
Abstract
Background:
We aimed to quantify the time to diagnosis among women with endometriosis in the United States (US) and to identify patient- and physician-related factors affecting diagnostic delay.
Patients and Methods:
An online cross-sectional survey was conducted from August 6, 2012, through November 14, 2012. Respondents aged 18–49 years who reported a physician's diagnosis/suspicion of endometriosis within the previous 10 years were included. Endometriosis-related symptoms and diagnostic history were captured and summarized. Univariate analyses identified factors associated with time from symptom onset to first consultation and from first consultation to diagnosis.
Results:
Of 638 respondents included, most (56%) reported seeking care for at least one of the following symptoms: menstrual pain (31.6%), nonmenstrual pain (27.3%), and pain during sex (7.5%). Most diagnoses (84%) were made by obstetricians/gynecologists; 49% of diagnoses were surgical versus 51% nonsurgical. Mean time from symptom onset to diagnosis was 4.4 years. Mean time to first consultation was shorter among women aged 40–49 years versus those aged <18 years (14.2 vs. 43.5 months; p < 0.0001) and those consulting for symptoms versus routine/other care (27.9, 24.9, and 28.4 months for menstrual pain, nonmenstrual pain, and pain during sex, respectively, vs. 61.4 months; all p < 0.01). Mean time from first consultation to diagnosis was shorter among women aged 40–49 years versus those aged <18 years (12.4 vs. 34.5 months; p = 0.0009) and those diagnosed by obstetricians/gynecologists versus nonobstetricians/gynecologists (21.5 vs. 40.3 months; p = 0.041).
Conclusions:
Time to endometriosis diagnosis appears to have shortened in the US. Better patient and physician education regarding symptomatology may contribute to further gains.
Introduction
E
Globally, the delay in diagnosing women afflicted with endometriosis is currently estimated at ∼5–10 years. 6 –10 In the United States (US), the average length of time to establish an endometriosis diagnosis was estimated at ∼12 years based on a survey conducted in 1995 2 and at ∼9 years based on analyses of the 1998 Endometriosis Association Survey. 11,12 These estimates indicate that time to diagnosis is quite long and one of the goals of this study was to determine if this lengthy delay still exists today. Because endometriosis is associated with decreased health-related quality of life, increased healthcare resource utilization, and loss of work productivity, 6,8,13 –15 longer delay in diagnosis may lead to unnecessarily prolonged patient suffering and to greater socioeconomic cost.
To accelerate diagnosis, a number of investigators have begun to characterize the factors that contribute to lengthy delay. For example, Greene et al. 12 showed that US patients who were adolescents at symptom onset took 3 times longer to receive a diagnosis versus those with adult onset; they also showed that patients who sought care from a generalist experienced a 30% longer delay in receiving a diagnosis versus those who saw a gynecologist. 12 Other factors, including key symptoms that lead women to seek medical attention, remain less well studied.
Guidelines for the diagnosis and management of endometriosis have begun to emphasize the role of noninvasive methods, including advanced imaging techniques, 5,16 but the impact of this shift in diagnostic algorithm on time to diagnosis has not been assessed. Understanding the factors contributing to delays in diagnosis may lead to changes in current clinical practice patterns, patient awareness/education and identify key areas for further improvement.
The objectives of the current study were (1) to assess the duration of time to a diagnosis of endometriosis among patients in the US from 2002 to 2012 and (2) to identify key patient- and physician-related factors that affected the duration of time to diagnosis during that period. Patient-related factors assessed included sociodemographic characteristics, endometriosis-related symptom experience, and diagnostic experience; physician-related factors included clinical specialty and diagnostic methods employed. Overall diagnostic delay was defined as time from symptom onset to the diagnosis of endometriosis. To better differentiate patient-dependent factors from physician-related factors, we considered the contributions to overall delay from two separate intervals: the time from symptom onset to first consultation with a medical practitioner and the time from first consultation until diagnosis.
Patients and Methods
Study design
Details on study design and survey content were described in previous reports. 17,18 We conducted a cross-sectional online survey of US resident women aged 18–54 years from August 6, 2012, through September 14, 2012. The survey was designed by the investigators and administered through Harris Interactive, Inc. (New York, NY), using previously described methodology. 17 –20 The study was reviewed and approved by the Copernicus Group Institutional Review Board (Durham, NC), and all survey respondents provided informed consent to be included in the study. To protect subject confidentiality, the survey was conducted using secure servers, and data were deidentified before analysis.
For the current study, survey participants were recruited primarily from three actively managed market research panels: Harris Poll Online (Harris Interactive, Inc., NY, NY), Global Market Insights (Lightspeed Research, Warren, NJ), and e-Rewards Opinion Panel (Research Now Group, Inc., Plano, TX). A subset of respondents was recruited from a specifically targeted sample of women who had indicated being diagnosed with endometriosis and/or uterine fibroids (UF) during previous research. 17,18
Data analyses of this survey that focused on examining the prevalence and symptomatic burden of diagnosed endometriosis in comparison with women with no diagnosis of endometriosis were reported previously. 17 The current analysis included those respondents who reported a physician's diagnosis of endometriosis only. Additional inclusion criteria were age 18–49 years at the time of survey administration and history of endometriosis within the past 10 years. The age range was restricted to focus primarily on premenopausal women, and the past 10-year history of endometriosis requirement was imposed to reduce the possibility of recall errors associated with responses to events from the more distant past. 21
Survey contents
The survey was divided into two main parts: an eligibility screening questionnaire and the main survey of endometriosis-related outcomes. The screening questionnaire collected information on sociodemographic characteristics (age, race/ethnicity, geographic region, education, income, and insurance status) and contained items to identify and qualify respondents based on endometriosis-related symptoms and diagnosis.
Survey participants were first asked whether they had ever experienced any of the endometriosis-related symptoms listed in Supplementary Box S1 (Supplementary Data are available online at
The main survey collected detailed information on each patient's history (pre- and postdiagnosis and within 1 month of completing the survey) regarding symptom severity; medical, treatment, and surgical history; quality of life and health productivity losses related to endometriosis. The main survey also contained several questions used to assess factors potentially affecting the length of time to a diagnosis of endometriosis.
We assessed both the time from symptom onset to first physician consultation and the time from first consultation to diagnosis by asking the questions, “How long after you first noticed your symptoms did you first visit a physician to discuss them?” and “How long after you first mentioned your symptoms to a physician were you diagnosed with endometriosis?” Overall diagnostic delay was defined as the time from symptom onset to diagnosis of endometriosis and was calculated as the sum of the two components. We also assessed overall diagnostic delay independently by asking the questions, “How long ago did you first experience any endometriosis symptoms?” and “How long ago were you first diagnosed with endometriosis?”
Symptoms that led respondents to consult with a physician were assessed by asking, “What was the primary symptom for which you sought medical help?” Symptom burden was assessed by asking, “How would you categorize the overall severity of your endometriosis at the time of diagnosis?” Responses of mild, moderate, or severe were allowed. Medical history, surgical history, and testing related to endometriosis were assessed with the question, “Thinking about the time before you were diagnosed with endometriosis, how many times (in total) did you do each of the following to seek symptom relief?” Potential responses included, visited a doctor, was hospitalized, had a surgical procedure, had a diagnostic procedure (e.g., ultrasound, magnetic resonance imaging [MRI]), and went to the emergency room.
Diagnosing physician specialty was ascertained with the question, “What was the specialty of the physician who formally diagnosed your endometriosis?” Potential responses included primary care physician, obstetrician/gynecologist (OB/GYN), infertility specialist, general surgeon, urologist, and other. For analysis, responses were grouped according to OB/GYN and non-OB/GYN.
Statistical analysis
Survey results were summarized using descriptive statistics (means for continuous variables; frequencies and weighted percentages for categorical variables). To achieve a national representation of the US female population aged 18–49 years, all data were weighted (using the random iterative method) by education, age, race, region, and household income. 22 The weighting algorithm included a propensity score to adjust for attitudinal and behavioral differences between those participants who are online and those who are not, those who join online panels and those who do not, and those who responded to the survey and those who did not. 22 To limit any extreme weighting or outliers, weight values were capped based on standard parameters according to sample size. 23
Univariate analyses were used to identify factors associated with time to diagnosis of endometriosis. T-tests and analysis of variance models were used to estimate differences between groups in continuous variables, and the Rao–Scott chi-square test was used to estimate differences in categorical variables. 24 Time from symptom onset to first consultation and time from first consultation to diagnosis were assessed independently for each variable of interest. To simplify interpretation of results and increase statistical power, several survey questions with multiple response options were grouped into dichotomous categories. To assess potential trends in diagnostic delay over time, we also performed an analysis of respondents grouped by duration of diagnosis (<5 years vs. 5–10 years). All analyses were completed using SAS 9.3 (SAS Institute, Inc., Cary, NC).
Results
Sociodemographic characteristics
A total of 59,411 women aged 18–54 years completed the screening portion of the survey (Fig. 1). Of these, 36,265 were excluded from the analysis because they were not diagnosed with or symptomatic of endometriosis or UF or did not agree to informed consent; another 17,267 met qualifying criteria, but were excluded because they entered the survey after prespecified quotas were met. Of the remaining 5879 respondents who completed the main survey, 3249 were aged 50–54 years and/or did not report a diagnosis or symptoms consistent with endometriosis; 800 reported symptoms consistent with endometriosis, but did not report being diagnosed by a physician; 812 did not have valid data for both periods of interest (time from symptom onset to first consultation and time from first consultation to diagnosis); and 380 reported being diagnosed greater than 10 years before the survey.
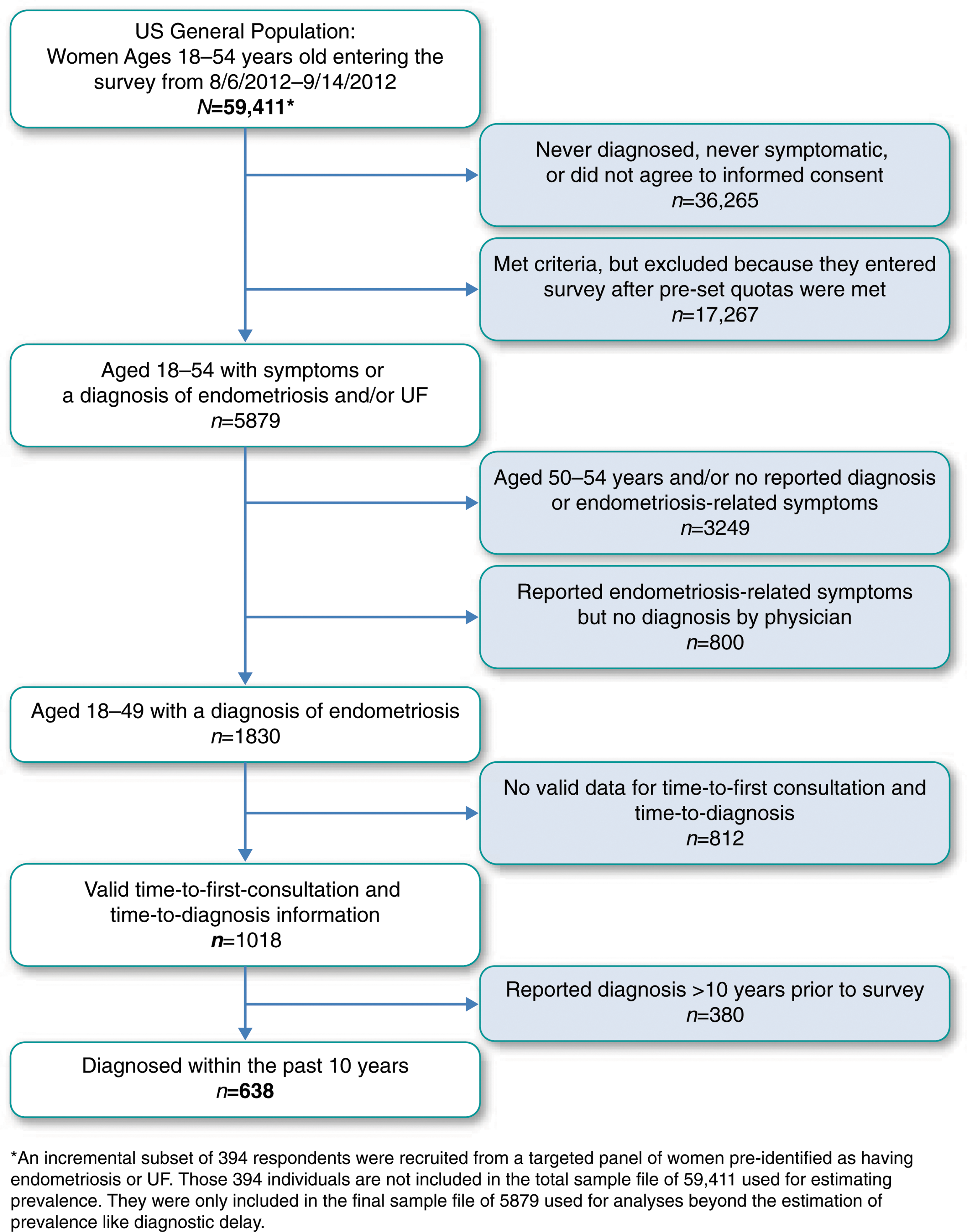
Patient Selection Flow Diagram. UF, uterine fibroids; US, United States.
Baseline sociodemographic characteristics of the final sample are shown in Table 1. Mean age was ∼32 years. Most (72%) respondents were white; 78% had a college or higher education; and 59% were privately insured. The sample captured a broad economic and geographic distribution of respondents.
Except where noted, values are reported as frequency (weighted %).
US, United States.
Symptom burden and diagnostic experience
Clinical characteristics are summarized in Table 2. Mean age at symptom onset was 23.2 years, and mean age at diagnosis was 27.5 years. The average overall delay from symptom onset to endometriosis diagnosis was ∼4.4 years; mean time from symptom onset to first consultation was ∼2.4 years, and mean time from first consultation to diagnosis was ∼2.0 years (Fig. 2). An independent assessment of overall delay from symptom onset to endometriosis diagnosis yielded similar results (mean time to diagnosis = 4.6 years).
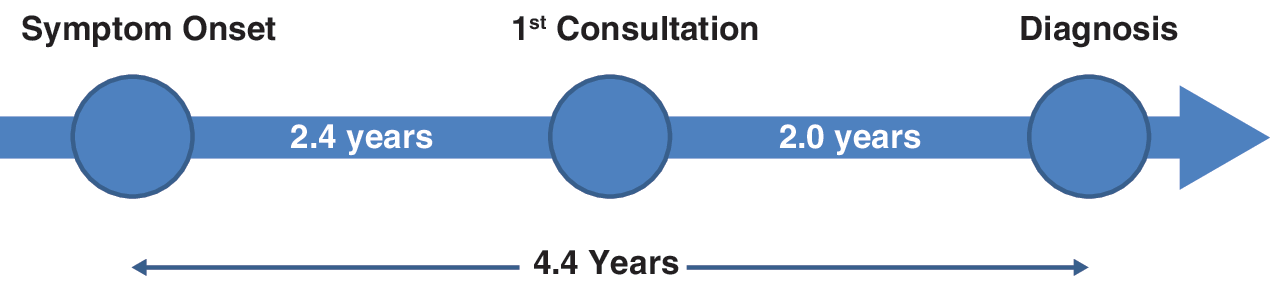
Components of diagnostic delay. Mean overall time from symptom onset to diagnosis of endometriosis, as well as patient- and physician-related components, are shown.
Values reported as frequency (weighted %) unless otherwise noted.
Primary symptoms include pelvic pain/cramping during menstrual period, pelvic pain during nonmenstrual period days, and pain during sex.
OB/GYN, obstetrician/gynecologist.
We also examined the relationship between severity of endometriosis at the time of survey administration and the time from symptom onset to first physician visit. The percentage of women with mild, moderate, and severe symptoms was 8.3%, 37.2%, and 54.5%, respectively. For women with mild, moderate, and severe symptoms, time from symptom onset to first physician visit was 1.7, 2.6, and 2.3 years, respectively; time from first physician visit to diagnosis was 1.2, 2.0, and 2.2 years, respectively; and time from symptom onset to diagnosis was 2.9, 4.6, and 4.5 years, respectively.
The most common single symptom (reported by 32% of patients) that led to a consultation was menstrual pain, whereas a majority of respondents (56%) reported seeking medical attention for at least one of three symptoms commonly considered hallmarks of endometriosis—menstrual pain, nonmenstrual pain, and pain during sex. 3,25 These three symptoms were present simultaneously only in ∼10% of respondents. Heavy menstrual periods were reported by 14% of respondents. Less commonly reported symptoms (occurring in <3% of respondents each) that led to consultation included excessive or irregular bleeding, passage of clots, pelvic pressure, and gastrointestinal problems.
Approximately 7% of respondents who were eventually diagnosed with endometriosis indicated seeking treatment for another condition or as part of routine care. Approximately 19% of respondents reported having experienced infertility; however, none indicated that infertility was the primary symptom leading to consultation. Nearly all respondents (99.7%) reported experiencing endometriosis-related symptoms before diagnosis, with the vast majority (93%) having sought medical attention for symptom relief. Symptom severity at the time of diagnosis was reported as moderate to severe by 92% of respondents; moreover, nearly 40% of respondents had an emergency department visit to seek symptom relief.
Most endometriosis diagnoses (84%) were made by OB/GYNs and 16% were made by non-OB/GYNs. Approximately 6% of respondents reported being diagnosed by primary care physicians (PCPs); smaller proportions reported diagnosis by general surgeons, infertility specialists, urologists, and others (<5% each). Diagnostic method was reported as surgical (laparoscopy, laparotomy, or other surgical procedure) in 49% of respondents and nonsurgical (all other methods) in 51%. A majority of respondents (64%) had been diagnosed with endometriosis within the past 5 years.
Factors associated with diagnostic delay
Age
Associations of sociodemographic and clinical factors with diagnostic delay are summarized in Tables 3 and 4, respectively. As shown in Table 3, younger age at symptom onset was associated with significantly longer diagnostic delay; both time from symptom onset to first consultation and time from first consultation to diagnosis were progressively greater among respondents aged >40, >30, >18, and <18 years, respectively. Time from symptom onset to first consultation was significantly shorter for all age groups compared with the <18-year age group, and time from first consultation to diagnosis was significantly shorter for the 30- to 39-year and 40- to 49-year age groups compared with the <18-year age group (p < 0.01 each comparison).
Ref., reference group for comparisons.
Ethnicity
Mean time from symptom onset to first consultation was significantly longer among white versus other (i.e., those who identified as neither white nor black) respondents (31.4 vs. 21.4 months; p = 0.0148), and mean time from first consultation to diagnosis was significantly shorter among black versus white respondents (8.7 vs. 25.7 months; p < 0.0001).Other sociodemographic characteristics (education, income, insurance status, and geographic region) generally had little relationship to the duration of diagnostic delay.
Symptom experience
As shown in Table 4, time from symptom onset to first consultation was significantly shorter among respondents who sought treatment for endometriosis-related symptoms (except pelvic pressure) compared with those who were diagnosed during routine medical care; mean time from symptom onset to consultation ranged from 14 months for respondents with constipation, bloating, or diarrhea to 28 months for respondents with pain during sex versus 61 months for those in routine care (p < 0.05 for all comparisons).
Diagnostic experience
Time from symptom onset to first consultation, but not time from first consultation to diagnosis, was significantly shorter among patients who reported having had a diagnostic procedure (e.g., ultrasound, MRI) compared with those who did not (mean 24.9 vs. 39.7 months; p = 0.0017). In contrast, no significant differences were observed for patients who reported having had a surgical procedure to seek symptom relief and those who did not. No significant associations were observed between diagnostic delay and either emergency department visits or hospitalizations related to endometriosis-related symptoms.
Time from first consultation to diagnosis of endometriosis was significantly shorter among respondents seen by an OB/GYN compared with those seen by non-OB/GYNs; mean time from consultation to diagnosis was 21.5 versus 40.3 months (p = 0.041), respectively. Those diagnosed via nonsurgical methods tended to have a shorter time to diagnosis compared with those diagnosed surgically (mean time from first consultation to diagnosis 21.1 vs. 28.1 months, respectively); however, the difference was not statistically significant. In addition, time to diagnosis of endometriosis was not significantly different among those diagnosed within 5 years of the survey versus those diagnosed from 5 to 10 years before the survey.
Discussion
Results from the current study indicate a shorter overall delay in the diagnosis of endometriosis over the past 15–20 years in the US. In the present study, the average time from symptom onset to endometriosis diagnosis among US women was 4.4 years, less than half of the 9-year estimates reported in 1998 11,12 and nearly three times shorter than the 12-year estimate reported in 1996 2 (Supplementary Table S1).
Average times from symptom onset to first physician consultation and from first consultation to diagnosis were 2.4 and 2.0 years, respectively, compared with 4.6 and 4.7 years, respectively, reported for 4334 surgically diagnosed women who participated in a 1998 survey conducted by the Endometriosis Association. 12 A shorter time to diagnosis of endometriosis, therefore, appears to be driven both by women seeking medical attention more quickly once they experience symptoms and with faster diagnosis following presentation to a physician. Together, these results suggest that public and physician awareness of endometriosis symptoms and clinical practice methods may have improved over time.
The overall time to diagnosis in the US appears similar to or slightly better than recent global estimates of ∼5–7 years 6 –10 (Supplementary Table S1). In addition, our study provides a greater level of detail in terms of symptom burden and diagnostic delay compared with these recent international studies. 6 –10 As shown in Supplementary Table S1, we compare our results with several study populations, including tertiary centers, outpatient clinics, endometriosis association members, and online market research providers. Some of these studies examine data from 10 countries and include information on diagnostic delay of endometriosis in women across different cultures and healthcare settings. 6,8
Across the studies summarized in Supplementary Table S1, reported diagnostic delays ranged from 5 to 12 years with shorter delays being reported in more recent years. Research on all of these populations needs to be performed to obtain a complete understanding of the factors contributing to diagnostic delay. To ensure that our survey sample would be representative of the national US population, we used a weighting algorithm with propensity score adjustment to control for attitudinal and behavioral differences between study participants who join online panels and those who do not to reduce selection bias.
It is important to note that whereas the majority of previous studies have been restricted to patients with surgically confirmed diagnoses, the current study included women who were diagnosed via surgical and nonsurgical methods. Nonsurgical diagnoses were slightly more common than surgical diagnoses among women in our sample, and those diagnosed via nonsurgical methods tended to have a shorter time to diagnosis.
Although current clinical practice guidelines continue to advocate laparoscopic surgery as the gold standard for diagnosis of endometriosis, these guidelines also emphasize the importance of flexibility in diagnostic and therapeutic thinking and include limited roles for advanced imaging techniques (transvaginal ultrasound and MRI) in disease assessment as well as trials of empirical treatments, such as nonsteroidal anti-inflammatory drugs, combined oral contraceptives, and (in some guidelines) gonadotropin-releasing hormone agonists, in cases of suspected, but unconfirmed, endometriosis. 5,16
Approximately three-fourths of respondents reported receiving diagnostic imaging procedures. However, time from consultation to diagnosis was not affected by the use of imaging. The basis for this result is unclear. Detailed analyses of clinical algorithms employed in endometriosis diagnosis (e.g., the potential use of empirical treatments, the timing of treatments relative to diagnostic imaging, and the identification of physicians most likely to order treatments and/or imaging) were beyond the scope of this analysis.
Overall, our results appear to be consistent with a shift in clinical practice toward the use of nonsurgical diagnostic methods, including emphasis on symptom presentation, empirical treatments, and/or use of imaging techniques for the diagnosis and management of endometriosis. This shift may be associated with greater quality of life, owing to timelier symptom relief, and with lower economic burden associated with surgery. 13
Despite the overall reduction in the time to endometriosis diagnosis, a broad range in time to diagnosis was reported among various segments of respondents. Young women, particularly those aged ≤18 years at symptom onset, experienced significantly longer time to diagnosis than older women. The greater delay was associated with longer delays both in seeking medical attention and in receiving a diagnosis following presentation. These results are consistent with a number of previous reports showing longer time to diagnosis of endometriosis among adolescents and young women compared with older women. 6,10,12 For example, the study of women who completed the 1998 Endometriosis Association survey showed that young women aged <19 years at symptom onset waited an average of three times longer than those aged >19 years to seek medical attention (mean 6 years vs. 2 years) and 2.8 times longer to receive a diagnosis following consultation (mean 5.4 years vs. 1.9 years). 12
Longer time to diagnosis in younger women is thought to be associated with poor awareness of endometriosis symptoms in young women and with failure of physicians to consider the diagnosis of endometriosis or reluctance to consider surgical intervention or empirical treatment in this group. 12 Although the trend toward more timely diagnosis among young women is encouraging, the continued gap in time to diagnosis between younger and older women supports an emphasis on targeting younger women and their physicians for increased education. 26
The burden of endometriosis-related symptoms among respondents in our sample was comparable with that observed in previous studies. For example, a study of 5540 patients with surgically diagnosed endometriosis in the UK General Practice Research Database revealed a prevalence of 25% for dysmenorrhea, 16% for pelvic pain, 9.2% for dyspareunia, and 23% for menorrhagia. 3 These frequencies are remarkably similar to the prevalence reported here for women with a combination of surgically and nonsurgically based diagnoses. The presence of endometriosis-related symptoms was strongly associated with shorter waiting time before seeking medical attention among respondents in our sample, suggesting that symptoms are a key trigger for women to seek medical attention.
A trend toward shorter time from consultation to diagnosis was noted for patients who reported seeking care for symptoms such as pelvic pain, passage of clots, and constipation/bloating/diarrhea; however, no single symptom reached statistical significance in this analysis. Clinicians take multiple factors into account when considering a diagnosis of endometriosis or other medical conditions, and further research into physician-related factors (for example, the presence of multiple symptoms) with the potential to impact the time to endometriosis diagnosis is warranted.
Time from first consultation to diagnosis was nearly two times shorter among respondents diagnosed by OB/GYNs compared with those diagnosed by other specialists. This finding suggests that OB/GYNs are likely better sensitized to the constellation of endometriosis-related symptoms compared with other specialists and indicates that non-OB/GYNs may benefit from greater awareness of endometriosis signs, symptoms, and diagnostic guidelines. It is likely that women who were diagnosed by non-OB/GYNs consulted with a greater number of physicians before receiving a diagnosis 27 ; however, this possibility was not assessed in the current study.
A considerable strength of the current study is that it included a large nationally representative sample of women who were diagnosed over a 10-year period, suggesting that results should be readily generalizable to a broader population. Our survey limited enrollment to those with a diagnosis within the past 10 years, strengthening the internal validity through control of recall bias. However, the study is also limited in several respects. First, comparison of our results with those from other studies may be affected by the fact that our survey is the first to be conducted entirely over the Internet. Although we incorporated a propensity score, which aimed at correcting for differences between participants in online surveys and the general population, into our algorithm, we cannot entirely exclude the possibility of sample bias owing to online methodology.
Second, our survey may be limited by unreliable recall among respondents who are asked to recall events from the distant past. 21 We sought to minimize recall bias by limiting our sample to respondents who received the diagnosis within the past 10 years. We also note that previous surveys incorporate a similar recall time. Data regarding diagnostic experience were entirely patient reported; additional studies that include physician input would strengthen our results. Studies replicating our findings using a larger sample of US patients with recently diagnosed endometriosis are also warranted.
Finally, in contrast with prior studies, we did not restrict our analysis to patients with surgically confirmed diagnoses. Therefore, it was not possible for us to assess the prevalence of misdiagnosis (which has been previously shown to be associated with increased diagnostic delay) among patients in our sample. Although it is possible that inclusion of respondents without surgically confirmed diagnoses would skew our results, we found that diagnostic delay was similar among both groups, suggesting that the overall estimate is robust.
Conclusion and future directions
During 2002–2012, the average delay in endometriosis diagnosis among US women in our sample was 4.4 years, reflecting a major improvement in time to diagnosis over the past 15 years. Half of all diagnoses were based on surgery and half were based on nonsurgical methods.
Predictors of shorter diagnostic delay included older age of women, presence of endometriosis-related symptoms, and OB/GYN as the specialty of the diagnosing physician and careful examination of how these predictors influence diagnosis may assist in identifying appropriate corrective action to reduce diagnostic delay. For example, further research into the relationship between reporting of symptoms and the time between consultation and diagnosis may provide insight into ways to shorten time to diagnosis. Programs educating younger women and their physicians about the complete spectrum of endometriosis-related symptoms may encourage younger women to seek medical attention earlier and result in shorter time to diagnosis.
Footnotes
Acknowledgments
Medical writing and editorial support were provided by Eric Bertelsen, PhD, and Joann Hettasch, PhD, of the Fishawack Group of Companies. Financial support for these services was provided by AbbVie. The authors would like to dedicate this article to the memory of Dr. Craig Alan Winkel, MD, MBA (1945–2016), for his significant contribution to the development of the article.
Financial Support
Financial support for this study and for medical writing and editing services was provided by AbbVie, Inc.
Role of Sponsor
AbbVie participated in developing the study design; data collection, analysis, and interpretation; writing, review, and approval of the manuscript; and the decision to submit the manuscript for publication.
Author Disclosure Statements
A.S., M.F., and M.S. are employees of AbbVie and may own stock or stock options in AbbVie. C. Winkel has served as a consultant for AbbVie and has received consulting fees for research from AbbVie.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.