
Abstract
Background:
More than a third of hospitalized women are both overdue for breast cancer screening and at high risk for developing breast cancer. The purpose of the study was to evaluate if inpatient breast cancer screening education, scheduling an outpatient mammography appointment before hospital discharge at patients' convenience, phone call reminders, and a small monetary incentive ($10) would result in improved adherence with breast cancer screening for these patients.
Methods:
A prospective intervention pilot study was conducted among 30 nonadherent women aged 50–75 years hospitalized to a general medicine service. Sociodemographic, reproductive history, family history for breast cancer, and medical comorbidity data were collected for all patients. Chi-square and unpaired t-tests were utilized to compare characteristics among women who did and did not get a screening mammogram at their prearranged appointments.
Results:
Of the 30 women enrolled who were nonadherent to breast cancer screening, the mean age for the study population was 57.8 years (SD = 6), mean 5-year Gail risk score was 1.68 (SD = 0.67), and 57% of women were African American. Only one-third of the enrolled women (n = 10) went to their prearranged appointments for screening mammography. Not feeling well enough after the hospitalization and not having insurance were reported as main reasons for missing the appointments. Convenience of having an appointment scheduled was reported to be a facilitator of completing the screening test.
Conclusion:
This intervention was partially successful in enhancing breast cancer screening among hospitalized women who were overdue and at high risk. Future studies may need to evaluate the feasibility of inpatient screening mammography to improve adherence and overcome the significant barriers to compliance with screening.
Introduction
B
The purpose of the current study was to evaluate whether an intervention that included breast cancer screening education during a hospital stay, coupled with scheduling an outpatient mammography appointment before hospital discharge, would improve adherence with screening. We hypothesized that the intervention would result in a 50% increase in breast cancer screening adherence.
Methods
Study design and sample
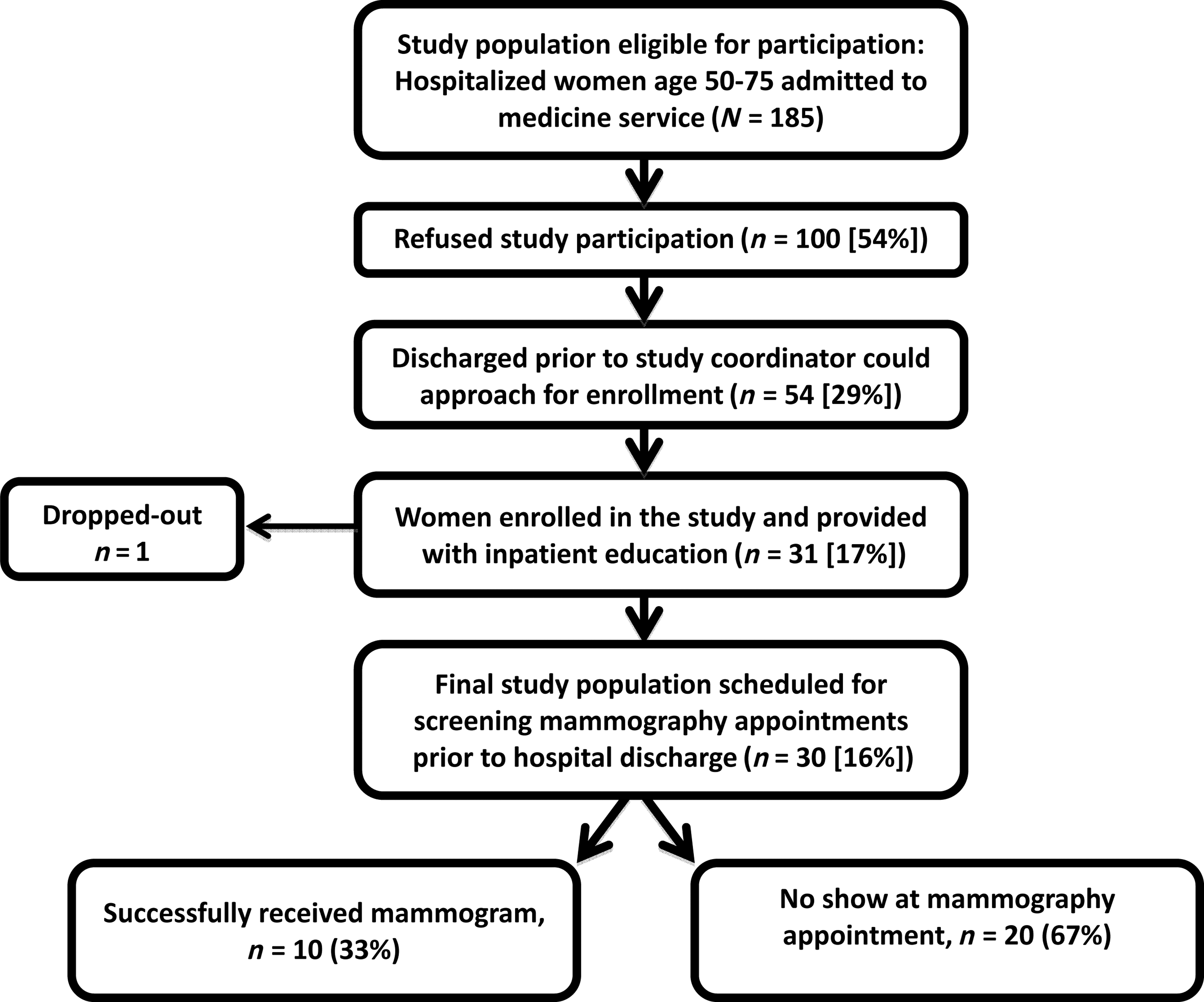
In this prospective intervention study, all women between 50 and 75 years of age admitted to the general medical service at Johns Hopkins Bayview Medical Center (JHBMC) were assessed to determine study eligibility. Only women who were nonadherent to breast screening guidelines were approached for study participation between October 2012 and March 2013. “Nonadherence with breast cancer screening” recommendations was defined as having had a screening mammography more than 24 months before enrollment among women aged 52 or older—in accordance with guidelines by the United States Preventive Services Task Force (USPSTF). 6 Patients who had multiple admissions during the study period were only offered enrollment during their first hospitalization. Of the 655 eligible women, 245 (37%) were adherent to screening mammography (self-reported last screening mammogram less than 24 months), and many met exclusion criteria (32 [5%] had a history of breast cancer, 40 [6%] reported a history of cancer other than breast with metastasis or were undergoing active treatment, 69 [11%] admitted with confusion, 26 [4%] were residents of nursing homes, 36 [5.5%] were significant physically disabled, and 22 [3.3%] had communication constraints that limited interaction with the research assistant [deaf, aphasia, non-English speaking]). Taking the abovementioned into account, only 185 women were eligible for the study. Of these qualified hospitalized women, 100 (54%) refused to participate, and 54 (29%) were discharged from the hospital before the study coordinator could consent them. Only 31 (17%) hospitalized women were nonadherent to breast cancer screening recommendations and willing to participate in the study. One patient dropped out of the study after agreeing to participate. Thus, final study population consisted of 30 (16%) women, of whom 23% (n = 7) never had a screening mammogram. Detailed enrollment information can be seen in Figure 1.
Study population.
Protocol and measures
The bedside data collection consisted of survey questions regarding sociodemographic information such as race, education, and annual household income. Several questions regarding breast cancer risk factors, including reproductive history, family history of breast cancer, and personal history of breast biopsy, were also asked to generate “Gail Risk Prediction Score” using the National Cancer Institute Breast Cancer Risk Tool (
Study intervention
The study coordinator provided bedside education about breast cancer and the benefits of screening mammography, handouts with information, and pictures were also given to patients. The same individual also did general counseling and offered encouragement to the patients. Participants were then scheduled by the study coordinator to have an appointment for outpatient screening mammography at a convenient day/time and at their preferred mammography facility/center. Attempts were made to schedule the screening appointments 2–4 weeks after hospital discharge. After discharge from the hospital, patients received a reminder about their forthcoming appointments by phone call, 24 hours before their scheduled appointments. On successfully completing their screening appointment, a $10 gift card was mailed to their home address. Patients were explained that the gift card could be used to offset the cost associated with transportation to their appointments. A short follow-up survey was done within 1 week after the scheduled appointment to assess the patient's compliance with their scheduled appointments and to evaluate their experience with their appointments or barriers if they missed the mammogram.
The Institutional Review Board at JHBMC approved the study protocol. All study participants provided their written informed consent for participation.
Outcome and evaluation
Our primary outcome of interest was the proportion of women who underwent a screening mammogram posthospitalization. We also evaluated patients' satisfaction with the study intervention (via phone survey) after completion of screening appointments as a secondary outcome.
Statistical methods
Respondent characteristics are presented as proportions and means. Unpaired t-test and Fisher's exact tests were used to compare demographic and socioeconomic characteristics among women who did and did not get a screening mammogram at their prearranged appointments. T-tests and Fisher's exact tests determined significance at p-value ≤0.05. Data were analyzed using the Stata statistical software (StataCorp LP, Version 13.1).
Results
The mean age of the study population was 57.8 years, 57% were African American, 3% were uninsured, and 37% women were at high risk for breast cancer (5-year risk prediction Gail score ≥1.7%). Characteristics of the study participants are shown in Table 1. There were almost no differences in characteristics among women who did and did not get their screening mammogram except that women who received outpatient screening mammogram were more likely to be Caucasian (p = 0.007), admitted under observation status (p = 0.05), and had a shorter hospital length of stay (p = 0.009).
Fisher's exact statistic.
Unpaired t-test statistic.
Gail score was estimated using the National Cancer Institute Breast Cancer Risk Tool (
Family history of breast cancer was defined as breast cancer in first-degree relatives (i.e., mother, sisters, or daughters).
Three-quarters of the screening mammography appointments were scheduled between 2 and 4 weeks after hospital discharge. The others, 26% (n = 8) were scheduled 4–5 weeks after discharge because of patient preference.
One-third of the study population, 10 women, successfully completed the screening mammography appointments. Of them, five women (50%) required additional imaging and follow-up.
The most common barriers described by the 30 women who enrolled in our study who were previously nonadherence to breast cancer screening guidelines were “no specific reason for nonadherence or just putting it off” (40%), “family, personal, or medical issues” (17%), and “not having insurance” (17%). Similarly, the most commonly cited barriers for not following up for the postdischarge screening mammography appointments (n = 12) included “not feeling well enough to go to the appointment,” “forgot appointment,” “family issues,” and “lack of insurance.”
Of the 10 women who were successful in having their mammograms following discharge, all (100%) were satisfied with the appointment being set up while they were in the hospital. All (100%) would recommend this timing and method of scheduling appointments to family and friends who were overdue for it at the time of hospitalization, and 100% would want to have their appointments scheduled after hospital discharge in the future if they were noted to be overdue again while in the hospital (Table 2).
Two patients did not participate in follow-up survey.
Discussion
This study demonstrates the outcomes associated with efforts to improve breast cancer screening among nonadherent hospitalized women through a multipronged intervention; inpatient breast cancer screening education, scheduling an outpatient mammography appointment at patients' convenience following discharge, a phone reminder 24 hours before screening appointments, and a small financial incentive ($10 gift card) to partially offset transportation costs. This pilot shows that it is feasible to coordinate mammograms after discharge, which could improve the adherence to breast cancer screening guidelines. However, this was only possible after screening many hospitalized women (N = 185), of whom only a small number (n = 30) could be enrolled and fewer still ultimately went on to complete a screening mammogram (n = 10). The study participants who were able to receive a screening mammogram after discharge were satisfied with the encouragement, convenience, and would both do it again and recommend this to friends and family.
The concept of improving breast cancer screening through inpatient education is not entirely new. Boling used inpatient brochures to describe and encourage screening mammography among hospitalized women aged 40–80 years. 14 At 3 months posthospitalization, only 54% of their subjects were reachable for follow-up, and only 15% underwent screening mammography. They concluded that the inpatient education intervention was successful as it induced changes in patients' screening behaviors. Our findings were consistent with Boling's (33% underwent screening mammography), however, to achieve this we counseled, scheduled the appointment at the patients' preferred site and time, called them with a reminder 24 hours before the test, and provided a small monetary incentive of $10 gift card for successful screening appointment. The Boling study data coupled with our findings reiterate the significant barriers in securing mammography following discharge, which are not markedly different from the barriers described related to breast cancer screening noted at any other time. 3
Dole and Carney reported that voucher program for promoting screening mammography among highly motivated women may be effective for some women. 15 It was felt that this strategy would not work for those who were at greatest risk for nonadherence (i.e., without access to healthcare). 15 This is also consistent with our finding that women who failed to show up for their appointments were more likely to be uninsured and without a primary care provider (although both statistically not significant). We noted a trend in which women who received mammography were more likely to be at higher risk for breast cancer (mean 5-year risk prediction using Gail model 1.98) compared to women who failed to come to their appointments (Gail score: 1.5).
Several limitations of this study should be considered. First, this study was conducted at a single hospital. Second, our study sample size was small, however, it was large enough to evaluate the feasibility of the pilot intervention. Third, only one-third of the study population received outpatient screening mammography. The reason for this may be due to slow recovery from acute illness. This may be supported by the fact that those with shorter length of stay were more likely to follow up for mammography. It is also possible that mammogram appointments made for 4–5 weeks posthospitalization may be most successful in enhancing optimal screening adherence rates. Both too soon (within days) and too long (beyond 2 months when patients have returned to work/baseline and are thinking less about preventive health) are suboptimal. Scheduling these appointments in the window (2–4 weeks) seemed most appropriate to our study team and all study participants seemed agreeable and in favor of this time span. Fourth, our relationship with mammography centers (both internal and external) made it fairly easy to set up the appointments for these patients. However, this may not be the case in every community. Fifth, almost 50% of hospitalized women who were eligible declined to participate. Hospitalized patients are relatively sick and medically complex; this may explain the lower participation in research studies compared to healthy volunteers or patients presenting to clinics. Finally, we struggled with posthospitalization patient follow-up, in that we could not reach almost one-third of the enrolled women, either to remind them of their appointment or to assess barriers. This is clinically relevant because half of the women who completed the study intervention needed additional imaging for completion of screening.
Conclusion
In summary, a multipronged intervention consisting of inpatient education/counseling, scheduling appointments at patients' convenience, appointment reminders, and small incentive was somewhat successful for achieving the goal of securing screening mammography for hospitalized women who were overdue. It remains to be seen whether the efforts to screen and enroll patients are justified by the few who ultimately went on to have the test. As our hospitals are moving toward full assimilation into accountable care organizations, tests needed for preventive care should be made available to patients wherever they interact with healthcare system. This is especially true for patients at highest risk.
Footnotes
Acknowledgment
Dr. Wright is a Miller-Coulson Family Scholar supported by Hopkins Center for Innovative Medicine.
Author Disclosure Statement
No competing financial interests exist.