
Abstract
Importance:
Patients with acute myocardial infarction (MI) and nonobstructive coronary artery disease (CAD) have an elevated cardiac event rate, suggesting that these patients may benefit from cardiac medication.
Objective:
We evaluated the rates of cardiac medication use 3 months before angiography and 3 months following clinically indicated angiography for MI in patients with no CAD, nonobstructive CAD, and obstructive CAD. We also examined the sex differences in cardiac medication use 3 months following angiography in patients by extent of angiographic CAD.
Methods:
We studied patients ≥20 years old with MI undergoing coronary angiography in British Columbia, Canada, from January 1, 2008, to March 31, 2010 (n = 3,841). No CAD, nonobstructive CAD, and obstructive CAD were defined as 0%, 1% to 49%, and ≥50% luminal narrowing in any epicardial coronary artery, respectively. Medication use, 3 months before and 3 months following angiography, was obtained through British Columbia PharmaNet for angiotensin-converting enzyme inhibitors (ACE-Is), angiotensin receptor blockers (ARBs), calcium channel blockers (CCBs), beta-blockers, statins, and antiplatelet agents. Optimal medical therapy (OMT) was defined as filled prescriptions for all three: ACE-Is/ARBs, beta-blockers, and statins.
Results:
Following angiography, in all medication categories except CCBs, patients with no CAD and nonobstructive CAD had significantly lower rates of prescriptions filled than patients with obstructive CAD (all p < 0.001). After adjusting for age and prior medication use, patients with nonobstructive CAD were still less likely to receive these medications than patients with obstructive CAD, including OMT with an odds ratio = 0.25 (95% confidence interval: 0.18–0.36). There were no significant sex differences in medication use 3 months postangiography.
Conclusions:
In post-MI patients, medication use following angiography is significantly lower in nonobstructive CAD than obstructive CAD at 3 months. While sex was not an independent predictor of medication use 3 months post-catheterization, future studies should explore methods of improving medication use in both females and males with nonobstructive CAD post-MI.
Introduction
P
These studies did not exclude patients with nonobstructive coronary artery disease (CAD). Up to 10% of women and 6% of men with MI have nonobstructive CAD on coronary angiography. 8 Potential etiologies of MI in these patients would include coronary vasospasm, embolism, unidentified plaque rupture, 9,10 or missed spontaneous coronary artery dissection. 11
Despite the finding of nonobstructive CAD, recent literature suggests that these patients have a threefold increased risk of all-cause mortality at 8.5 years, suggesting that these patients may benefit from cardiac medication. 12 The 2014 AHA/ACC guidelines for the management of patients with acute coronary syndrome assign a class I indication to beta-blockers, ACE-Is, and statins post-MI, irrespective of anatomy found on angiography. Furthermore, most of these treatments are recommended in the first 24 hours before angiography being performed. 3 As well, the CCS 2016 guidelines for the management of dyslipidemia recommend the use of a statin in all patients with documented coronary disease by angiography with greater than 10% stenosis. 13
Scant literature exists examining medication use in patients with nonobstructive CAD compared with obstructive CAD post-MI. Furthermore, these existing studies are limited, in that they did not differentiate stable angina from MI, 14 used older data, 15 and/or did not report on medication use by sex. 14,16
To provide further insight into the pharmacologic treatment of patients with no CAD, nonobstructive CAD, and obstructive CAD in British Columbia (BC), Canada, we evaluated medication use 3 months before and 3 months after diagnostic coronary angiography during the MI admission for males and females stratified by extent of CAD.
Methods
Study population
We studied all BC residents ≥20 years old admitted to hospital with MI diagnosis and undergoing coronary angiography from January 1, 2008, to March 31, 2010. Patients with known CAD consisting of obstructive CAD on prior angiography were excluded. Figure 1 illustrates patient selection and composition of the study cohort. Data were obtained from Cardiac Services BC (CSBC) Registry (cardiac procedures and patient's clinical and demographic characteristics) with linkage to the BC Hospital Discharge Abstract Database (hospital admissions), BC Vital Statistics (death records), and BC PharmaNet (prescriptions for medications dispensed). Medication use focused on cardiac medications, including ACE-Is, ARBs, calcium channel blockers (CCBs), beta-blockers, statins, and antiplatelet agents, obtained 3 months before angiography and 3 months following angiography.
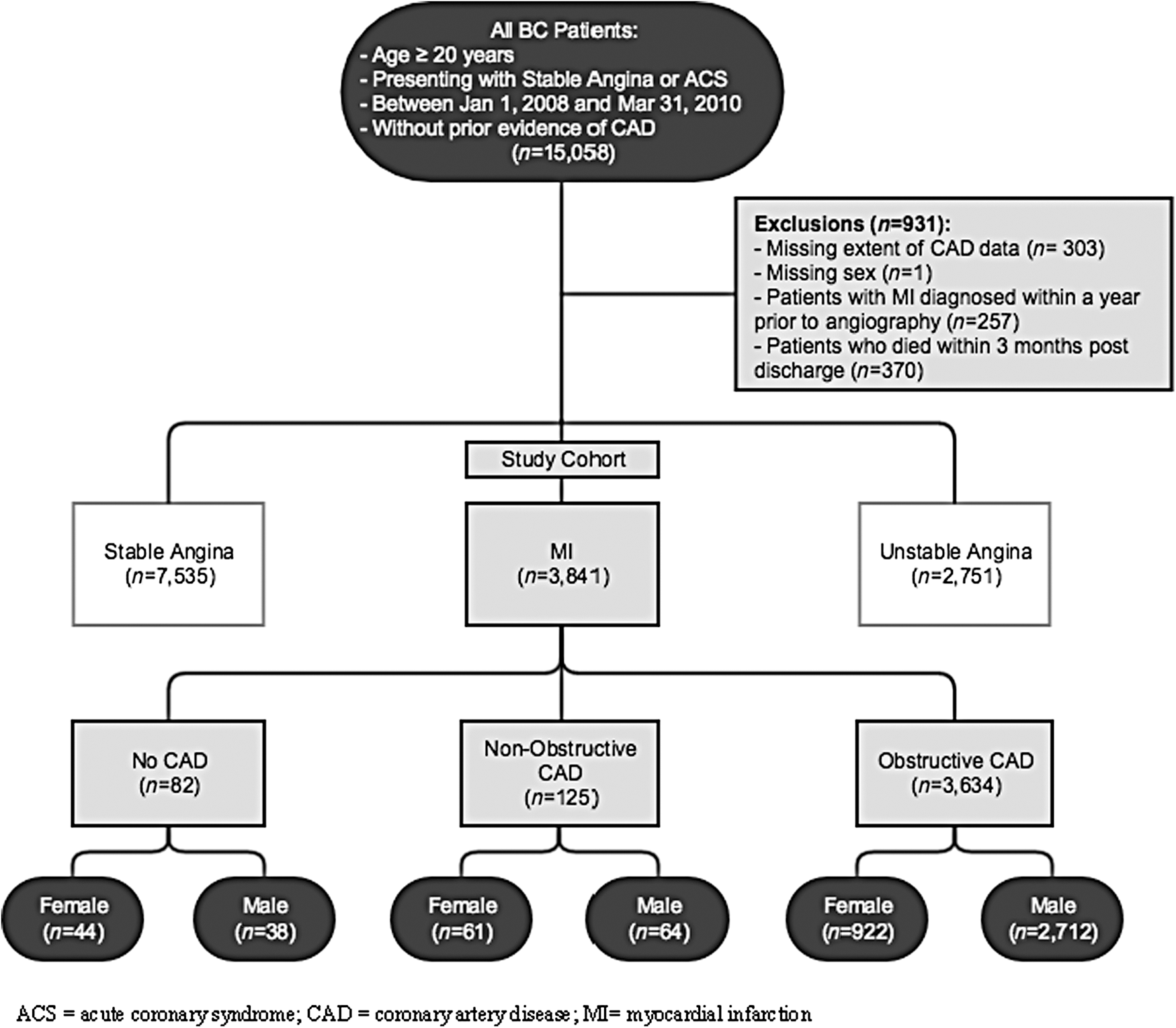
Patient selection and study cohort.
Ethics approval was obtained from the University of British Columbia Clinical Research Ethics Board.
Definitions
MI was defined as non-ST elevation or ST elevation myocardial infarction according to the Universal Definition of Myocardial Infarction. 17 No CAD, nonobstructive CAD, and obstructive CAD were defined as 0%, 1% to 49%, and ≥50% luminal narrowing in any epicardial coronary artery, respectively, as reported in the CSBC Registry. We chose to include the no CAD group as rates of recurrent MI in patients with no CAD due to the fact that there is a threefold increase compared with patients with no CAD, but without a prior MI. 12 The level of stenosis was defined by the angiographer at the time of the angiogram with no quantitative core laboratory assessment. History of CAD was defined as a previous diagnosis of obstructive CAD on prior angiography. Prior medication use was defined as having at least one prescription filled within 3 months before angiography. Likewise, postmedication use was defined as a filled prescription within 3 months postangiography discharge. Optimal medical therapy (OMT) was defined as filled prescriptions for all three medications, including ACE-Is/ARBs, beta-blockers, and statins within the specified time frame. We have used the term OMT for consistency between 3 months before angiography and 3 months following angiography for the purposes of comparison between the no CAD group, nonobstructive CAD group, and obstructive CAD group. We chose to evaluate OMT as recent guidelines support significant improvements in long-term mortality, morbidity, and cost-effectiveness post-MI with the use of these medications. 3 De novo medication use describes patients without medication use 3 months before angiography, but starting within 3 months postangiography. Aspirin use was not evaluated because it is commonly obtained without a prescription (i.e., over the counter).
Statistical analyses
Categorical baseline characteristics were summarized as frequencies and percentages. Chi-square or Fisher's exact tests were used for the comparison between sexes and between extent of CAD for categorical variables. Observations of 5 or less counts were not reported for patient confidentiality. Age was summarized using mean and standard deviation (SD) and tested for differences with Student's t-test. Differences by sex and extent of CAD in prior, post, and de novo medication use were tested using chi-square tests. Sex, extent of CAD, and the interaction between sex and extent of CAD on medication use postangiography for OMT, ACE-Is/ARBs, beta-blockers, and statins were modeled with logistic regression (Model 1). The interaction term was eliminated from the model if it was not statistically significant (p > 0.05), with sex and the extent of CAD remaining as main effects. Multivariable logistic regression modeling with clinically selected covariates, age and prior medication use, was utilized to explore, in greater depth, the impact of sex and extent of CAD on postmedication use (Model 2). Age was categorized as [20–55], [56–65], [66–75], and >75 years since the linearity assumption for age as a continuous covariate was not satisfied. Estimated odds ratios (ORs) and confidence intervals (95% CIs) were reported for the factors in the logistic models. Statistical analyses were performed using SAS software, version 9.4 (Cary, NC).
Results
Patient selection and study cohort
From the 15,058 BC patients who underwent angiography from January 1, 2008, to March 31, 2010, 931 (6%) cases were excluded for missing angiographic details (n = 303), sex not reported (n = 1), MI diagnosis within a year before angiography (n = 257), and death within 3 months postdischarge date (n = 370). Of the remaining 14,127 patients, we identified 3,841 MI patients with no prior diagnosis of CAD. The flowchart describing the derivation of the study cohort is shown in Figure 1.
Baseline characteristics
Of the 3,841 patients, 94.6% had obstructive CAD, 3.3% had nonobstructive CAD, and 2.1% had no CAD. Nearly 4.3% of females had no CAD compared with 1.4% of males; females also had a higher proportion of nonobstructive CAD compared with males (5.9% vs. 2.3%); males had a significantly higher proportion of obstructive CAD compared with females (96.4% vs. 89.8%) (p < 0.0001). Baseline characteristics for the study cohort, classified by extent of CAD and by sex, are shown in Table 1. Baseline characteristics by CAD status are described in Table 2. Patients with obstructive CAD were older and had more Chronic Obstructive Pulmonary Disease (COPD) and diabetes than patients with no CAD or nonobstructive CAD. In Table 1, females were significantly older than males in all CAD categories: [mean difference (SD): no CAD 17.0 (3.0); nonobstructive CAD 9.3 (2.0); and obstructive CAD 6.4 (0.5), all p < 0.001]. In the obstructive CAD group, females had a significantly higher rate of diabetes (22.8% vs. 18.0%, p = 0.001) and heart failure (9.9% vs. 6.4%, p < 0.001). In the nonobstructive group, females had a higher rate of heart failure (13.1% vs. ≤7.8%, p = 0.02), although overall counts were low. In all three categories, females had higher rates of hypertension than males.
Fisher's exact test.
No testing done since both cell sizes are 0.
CAD, coronary artery disease; COPD, chronic obstructive pulmonary disease; CVA, cerebrovascular disease; HF, heart failure; MI, myocardial infarction; PVD, peripheral vascular disease; SD, standard deviation.
Medication use
Medication use 3 months before and 3 months postangiography is reported in Tables 3 and 4, respectively. Before angiography, nonobstructive CAD patients had the highest rates of prescription use for OMT (11.2% for nonobstructive CAD compared with 4.2% for obstructive CAD and ≤5% for no CAD, p < 0.001), ACE-Is/ARBs (36.8% for nonobstructive CAD compared with 25.6% for obstructive CAD and 34.1% for no CAD, p = 0.005), and statins (28.8% for nonobstructive CAD compared with 17.2% for obstructive CAD and 22.0% for no CAD, p = 0.002). There was no significant difference in prescribing rates by extent of CAD for beta-blockers, CCBs, and clopidogrel. When examined by sex, females had significantly higher rates of prescriptions filled for beta-blockers irrespective of extent of CAD, for ACE-Is/ARBs in obstructive and nonobstructive CAD, and for statins, CCBs, and OMT among patients with obstructive CAD, compared with males (Table 3).
ACE-I, angiotensin-converting enzyme inhibitor; ARB, angiotensin receptor blocker; CCB, calcium channel blocker; OMT, optimal medical therapy.
Following angiography, in all medication categories except CCBs, patients with no CAD and nonobstructive CAD had significantly lower rates of prescription use than patients with obstructive CAD (all p < 0.001). Regarding sex differences, only females with no CAD continued to have a higher rate of prescriptions filled for ACE-Is/ARBs and beta-blockers (Table 4). Among patients with obstructive CAD, males had significantly higher rates of prescriptions filled for OMT and statins, while females in this group filled more prescriptions for CCBs. Among patients with nonobstructive CAD, males filled a prescription for clopidogrel more frequently than females.
De novo medication use 3 months postangiography is shown in Figure 2. More patients with obstructive CAD initiated medication use than patients with no CAD or nonobstructive CAD (all p < 0.0001). In the obstructive CAD group, more males than females initiated ACE-Is/ARBs, beta-blockers, statins, and OMT. In the nonobstructive group, more males than females initiated ACE-Is/ARBs (p = 0.05). In both the obstructive CAD and nonobstructive CAD groups, more females than males initiated CCBs (data not shown). No sex differences were found in the no CAD group in any of the medication groups.

De novo medication initiation in MI patients 3 months postcatheterization by extent of CAD and sex.
In the logistic model for the odds of medication use postangiography, the interaction term between sex and the extent of CAD was not significant in any of the medication groups, with the exception of beta-blockers (p = 0.04), Model 1. After adjusting for age and prior medication use (Model 2), the interaction term for the use of beta-blockers was not significant at the 0.05 level and hence was removed from the model. Odds ratios shown in Figure 3 indicate no sex differences in any of the medication groups, neither in Model 1 nor in Model 2. The odds of medication use in patients with no CAD and nonobstructive CAD were significantly less for all medications, including OMT, compared with patients with obstructive CAD (OMT OR = 0.11 [95% CI: 0.07–0.18] for no CAD vs. obstructive CAD and OR = 0.25 [95% CI: 0.18–0.36] for nonobstructive CAD vs. obstructive CAD) (Fig. 3, Model 2).
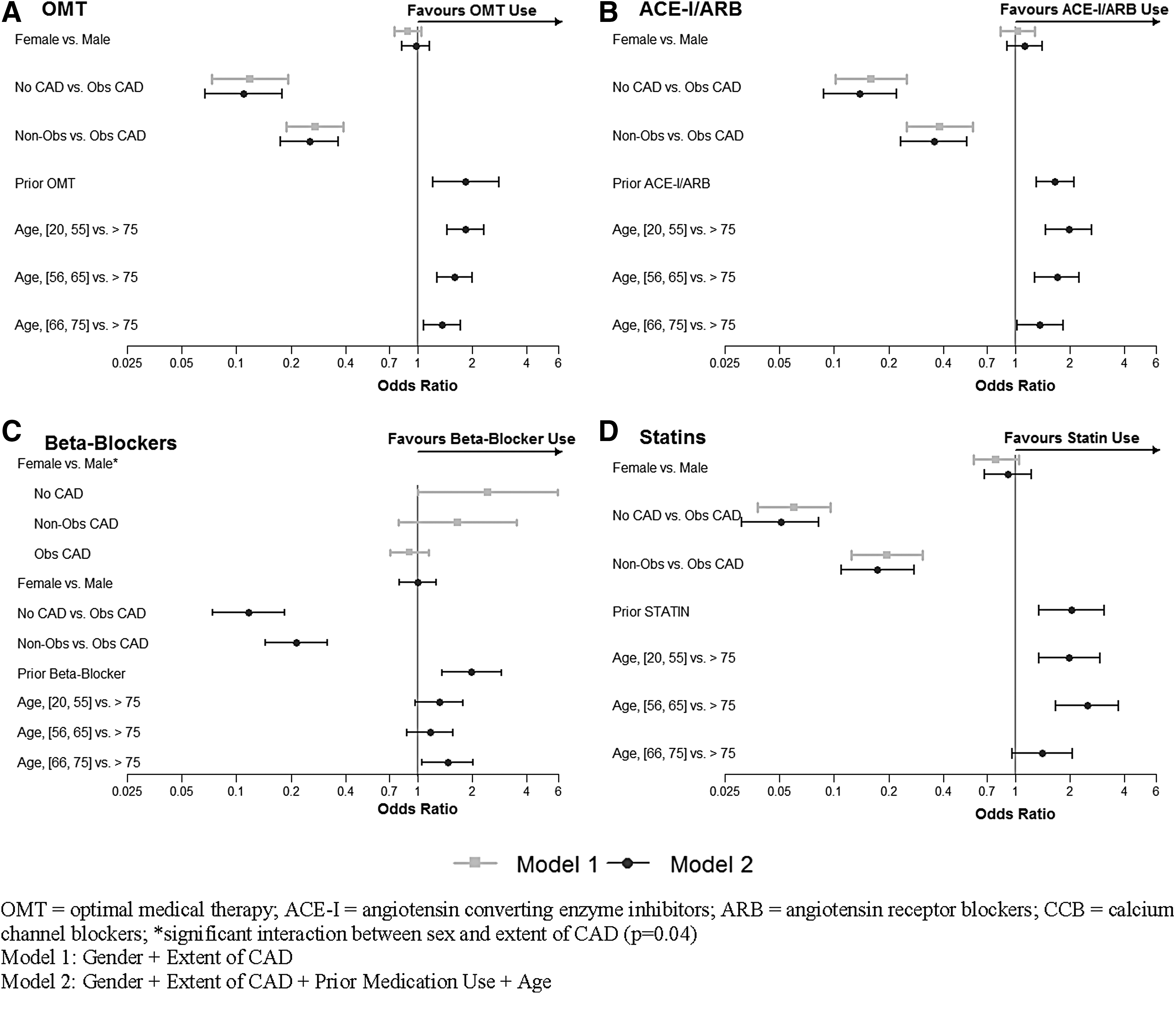
Odds ratios (95% CI) for medication use in MI patients within 3 months postcatheterization.
Discussion
In patients undergoing coronary angiography for MI, medication use following angiography is significantly lower in nonobstructive CAD with only 50.8% of females and 46.9% of males prescribed OMT compared with 76.4% of females and 79.0% of males with obstructive CAD at 3 months. Furthermore, only 75.4% of females and 79.7% of males with nonobstructive CAD were prescribed statins compared with 93.6% of females and 95.4% of males with obstructive CAD. Patients with obstructive CAD were more likely to initiate therapy de novo in all medication categories compared with those with nonobstructive CAD. Regarding sex differences in prescription use post-MI, there were no significant differences between males and females after adjustment for confounders such as age and prior medication use.
Prior studies found lower rates of prescription use post-MI for nonobstructive CAD; however, these studies suffer from important limitations. Maddox et al. examined prescription rates among 1,489,745 patients undergoing cardiac catheterization in 786 U.S. centers between 2004 and 2007. 14 They found lower rates of statin use (60% in nonobstructive CAD vs. 80.3% in obstructive CAD) and after multivariable adjustment, nonobstructive CAD patients remained significantly less likely to receive aspirin (OR = 0.37), statins (OR = 0.45), ACE-Is/ARBs (OR = 0.83), and beta-blockers (OR = 0.46) compared with obstructive CAD patients. Maddox et al. did not differentiate stable angina from MI and did not report on medication use by sex. Rossini examined medication use at discharge in patients with an acute coronary syndrome. 16 They reported lower rates of prescription use in nonobstructive CAD compared with obstructive CAD with 66.5% versus 85.9% receiving a beta-blocker, 50% versus 71.4% receiving an ACE-I/ARB, 80.4% versus 90.2% receiving a statin, and 89.2% versus 99.4% receiving aspirin, respectively. They did not report on sex differences in medication use. Ramanath conducted a cohort study of 2,264 patients who were followed for 6 months posthospitalization after an acute coronary syndrome. 15 They reported less prescription use of beta-blockers, aspirin, and statins in patients with nonobstructive CAD compared with obstructive CAD and did not find any sex differences in medication use. Their study was limited, in that it reported data only up until 2004. Reynolds et al. suggest that regardless of the no CAD or nonobstructive CAD shown on angiography, all MI patients should be on secondary prevention due to the fact that 40,000–100,000 women and 20,000–50,000 men have an MI annually in the no-CAD and nonobstructive CAD groups, respectively. 9 Furthermore, the AHA/ACC 2014 guidelines and CCS 2016 guidelines support the use of beta-blockers, ACE-I, and statins, irrespective of coronary anatomy post-MI. 3,13
Our results add to the findings from prior studies, in that we provide a contemporary analysis of a large Canadian cohort of both males and females with no CAD, nonobstructive CAD, and obstructive CAD. Our findings confirm the lower use of medications in both males and females with nonobstructive CAD. Possible reasons for this include under-recognition of the importance of treating nonobstructive CAD post-MI. While there were no sex differences after adjustment for age and prior medication use, de novo initiation was much greater in men than women for the obstructive group and borderline significant in the nonobstructive group, with the exception of Beta-Blockers. The lack of significant sex differences in medication use in general may indicate an increased awareness that women with MI have adverse outcomes similar to and, in some cases, worse than men. 18
Limitations
Our study has several limitations. First, it is known that the rates of the comorbidity data such as hyperlipidemia and smoking are often under-reported in administrative data and thus are not reported in our article. 19 Second, in instances where the number of cases was <5 per comorbidity, the true proportions are known; however, it is not possible to report those data due to confidentiality reasons. We agree that it is not ideal that we have such low numbers in a few categories. Third, medication use is presumed given the prescription for that medication was filled; however, we were unable to test or report on actual use, let alone adherence. Furthermore, we were unable to report on or account for contraindications to medication use. Nevertheless, it is unlikely that medication use, given the prescription was filled, differs by sex. Fourth, we did not report on aspirin as it is predominantly an over-the-counter medication in BC rather than a prescription. Fifth, only patients who survived to 3 months postangiography were included in our analysis to allow sufficient time to fill a prescription. Last, we acknowledge that our findings are based on Canada's universal healthcare system and hence our findings may not be generalizable to other countries where there may be more barriers to access to medications compared with Canada.
Conclusion
In post-MI patients, medication use following angiography is significantly lower in nonobstructive CAD than obstructive CAD at 3 months. While sex was not an independent predictor of medication use 3 months postcatheterization, future studies should explore methods of improving medication use in both women and men with nonobstructive CAD post-MI.
Footnotes
Author Disclosure Statement
No competing financial interests exist.