
Abstract
Background:
Prepregnancy maternal obesity and excessive weight gain during pregnancy lead to significant morbidities in mothers and their children. Mothers who never return to their prepregnancy weight begin subsequent pregnancies at a greater weight and have a larger propensity for excess gestational weight gain and postpartum weight retention.
Methods:
In this pilot study, 40 postpartum women credentialed to receive postpartum women, infants, and children (WIC) service were randomized to usual care (“WIC Moms”) or a personalized health intervention delivered via a SmartPhone (“E-Moms”). Assessments, including body weight, vital signs, circumferences, and body composition, were completed at week 0 (6–8 weeks postpartum), week 8, and week 16.
Results:
Results are presented as change from week 0 at 16. As per the completers analysis, body weight change was not different between the groups (WIC Moms vs. E-Moms; 1.8 ± 0.9 vs. −0.1 ± 0.9 kg; p = 0.10), neither was the change in percent body fat (1.7 ± 0.6 vs. 0.1% ± 0.6%; p = 0.90) or waist/hip ratio (−0.01 ± 0.01 vs. −0.02 ± 0.01 cm; p = 0.60). However, due to notable variability in intervention adherence as the study progressed, participants were classified post hoc as having low (<40% adherence), medium (40%–70% adherence), or high adherence (>70% adherence). Participants with high intervention adherence (n = 5) had a significant reduction in body weight (−3.6 ± 1.6 vs. 1.8 ± 0.9 kg; p = 0.005) and percent body fat (−2.5 ± 1.0 vs. 1.7% ± 0.6%; p = 0.001) when compared to WIC Moms.
Conclusions:
Overall, the E-Moms intervention was not able to decrease postpartum weight retention in women receiving WIC benefits compared to usual care received through the current WIC program. However, there is some evidence to suggest improved adherence to the intervention would improve weight management.
Introduction
T
The most successful weight management programs are intensive, employing frequent in-person contact, a specific dietary prescription, and individualized feedback on body weight change and dietary intake. 5 –8 Intensive in-person programs have several limitations including financial and geographical barriers that prevent many individuals from obtaining these services. In-person interventions do not typically provide timely treatment advice to individuals and have limited scalability, making dissemination of the lifestyle intervention to large numbers of individuals costly and impractical. 9 –11
New to the mobile health (mHealth) technology domain is delivery of weight management programs via SmartPhones. SmartPhones provide a platform for objective data collection and delivery of data-driven feedback and treatment advice almost immediately. With SmartPhones, people are “mobile” and less reliant on computers for Internet access. 12 SmartPhones are the fastest growing segment of the cell phone market, 13 and 90% of adults in the United States use SmartPhones. 12 Minorities are the most frequent users of mobile Internet, and low-income households are more likely to rely solely on SmartPhones for Internet access. 14 These data clearly indicate that SmartPhone-based programs could be effective at reaching individuals with limited access to healthcare.
Thus, the objective of this study, E-Moms: A personalized mHealth intervention for health and weight loss in postpartum women, is to capitalize on the ease of increased contact and information delivery through SmartPhones to promote weight loss and improve diet quality in overweight and obese postpartum women enrolled in the supplemental nutrition Women, Infants, and Children's program.
Materials and Methods
This randomized controlled trial (Clinical trials identifier: NCT 01751230) is part of the women, infants, and children (WIC) Periconception Network, which is a cluster of seven independent studies aimed at understanding the impact of obesity throughout the periconception period. The Institutional Review Boards (IRB) at Pennington Biomedical Research Center, University of California Los Angeles, and Louisiana Department of Health and Hospitals approved the research, and all participants provided written informed consent before participation.
Participants
Forty women were recruited using IRB-approved brochures at two local WIC clinics in Baton Rouge, LA, during the first postpartum WIC certification visit. Participants were required to be postpartum females who gave birth less than 8 weeks ago, ≥18 years old, overweight or obese (body mass index [BMI] ≥25 and <40 kg/m2), certified for WIC postpartum services, and English speaking. Participants were ineligible if they were enrolled in the Nurse Family Partnership program, had a multiple gestation in the index pregnancy, a history of psychiatric conditions or chronic disease that can impact body weight, appetite, or intake, type 1 diabetes mellitus, or taking medications or supplements to aid in weight loss.
Design
This study was a prospective, parallel arm, randomized controlled, trial to test the efficacy of a SmartPhone-based intervention to promote postpartum weight loss. The participants were recruited, screened, and randomized before 7 weeks 6 days postpartum equally to one of two groups: (1) WIC standard care (WIC Moms) and (2) WIC standard care and personalized weight management via a SmartPhone (E-Moms). The WIC Moms (control) group received usual care, that is, standardized advice and services for postpartum nutrition and weight management through their WIC clinic, and they did not receive a dietary prescription or personalized weight management services from the study team.
Weight loss intervention
Participants enrolled in the E-Moms group received a personalized lifestyle intervention through the SmartLoss® application, which has been described previously. 15 In brief, the participants were given access to the SmartLoss SmartPhone application and an iPhone through which a weight loss lifestyle intervention tailored to postpartum women was delivered. The application included near real-time weight and activity monitoring, scheduled delivery of health information, and interventionist feedback.
To track weight and activity, participants were provided a BodyTrace© scale and a Fitbit Zip® accelerometer. Weight and steps were wirelessly transmitted via cellular and Bluetooth technology and plotted on a weight and step graph found in the SmartLoss App and interventionist webportal once daily. This allowed near real-time monitoring by both the participant and interventionist (LAG, Registered Dietitian). The weight graph included an individualized postpartum weight loss zone that provided a weight loss goal of 10% ± 3% of enrollment weight at 16 weeks. 16 Instead of following a caloric prescription, the participants were oriented to the weight graph and counseled to keep their body weight within their ideal weight zone by adjusting energy intake and expenditure accordingly. Body weights above or below the zone for ∼3 consecutive days triggered supportive personalized treatment advice from the interventionist (delivered remotely through phone conversations, email, and text messages).
An individualized step count goal was given to each participant. The initial step count goal was 500 steps/day over the baseline steps/day measured by the SenseWear Armband at week 0. The step goal was then increased 500 steps/day each week. In addition to objective assessment of daily weight and step data, the behavioral intervention was delivered through a series of 16 SmartTips that were automatically sent to the participant on a weekly basis through the SmartLoss application.
The SmartTips included information on diet, physical activity, and behavior modification used in previous large weight loss trials 17,18 tailored to weight loss specifically for the WIC population. Topics included meal planning, incorporation of WIC-approved foods into a healthy diet, healthy eating on a budget, portion control, macro- and micronutrient information, overcoming barriers to lifestyle change, controlling food and hunger cues, mindful eating, methods to reduce stress and improve sleep, and recommendations to increase physical activity. The SmartTips also allowed participants to follow “Mia,” a fictitious new mom through her own postpartum weight loss journey. Each tip concluded with a short interactive activity to assess understanding of the material and provide a list of behavior change goals for the coming week to put the new information into practice.
Clinic measurements
After assessing eligibility at a screening visit, eligible participants were evaluated for outcome assessments at baseline (week 0) and after 8 and 16 weeks of the intervention. Assessments were performed by study personnel according to standard operating procedures at one of the two collaborating WIC clinics or at Pennington Biomedical Research Center. The clinic visits included measurement of height (screening visit only), weight, blood pressure and heart rate, weight and hip circumferences, and body composition and administration of questionnaires.
Anthropometrics
Height was measured in duplicate using a wall-mounted stadiometer. With shoes removed, the participant stood with the head held in a Frankfurt plane by a second study staff member, while the measure was being read.
Weight was measured in duplicate, while participants were wearing underwear or light clothing using a Tanita BWB-800S scale. Weights were not required to be fasting and the date and time of the last meal were recorded.
Study enrollment BMI was calculated at the screening visit as weight (kg)/height 2 (m2). Eligible participants were required to have a BMI 25–40 kg/m2.
Waist and hip circumferences
Waist and hip circumferences were measured with participants wearing underwear and the gulick positioned at the narrowest width of the waist and broadest width of the hips/buttocks, respectively.
Body composition
Body fat percentage was measured in triplicate using a Tanita SC-240 foot to foot bioelectrical impedance analyzer.
Questionnaires
At the screening visit, a lifestyle interview was conducted to identify potential barriers to study participation and a study-specific screening questionnaire assessing socioeconomic status, ethnicity, education, and obstetrical and gynecological history was administered. At week 0 and 16 visits, the Breastfeeding Self-Efficacy Short Form, adapted from the Southampton Women's Survey and CDC Infant Feeding Practices Study, 19,20 assessed influences on breastfeeding decisions, initiation and duration of breastfeeding, duration of exclusive breastfeeding, and timing of introduction of water and complementary fluids. To investigate the association between breast feeding and weight change, women were grouped into those who reported breastfeeding at least 1 week during the study and those who did not breastfeed during the study.
Statistical analysis
The data analysis for this article was generated by a biostatistician (J.H.B.) using SAS/STAT software, Version 9.4 of the SAS System for Windows© (SAS Institute, Inc., Cary, NC). All tests were evaluated using significance level α = 0.05. Both, a completer analysis and an intent-to-treat analysis with baseline values carried forward were performed. Both analyses drew the same statistical conclusion unless otherwise stated.
The primary outcome, change in weight following the 4-month intervention, was investigated in several ways. First, a linear mixed model was used to compare absolute change in weight between the intervention and control groups. A simple model with only fixed effects for treatment group, time, and their interaction was constructed. A random subject effect was included to account for intra-individual correlations over time. Using adjusted means from the model, two-sample t-tests were used to compare the two groups. This same method was used to assess absolute change in secondary outcome body fat percentage, waist circumference, hip circumference, and waist-to-hip ratio.
In addition to comparisons of outcomes between treatment groups, differences in outcomes based on intervention adherence were investigated post hoc. Adherence was defined in terms of the number of days participants weighed themselves and the number of days participants' step counts were recorded from the FitBit Zip. An expected number of days for logged weights and recorded steps was determined for each participant. Based on the distribution of data, women were divided into three adherence groups defined to meaningfully categorize the participants, while maintaining a near balance in adherence group sample sizes. Low adherence for both metrics was defined as meeting ≤40% of these expectations (1–3 days of engagement per week), medium adherence was meeting 40.1%–70% (3–5 days of engagement per week), and high adherence was meeting >70% (5 or more days of engagement per week). To determine overall adherence, these two adherence percentages were averaged. The same analyses described above for treatment groups were applied to these data to compare outcomes among the three adherence groups and the control group.
A power analysis was conducted for the intent-to-treat analysis of the primary outcome variable, weight change (kg) from week 0 to the end of the 4-month intervention. Variance estimate and effect sizes were based on data from our research group as well as published studies. 21,22 With an initial sample size of 20 participants per group and assuming β ≥ 0.80, α = 0.05, two-directional tests, a variance of 6.9 kg, and 10% attrition, a minimum detectable difference of 0.91 kg in weight change between groups and a 6.3 kg minimal detectable difference within each group can be detected.
Results
Five participants (WIC Moms, n = 4 and E-Moms, n = 1) were lost to follow-up resulting in an attrition rate of 12.5% (Fig. 1). Results are presented for the 35 completers and stratified based on intervention adherence.
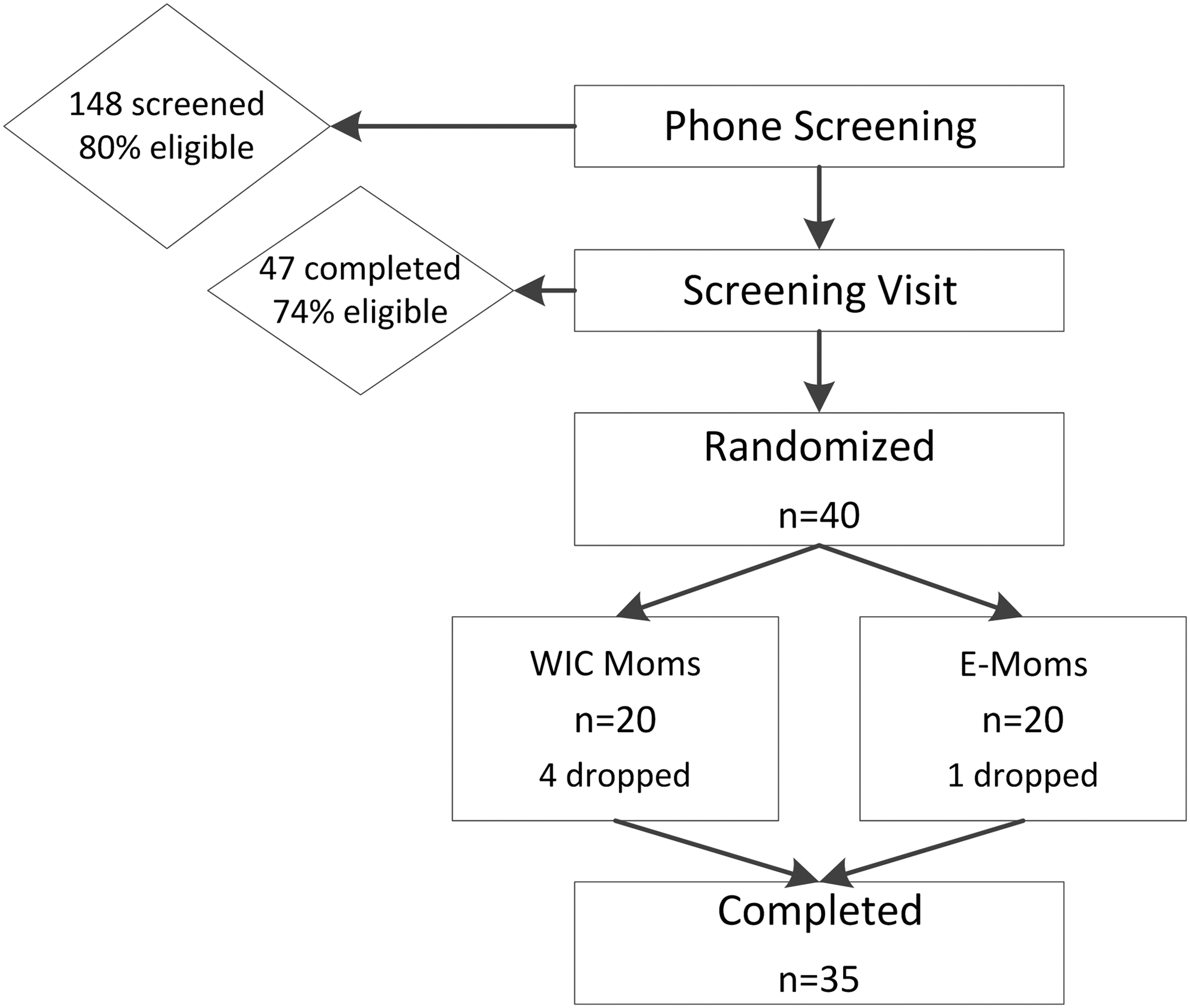
CONSORT diagram. One hundred and forty-eight individuals completed webscreening. Forty-seven individuals came to the clinic and completed a screening visit, and of those, 40 were randomized. Five participants dropped or were lost to follow-up, resulting in 35 participants who completed the study.
Baseline characteristics
Baseline characteristics are summarized in Table 1. Participants predominantly identified as African American (74%) were 26 ± 5.4 years old and had a parity of 2 ± 1. Nineteen participants reported beginning the index pregnancy as obese, 14 as overweight, 1 as normal weight, and 1 unknown. Average self-reported gestational weight gain was 14.5 ± 8.6 kg with 12% gaining below the 2009 Institute of Medicine gestational weight gain guidelines, 20% within, and 68% exceeding. Enrollment BMI at 6–8 weeks postpartum was 32 ± 3 kg/m2 (range: 25.6–37.0 kg/m2) and body fat percentage of 40% ± 4.3%. There were no differences in baseline characteristics between the WIC Moms and E-Moms groups in the completer analysis. Within the E-Moms adherence groups, the high adherence group (n = 5) was significantly older than the low adherence group (n = 7) (32.3 ± 5.4 vs. 23.0 ± 2.7 years; p = 0.03), but neither differed significantly from the WIC Moms group (27.2 ± 6.1 years). All of the individuals who were lost to follow-up were black. Inclusion of these individuals in the intent-to-treat analysis resulted in a significant difference in race distribution when the groups were stratified by adherence.
Continuous values in the table are displayed as mean ± SD and categorical variables as frequency (%).
p-values are used to indicate significant differences between groups.
BMI, body mass index; WIC, women, infants, and children.
Weight change
Weight was maintained during the 16-week study in both groups, and completer analysis suggested no difference (p = 0.10) in weight change between the WIC Moms (1.8 ± 0.9 kg; p = 0.05) versus E-Moms (−0.1 ± 0.9 kg; p = 0.92) groups. Weight change was variable among individuals (range: −8.7 to 10.8 kg; Fig. 2). If weight maintenance was considered to be ±1 kg, 14 (40%) women lost weight, 2 (5.7%) maintained weight, and 19 (54.3%) gained weight. When intervention adherence was stated as a continuous variable (range: 5.4%–94.2%), weight change negatively correlated with adherence (R = 0.52; p = 0.02). When weight change was stratified by adherence as a categorical variable, E-Moms participants with high adherence had a significant reduction in body weight (−3.6 ± 1.6; p = 0.03) when compared to the WIC Moms (−5.4 ± 1.8; p = 0.005). For those participants who had medium and low adherence to the intervention, weight change at week 16 (medium (n = 7): −0.4 ± 1.3 kg; p = 0.75; and low: 2.7 ± 1.3; p = 0.04) did not differ from the WIC Moms group (p = 0.17 and 0.56, respectively). Weight change was different between the high and low adherers (p = 0.004), but not different between the high and medium adherers (p = 0.13). In the intent-to-treat analysis, weight change within the low adherence group was not significant (2.4 ± 1.2; p = 0.05).
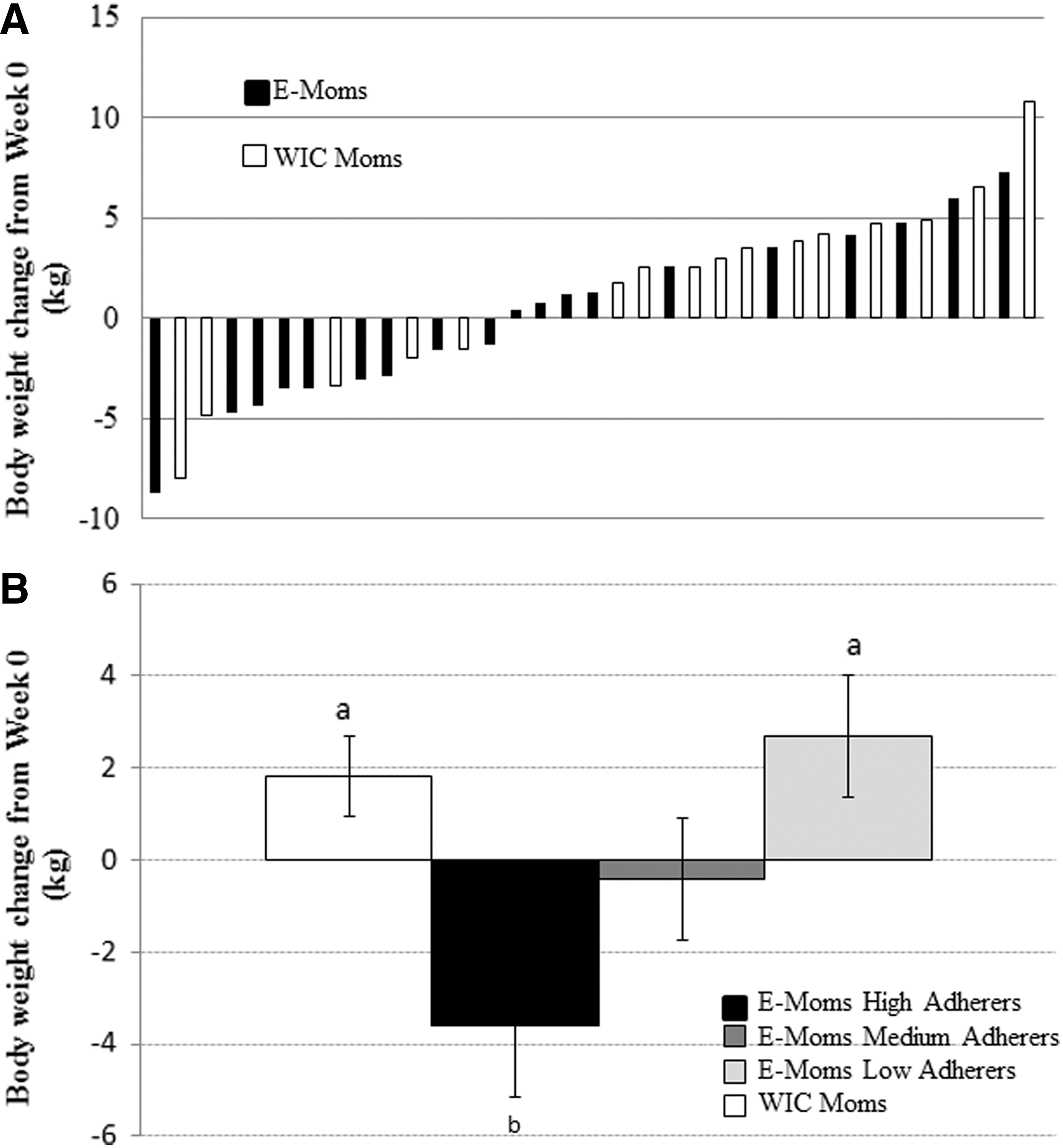
Weight change from baseline (week 0) to week 16.
Indicators of body composition change
In 16 weeks, WIC Moms gained 2.1% body fat (p = 0.002), while the E-Moms group saw no change in body fat percentage (0.03% ± 0.58%; p = 0.96; Fig. 3), and this was different between the groups (p = 0.02). With baseline values carried forward in the intent-to-treat analysis, estimates and standard errors changed slightly (WIC Moms: 1.7% ± 0.54%; p = 0.004 and E-Moms: 0.06 ± 0.54; p = 0.91) and resulted in a significant difference between the WIC Moms and E-Moms groups (1.6% ± 0.77%; p = 0.04). Similar to weight change, body fat percentage decreased in the E-Moms group who had high intervention adherence (−2.5% ± 1.0%; p = 0.02). No change in waist circumference, hip circumference, and waist–hip ratio was seen in any group, except for a decrease in hip circumference in the E-Moms group who had high adherence to the intervention (−5.0 ± 1.7 cm; p = 0.006). Due to slight increases in hip circumference in the low adherence (2.8 ± 1.4 cm; p = 0.06) and medium adherence (0.96 ± 1.44; p = 0.51) groups, change in hip circumference differed between those who had high adherence to the intervention verses those who had low adherence (p = 0.001) and medium adherence (p = 0.01) to the intervention.
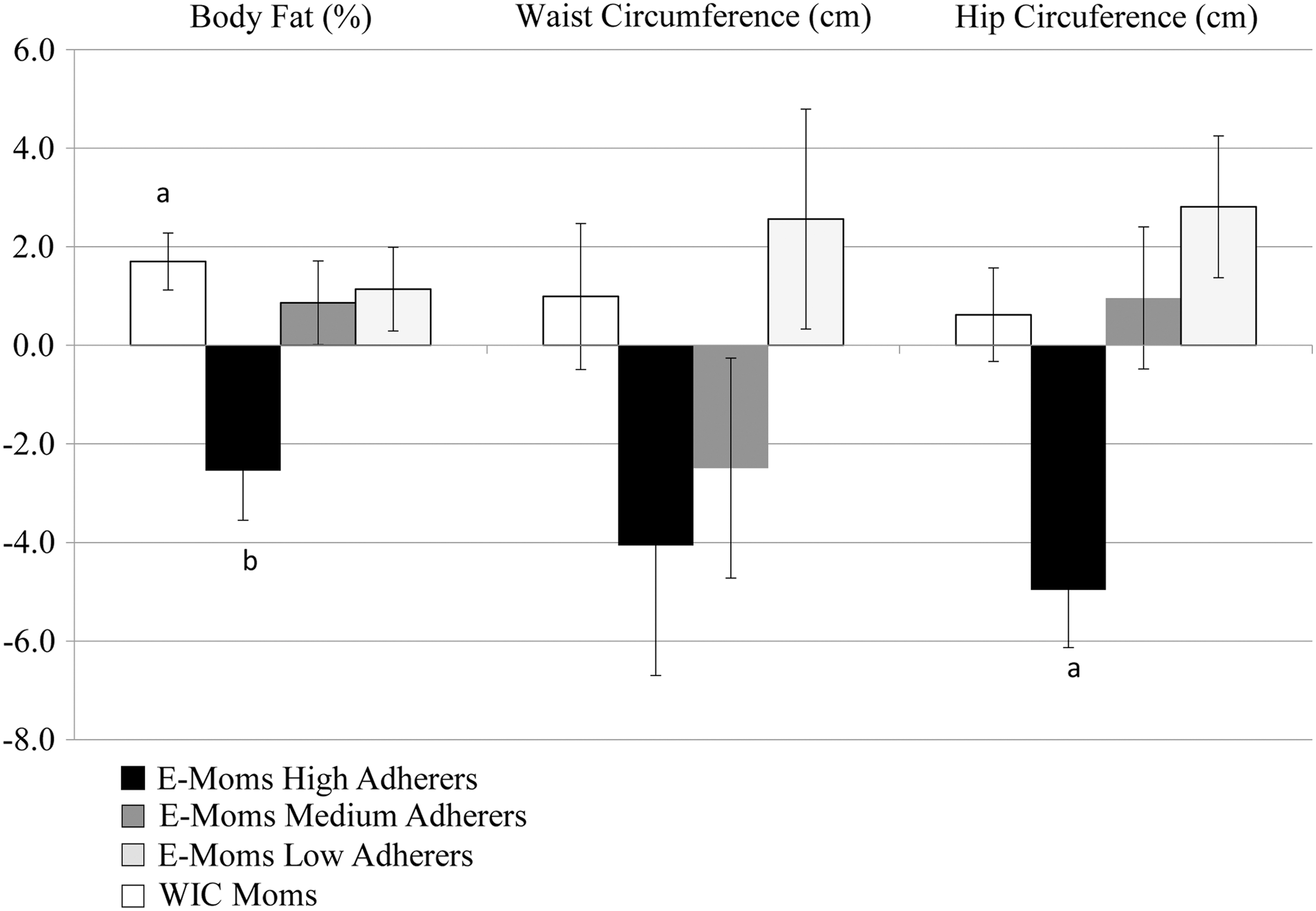
Changes in body composition indicators (% body fat, waist circumference, and hip circumference) from baseline (week 0) stratified by adherence to the E-Moms intervention. Body fat percentage increased significantly from baseline in the WIC Moms group (white bars) and decreased significantly in the E-Moms high adherence group (black bars). Body fat percentage change from baseline was significant between the two groups. Hip circumference decreased from baseline and in relation to the other groups in the high adherence group. Superscripts a or b denote a significant (p < 0.05) within-group change from baseline. Different superscripts denote significant (p < 0.05) between-group differences.
Blood pressure
Systolic and diastolic blood pressure decreased from baseline in both WIC Moms (systolic: −5.3 ± 2.6 mmHg and diastolic: −3.8 ± 2.2 mmHg) and E-Moms (systolic: −5.1 ± 2.4 mmHg and diastolic: −1.9 ± 2.1 mmHg) groups. The change from baseline in systolic (p = 0.96) and diastolic (p = 0.54) blood pressure was not significant between the two groups. In addition, no differences were seen when the E-Moms group was stratified by adherence (p > 0.05).
Breast feeding and weight change
Ten women reported breast feeding for at least 1 week during the study (range: 6–16 weeks) and 25 women did not. Weight change did not significantly differ between those who breastfed during the study (1.75 ± 1.4 kg) and those who did not (0.4 ± 0.9 kg; p = 0.43).
Discussion
Excessive gestational weight gain and postpartum weight retention contribute to increasing BMI of reproductive-age females. 2 Overall, the E-Moms SmartLoss mHealth intervention delivered over 16 weeks was not able to decrease postpartum weight retention in women receiving WIC benefits compared to usual care received through the current WIC program. Other mHealth weight loss interventions have found similar results, reporting a net weight loss of no more than 2 kg after a 6-month health intervention when compared to control. 23 –26 Due to negligible weight change, it is not surprising that body composition indicators and blood pressure were also unaffected.
The majority of participants (71%) did not breastfeed or stopped breastfeeding before study start. Due to study enrollment occurring at 8 weeks postpartum, the intervention did not focus on breastfeeding as most breastfeeding practices were established before study start. The effect of breastfeeding on postpartum weight loss in our study is difficult to isolate from other confounding factors, and thus, the available evidence is heterogeneous and does not show a strong association between breastfeeding and postpartum weight loss. 27 Larger, more robust studies are needed to assess the influence of breastfeeding on postpartum weight loss.
Intervention adherence was variable among participants with objective data transmitted from the body weight scale and accelerometer showing that some individuals were engaged at least 5 days per week and others not engaged at all. The women who had high adherence to self-monitoring did see a modest reduction in their body weight, body fat percentage, and hip circumference throughout the 16-week postpartum intervention when compared to the WIC Moms group who experienced weight gain. Individuals who had high adherence to the E-Moms intervention decreased body fat percentage by 2.5%, which is consistent with other weight loss trials that achieved caloric restriction through diet and exercise modifications. 28,29 Age at study enrollment was the only significant baseline characteristic difference between the adherence groups. However, with the small sample size and limited number of participants with high adherence, discerning demographic differences between the adherence groups is limited. In addition, other behaviors and characteristics not assessed during the study could further explain adherence and outcome differences.
Whether deployed in an mHealth or in-person intervention, increased self-monitoring, including weight and physical activity monitoring, has been associated with increased weight loss and successful weight management. 30 –34 As expected, similar to self-monitoring, an increased intervention engagement is associated with an increased weight loss. 35 –37 Despite near real-time feedback and increased frequency of communication and access to health information, mHealth interventions have the potential to be more passive than in-person interventions. Participants may more easily disengage by ignoring remote communication attempts (i.e., texts, emails, and phone calls) and decrease adherence to recommendations without the accountability of a face-to-face intervention, especially as the study progresses. 38,39 mHealth interventions may struggle to provide a dynamic intervention that motivates and encourages the participant to meet goals and remain engaged. 40 –42 While barriers to adherence and participation to the E-Moms intervention were not directly assessed, independent qualitative studies report barriers such as lack of knowledge and skills (which alludes to issues of health disparities), lack of child care or presence of other family duties, lack of time or work schedules, inadequate access to the needed foods, and stress. 43,44 Indeed, it is likely that many, if not all, of these factors may have impacted the desire and ability of E-Moms participants' to participate fully in the intervention. As a result, mHealth research and developers are charged to develop weight management interventions that integrate pillars of successful weight management interventions (e.g., self-monitoring and frequent, near real-time personalized feedback) with consistent motivation and reasons for engagement.
Pertinent to the WIC population who face health disparities, behavior change interventions should be more carefully developed with input from these groups to help overcome many of the stated barriers. Strategies to improve intervention engagement may include the use of peer-led programs, addition of a gamification component, deepening staff and participant relationships with video conferencing or in-person activities, 45 use of social networking or involvement of family and/or friends to increase social support, 43,46 delivery of participant-centered nutrition and health information, 47 and additional assistance with recommended foods for weight loss such as fruits, vegetables, and portion-controlled foods. Herring et al. 48 deployed a similar, yet successful (−3.6 kg difference between treatment and usual care), technology-based weight loss intervention in urban low-income mothers, which engaged participants via social networking (Facebook support group), and provided an incentive to respond to health coaches' text by conducting raffles for gift certificates on a monthly basis. As observed in the current trial, intervention adherence led to greater weight loss.
While intensive, in-person lifestyle interventions are the most effective behavioral weight loss treatment, frequent in-person counseling led by a trained interventionist is not always possible. 49 To decrease the burden on both the clinician and the client, the efficacy of alternative modes of weight management intervention delivery such as mHealth-based interventions for pregnant and postpartum moms are being tested. 50,51 In this pilot and feasibility study, we successfully partnered with local WIC clinics and deployed a mHealth weight management intervention. In a population that is traditionally difficult to recruit and retain, 50,52 40 women were enrolled within 1 year and 88% of the participants completed the 16-week study (95% retention in the intervention group). The increased retention in the E-Moms group may have been a result of an increased contact with the participants by nature of the study design, and the majority of the participants in the intervention were loaned a SmartPhone that provided a consistent mode of contact. In most cases, contact with the WIC Moms group was lost due to changes in address and phone numbers, and women not returning to the local clinic for routine WIC appointments, preventing follow-up. Similar retention and engagement challenges have been reported by Foster et al., including gaps in communication due to monthly renewal of limited cellular plans and lost cell phones. 53
WIC serves ∼2 million women of childbearing age in the United States 54 and the average interpregnancy interval in the United States is 34 months. 55 Therefore, the postpartum period of one pregnancy is also the prepregnancy period of another. With children eligible for WIC benefits until their fifth birthday, the likelihood that a woman will become pregnant again before ending WIC benefits with her first child is high. Together with the observation that without intervention mothers gained 4–6 kg in the first year postpartum, 56,57 WIC is an ideal setting to integrate weight management programs aimed to attenuate the weight gain observed during the reproductive years, while improving preconception health of the mother. A programmatic shift to focus on weight management would positively impact the health of more than just the mother as the mother's weight status directly influences the health of her developing fetus 58 –60 and her family. 61,62 Collaboration and increased communication (e.g., shared electronic medical records) with other subsidized programs such as the Supplemental Nutrition Assistance Program, Medicaid, and Healthy Start would improve the continuum of care and ease the financial and logistical burden of implementing a weight management program in WIC, potentially improving the health and well-being of millions of Americans.
Conclusions
Overall, the E-Moms SmartLoss mHealth intervention was not able to decrease postpartum weight retention in women receiving WIC benefits compared to usual care received through the current WIC program. However, the intervention was effective in those women who were adherent to the intervention. Therefore, further development of mHealth lifestyle interventions to improve adherence is needed. Interventions that successfully engage WIC participants may complement standard of care and facilitate weight loss during the postpartum period and reduce postpartum weight retention. Given that this is also the likely interpregnancy interval for subsequent pregnancies, further research is needed to improve individual engagement and adherence to mHealth interventions for low socioeconomic women, to improve the health of millions served by WIC.
Footnotes
Acknowledgments
The authors wish to thank the Louisiana Department of Health and Hospitals; Louisiana Woman, Infants, and Children; Emily Fontenot and all of the staff at Capitol City Family Health Clinic and Martin Luther King Community Center; and Melissa Guillory, Donna Richards, and all the staff at Wooddale WIC Clinic for welcoming our staff into the WIC clinics and their unwavering support of the study. Their selfless service to others is evident in all that they do. This work was supported by the United States Department of Agriculture through UCLA Small Grants Program (UCLA Subaward No. 1920 G QA123; L.M.R.) and support of LAG by T32DK064584. This work was supported, in part (J.H.B.), by 1 U54 GM104940 from the National Institute of General Medical Sciences of the National Institutes of Health, which funds the Louisiana Clinical and Translational Science Center.
Author Disclosure Statement
Drs. Gilmore, Myers, Klempel, and Burton and Ms. Sutton report no conflicts of interest. SmartLoss is a registered trademark of the Louisiana State University System, with the trademarked approach having been developed by Drs. Martin and Redman.