete Health supported by the International Olympic Committee (IOC).
Key Points
Authors Contribution
All authors have participated sufficiently in the conception and design of this work and the analysis of the data, as well as the writing of the article to take public responsibility for its content. Authors declare the article is original and its essential substance, tables, or figures have not been previously published in part or in whole.
Author Disclosure Statement
No competing financial interests exist.