
Abstract
Background:
Studies have shown conflicting information regarding the association between the age at menarche and/or menopause and cardiovascular and cerebrovascular diseases in older women. This study aimed to determine whether a longer duration of reproductive years in older women in the U.S. population was associated with a lower risk of cardiovascular and cerebrovascular diseases.
Materials and Methods:
Women ≥60 years who participated in the National Health and Nutrition Examination Survey from 2007 to 2012 were included. Subjects provided information about the age of menarche and menopause along with the presence/absence of cardiovascular and cerebrovascular diseases. Participants were categorized into either a longer reproductive duration group (>30 years) or shorter reproductive duration group (≤30 years). Subgroup analysis for each 5-year increment in the longer reproductive duration group was conducted. Relative risk (RR) regression was performed using a generalized linear model adjusting for several confounding factors.
Results:
3081 participants were included in the analysis. A longer duration of reproductive years was associated with a lower risk of cardiovascular and cerebrovascular diseases, compared with a shorter duration (RR 0.70, 95% confidence interval [CI] 0.53–0.92). This association was due to a reduction in the risk of stroke (RR 0.53, 95% CI 0.34–0.88) and angina (RR 0.57, 95% CI 0.34–0.97). A 1 year increase in the reproductive duration was associated with a 3% reduction in the risk of events (RR 0.97, 95% CI 0.95–0.99).
Conclusion:
Among women ≥60 years, a longer duration of reproductive years was associated with lower risk of cardiovascular and cerebrovascular diseases. This association was mainly due to a reduction in the risk of stroke and angina.
C
Several studies have examined the association between the age at menarche or menopause and cardiovascular and cerebrovascular diseases; however, the results are conflicting and targeted primarily a non-U.S. population. 3 –6 For example, an early age of menarche (<12 years) was shown to increase the risk of cardiovascular morbidity and mortality in several studies, 4,5 while another report demonstrated that early menarche was associated with a lower risk of ischemic stroke. 6 Moreover, few studies evaluated the actual duration of the reproductive years (i.e., the difference between the age of menopause and the age at first menarche) and its association with the risk of stroke. 5
The assessment of the actual duration of the reproductive duration and its association with cardiovascular and cerebrovascular diseases is important since this reflects a cumulative exposure to sex hormones, which would further improve our understanding about the role of reproductive factors on cardiovascular and cerebrovascular diseases. In this study, we hypothesized that the longer duration of reproductive years was associated with a lower risk of cardiovascular and cerebrovascular diseases in older women and aimed to test this hypothesis using data from the National Health and Nutrition Examination Survey (NHANES).
Materials and Methods
Study population
We utilized the NHANES data, which is a nationally representative cohort of civilian individuals across the United States. Information about the NHANES database has been described elsewhere. 7 We enrolled all women ≥60 years who participated in the NHANES interview cycles from 2007 to 2012. We required that the participant reported both ages at menarche and menopause in the reproductive history section and answered the survey questions of the medical conditions section related to cardiovascular and cerebrovascular diseases. Participants who developed a cardiovascular or cerebrovascular outcome before the menopause age were excluded from the analysis as they did not complete the exposure period, and the risk of a secondary cardiovascular event is known to be higher than the risk of a primary event.
Data collection
Participants were interviewed annually at home and examined in mobile examination centers. All procedures for data collection were approved by the National Center for Health Statistics Ethics Review Board and all participants provided written informed consent before data collection.
Definitions
The exposure variable was the duration of reproductive years; defined as the difference between the age of menopause (defined as natural “menopause” or surgical removal of the ovaries) and the age of first menarche. If the participant reported a range for menarche or menopause rather than actual numbers, the average number for the maximum and minimum numbers of this range was used. Since most studies defined early menarche <12 years and early menopause <40 years, we used a reproductive duration ≤30 years as a cutoff for the reproductive duration. 5,8 Based on the reproductive duration, the included individuals were categorized into two groups: longer reproductive duration (>30 years) and shorter reproductive duration (≤30 years). In an attempt to further refine the range of reproductive duration that was associated with lower cardiovascular and cerebrovascular outcomes, we further divided the longer reproductive duration group into subgroups with 5-year increments.
Outcomes measures
The primary outcome variable was the occurrence of any cardiovascular or cerebrovascular outcome, which was considered present if the participant answered “yes” for any of the following questions: “ever told you had angina/angina pectoris,” “ever told you had heart attack,” or “ever told you had a stroke.” The participants were also asked about the age when they developed the event. If the participant reported that she developed the event before the age of menopause, this participant was excluded from the analysis. For those participants who encountered >1 cardiovascular or cerebrovascular outcome, we considered this as only one event for the primary outcome. Secondary outcomes assessed were the risk of heart attack, stroke, and angina separately (if a participant reported >1 cardiovascular or cerebrovascular, each outcome was considered separately for the analysis of the secondary outcomes).
Statistical analysis
Means and standard deviations were calculated for continuous variables while two independent sample t-tests were used to test mean differences. For categorical variables, proportions were calculated and chi square test was used to test relationships between the exposure groups. As the outcome measured in the study was binary and prevalent, generalized linear model (GLM) was used, and relative risk (RR) regression was calculated since it was considered more conservative. 9 The following covariates were adjusted for: age, race/ethnicity, any use of hormonal replacement therapy, any use of oral contraceptive usage, parity (as a continuous variable), diabetes, hypertension, current smoking, education, low density lipoprotein levels, physical activity (measured as exercise for at least 30 minutes/day), and age of menopause. 10 –14
Multiple imputations using the discriminant function method were used to account for the arbitrary missingnesss of the data, only if <20% of the data was missing for this covariate. Low density lipoprotein level was the only variable that was not accounted for with imputations as the missing data for this variable was 68%. We further stratified the primary outcome according to the body mass index (BMI) (<25 vs. ≥25 kg/m2), and smoking status (current smokers vs. none). A secondary analysis using survey logistic using odds ratio that allows logistic modeling for complex survey designs was conducted. A third model was performed for the primary outcome for reproductive duration as a continuous variable. All statistical analyses were performed using SAS (SAS Institute, Inc., Cary, North Carolina) version 9.4.
Results
Enrolled participants
Among 30,442 individuals who participated in the survey cycles 2007–2012, 3081 women ≥60 years were included in the final analysis: 1029 in the shorter reproductive year group and 2052 in the longer reproductive duration group (Fig. 1). The mean age of the participants was 70 years. Non-Hispanic Whites comprised about 50% of the included subjects. The prevalence of some of the known risk factors for cardiovascular and cerebrovascular diseases such as diabetes, smoking, and BMI was comparable among the groups, while there was a difference in the prevalence of hypertension across the different groups. College degree or higher was more prevalent in the longer reproductive year group, while exercising >30 minutes/day was similar among the groups. The prevalence of hormone replacement therapy use was more in women with longer reproductive duration, whereas the use of oral contraceptive pills was comparable. The baseline characteristics of the study participants are shown in Table 1.
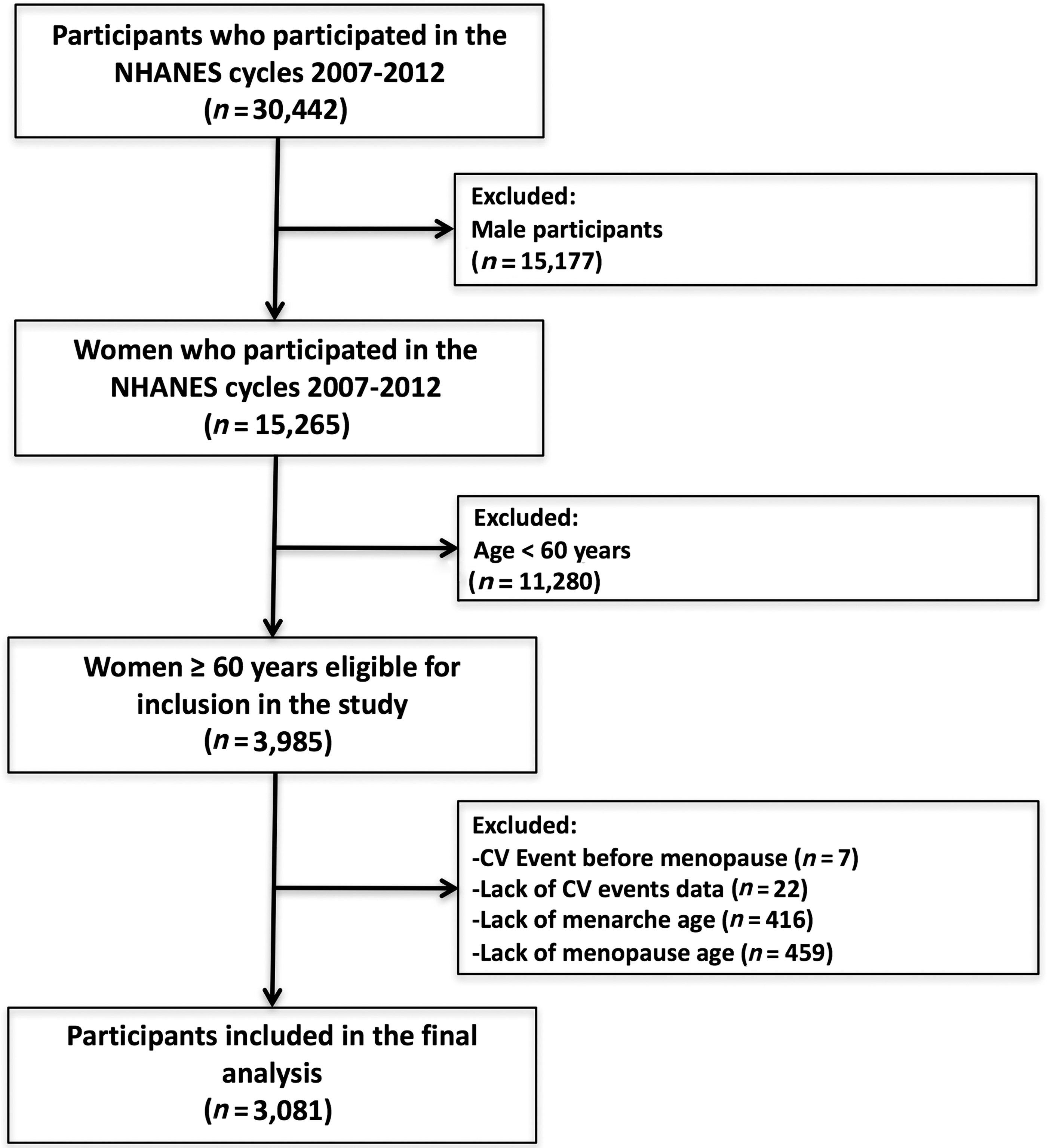
Flow diagram of study participants. CV, cardiovascular or cerebrovascular; NHANES, National Health and Nutrition Examination Survey.
Data are reported mean ± standard deviation.
BMI, body mass index; DM, diabetes mellitus; HRT, hormonal replacement therapy; HTN, hypertension; LDL, low-density lipoprotein; HDL, high-density lipoprotein.
Outcomes
Among the 3081 women included in the analysis, 177 (5.7%) developed >1 cardiovascular or cerebrovascular event. The multivariable analysis of the GLM for the adjusted analysis showed that the longer reproductive duration group had a lower risk of cardiovascular and cerebrovascular outcomes when compared with the shorter reproductive duration group (14.5% vs. 22.8%, adjusted RR 0.70, 95% confidence interval [CI] 0.53–0.92, p = 0.01) (Fig. 2). There was no evidence for effect modification based on BMI (BMI ≥25 kg/m2 [RR 0.70, 95% CI 0.51–0.97, p = 0.03], vs. BMI <25 kg/m2 [RR 0.74, 95% CI 0.48–1.14, p = 0.17], Pinteraction = 0.14), or smoking status (none-smoking [RR 0.68, 95% CI 0.51–0.91, p = 0.01], vs. current-smoking status [RR 0.78, 95% CI 0.42–1.45, p = 0.43], Pinteraction = 0.44).

Forest plot for the multivariate regression analysis for the primary outcome with the included covariates. Higher degree of education (i.e., college degree or higher) and non-Hispanic Black race were associated with a lower risk of the primary outcome, while age >70 years, diabetes, and hypertension were associated with an increased risk of the primary outcome.
Among the different variables included in the multivariable model, a higher degree of education (i.e., college degree or higher) and non-Hispanic black race were associated with a lower risk of the primary outcome, while age >70 years, diabetes, and hypertension were association with an increased risk of the primary outcome (Fig. 2).
For the primary outcome, the secondary analysis using survey logistic yielded a similar overall association. The third analysis using reproductive duration as a continuous variable demonstrated that for every year increase in the reproductive duration was associated with a 3% reduction in the risk of cardiovascular and cerebrovascular outcomes (RR 0.97, 95% CI 0.95–0.99, p = 0.01). The subgroup analysis based on the 5-year increment of the reproductive duration demonstrated that the subgroup with a reproductive duration ranging from 36 to 40 years was associated with a lower risk of cardiovascular and cerebrovascular diseases (Table 2).
The multivariate regression model was adjusted for age >70 years, race, education, age of menopause, parity, use of hormone replacement therapy, use of oral contraceptive therapy, diabetes, hypertension, LDL cholesterol, current smoking, physical activity, and cycle year.
Reported as longer reproductive duration group/shorter reproductive duration group.
The reference group was the shorter reproductive duration group.
Regarding the secondary outcomes evaluated in this analysis, the risk of stroke, and angina was lower in the longer reproductive duration group versus the shorter reproductive duration group (7.0% vs. 10.7%; adjusted RR 0.53, 95% CI 0.34–0.83, p = 0.005) (Supplementary Fig. S1; Supplementary Data are available online at
Discussion
In this observational study of 3081 women aged ≥60 years from a nationally representative cohort, we demonstrated that a longer duration of reproductive years (>30 years) was associated with a 30% reduction in the risk of any cardiovascular and cerebrovascular outcome compared with those with a shorter duration of reproductive years (≤30 years). Moreover, there was a reduction in the risk of stroke and angina individually. This association was mainly observed in the older women who had a reproductive duration ranging from 36 to 40 years. A potential explanation for the lack of benefit in the reproductive duration subgroup >40 years is the low number of participants in these subgroups (i.e., 41–45 years, and >45 years), which might have accounted for the lack of statistical significance. This is supported by the analysis with reproductive duration as a continuous variable, which suggested that every year increase in the reproductive duration was associated with a 3% reduction in the risk of cardiovascular and cerebrovascular events.
It is worth mentioning that the mean age of menarche was not statistically different in all groups, while the mean age of menopause was variable. Prior research has investigated both age at menopause and actual reproductive duration as risk factors for cardiovascular and cerebrovascular diseases, one study suggested that later menopause was associated with a lower risk of ischemic stroke, 5 and another showing that a longer reproductive duration was associated with a lower incidence of stroke in postmenopausal women in Taiwan. 6 A recent systematic review suggested that menopause age >45 years was associated with a lower risk of coronary heart disease, cardiovascular mortality, and overall mortality, 15 our findings support the importance of considering the actual duration of the reproductive duration as part of the cardiovascular and cerebrovascular risk assessment in older women.
The strength of this study lies in its large sample of participants from different survey cycles. Also, the combined outcome for all cardiovascular and cerebrovascular diseases allowed for better assessment of the relationship between reproductive history and cardiovascular and cerebrovascular diseases. The study targeted older women in the United States, a population in which the risk of cardiovascular and cerebrovascular diseases has not been well studied.
However, the study had some limitations. First, the cross-sectional and survey design of the study does not allow for causal inference. Second, the possibility of recall bias for the exposure, outcome, and some covariates represents a possible limitation since these findings were based on self-reporting with lack of validation of the documented information; however, studies have demonstrated that the recall of age of menarche and menopause are fairly accurate. 16 Third, some unmeasured cofounding factors might exist; for example, the intake of exogenous estrogen in medications and herbal remedies, which might alter the measurement of actual estrogen exposure and affect the results. Fourth, the duration of follow-up (i.e., the age at which the survey was conducted and the age of menopause) was not the same for all study groups; participants with shorter reproductive years were followed longer than those with a longer duration. This implies a possibility of risk window bias as a longer window of observation was attributed to the shorter duration group compared to longer reproductive duration groups. However, limiting the follow-up time would result in natural increase in the risk of cardiovascular and cerebrovascular outcomes in older compared to younger women, and age would be a covariate. Fifth, we could not account for time varying covariates due to the cross-sectional design of the study. Sixth, atrial fibrillation is an important risk factor for ischemic stroke and might be a confounder; however, these data are not available in the NHANES survey and so we were unable to adjust for atrial fibrillation in this study. Seventh, although we aimed to determine the association between reproductive duration and ischemic cerebrovascular and cardiovascular disease, the data regarding the etiology of stroke (ischemic vs. hemorrhagic) are unavailable in the NHANES survey. However; prior studies demonstrated that ischemic stroke represents >85% of all strokes. 1,17 Eighth, certain pregnancy complications (e.g., pre-eclampsia), and other conditions such as polycystic ovarian disease are associated with an increased risk of cardiovascular events; however, we were unable to account for these variables in the multivariable model since these data are lacking in NHANES. Ninth, we could not comment on the effect of surgical menopause (i.e., surgical oophorectomy) on the risk of cardiovascular and cerebrovascular diseases in our analysis as this information was remarkably missing in the NHANES database. However, prior studies had suggested that surgical menopause is an independent risk factor of cardiovascular events. 18 Finally, we used the reproductive duration as the surrogate for the period of estrogen exposure; however, estrogen levels are usually not similar during this whole period, since the levels usually are lower at both ends of the reproductive duration.
The results from the present study support the hypothesis that endogenous estrogen is cardioprotective. These findings can be used to further characterize the risk factors of cardiovascular and cerebrovascular diseases in women along with incorporating reproductive history into a predictive risk model that could be used in clinical practice as suggested by the AHA. 2 Our results support the recommendation to include the reproductive history for risk estimation in postmenopausal women to optimize preventive measures against cardiovascular and cerebrovascular disease. Future studies with larger sample sizes in a prospective design are needed to overcome the stated limitations and to determine the association on a larger scale.
Conclusions
Longer duration of reproductive years was associated with lower risk of cardiovascular and cerebrovascular diseases in women aged 60 years and older from a survey that enrolled a large sample size of the U.S. population. This association was mainly due to a reduction in the risk of stroke and angina.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.