
Abstract
Background:
There is evidence showing that marital status (MS) and marital disruption (i.e., separation, divorce, and being widowed) are associated with poor physical health outcomes, including for all-cause mortality. We checked for the available evidence on the association between MS and cardiovascular (CV) diseases, outcomes, and CV risk factors.
Methods:
A search across the PubMed database of all articles, including the term “marital status” in their title, was performed. All articles were then manually checked for the presence of the following terms or topic: CV diseases, acute myocardial infarction, acute coronary syndrome, coronary artery disease, cardiac arrest, heart failure, heart diseases, and CV mortality. Moreover, other search terms were: CV risk factors, hypertension, cholesterol, obesity, smoking, alcohol, fitness and/or physical activity, and health. Systematic reviews, meta-analyses, controlled trials, cohort studies, and case–control studies were potentially considered pertinent for inclusion. Case reports, comments, discussion letters, abstracts of scientific conferences, articles in other than English language, and conference abstracts or proceedings were excluded.
Results:
In total, 817 references containing the title words “marital status” were found. After elimination of articles dealing with other topics, 70 records were considered pertinent. Twenty-two were eliminated for several reasons, such as old articles, no abstract, full text unavailable, other than English language, comments, and letters. Out of the remaining 48 articles, 13 were suitable for the discussion, and 35 (accounting for 1,245,967 subjects) were included in this study.
Conclusions:
Most studies showed better outcomes for married persons, and men who were single generally had the poorest results. Moreover, being married was associated with lower risk factors and better health status, even in the presence of many confounding effects.
Introduction
P
Support was obtained from a comprehensive review and meta-analysis of 53 studies, including more than 250,000 subjects. 3 The overall relative risk (RR) for married versus nonmarried individuals (including widowed, divorced/separated, and never married) was 0.88, independent of gender and geographical area. In particular, compared with married individuals, the widowed, divorced/separated, and never married persons had increased RRs of death (1.11, 1.16, and 1.11, respectively). 3
The aim of the present study was to evaluate the available evidence in the literature on the association between MS and either cardiovascular (CV) diseases or CV risk factors.
Methods
The first step consisted in a search across the PubMed database of all articles, including the term “marital status” in their title. All articles were then manually checked for the presence of the following terms or topic: CV diseases, acute myocardial infarction (AMI), acute coronary syndrome (ACS), coronary artery disease (CAD), cardiac arrest, heart failure, heart diseases, and CV mortality. Moreover, other search terms were: CV risk factors, hypertension, cholesterol, obesity, smoking, alcohol, fitness and/or physical activity, and health. Systematic reviews, meta-analyses, controlled trials, cohort studies, and case–control studies were potentially considered pertinent for inclusion. Case reports, comments, discussion letters, abstracts of scientific conferences, articles in other than English language, and conference abstracts or proceedings were excluded.
We decided to include all the eligible studies, independent of their sample size, since even studies with smaller samples but dealing with very particular diseases, such as heart transplantation, may provide interesting information. For simplicity, we decided to roughly split all these studies into two main general topics: (i) CV diseases and (ii) CV risk factors.
Results
In total, 817 references containing the title words “marital status” were found. Figure 1 shows the flowchart of the strategy of choice. After elimination of articles dealing with other topics, 70 records were considered pertinent. Twenty-two were eliminated for several reasons, such as old articles, no abstract, full text unavailable, other than English language, comments, and letters. Out of the remaining 48 articles, 13 were suitable for the discussion, and 35 (accounting for 1,245,967 subjects) were included in this study.
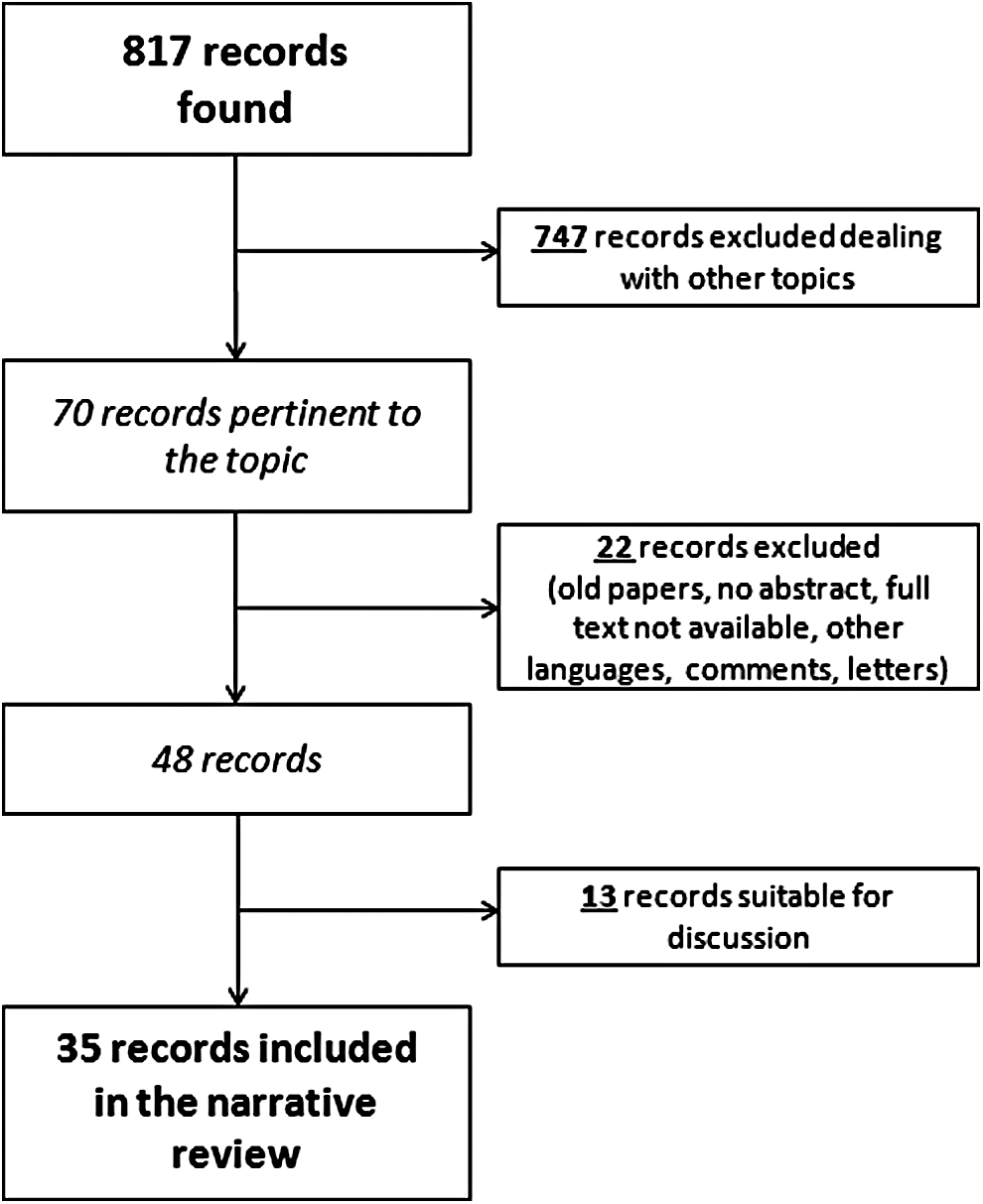
Flowchart of searching procedure.
Table 1 summarizes reports from studies dealing with CV diseases. In total, 23 studies were included (9 from the United States, 3 from United Kingdom, 2 each from Greece and Japan, and 1 each from China, Germany, Middle East, Netherlands, Spain, Sweden, and United Kingdom), accounting for 923,722 subjects in total. The lowest number of cases per study was 136 and highest 734,626. As for main topic, 19 dealt with mortality and/or survival, for example, CV diseases, myocardial infarction and coronary ischemic disease, heart failure, and heart transplantation, two dealt with risk and occurrence, that is, cardiac arrest and myocardial infarction, and two dealt with outcome, that is, percutaneous coronary intervention (PCI) and heart failure.
↑, increased; ↓, decreased.
ACS, acute coronary syndrome; AMI, acute myocardial infarction; CA, cardiac arrest; CAD, coronary artery disease; CE, coronary event; CVD, cardiovascular disease; DC, dilated cardiomyopathy; HF, heart failure; HR, hazard ratio; HT, heart transplantation; IH, inhospital; M, men; IHD, ischemic heart disease; MACE, major adverse cardiac event; MS, marital status; PCI, percutaneous coronary intervention; RR, relative risk; W, women.
Table 2 summarizes reports from studies dealing with CV risk factors. In total, 12 studies were included (4 from the United States, 2 each from Korea and Sweden, and 1 each from Finland, Greece, Hong Kong, and Japan), accounting for 322,245 subjects in total. The lowest number of cases per study was 325 and highest 127,545. As for the main topic, 7 dealt with risk factors, for example, smoking, obesity, hypertension, 1 with dietary habits, 2 with fitness and physical activity, and 2 with health and health behavior.
BMI, body mass index; BP, blood pressure; HR, hazard ratio; M, men; MS, marital status; OR, odds ratio; RR, relative risk; W, women.
In total, 20 out 35 studies provided separate analysis for subgroups by sex (57%), with similar distribution both for CV diseases (13/23, 57%) and CV risk factors (7/12, 58%).
Brief summary remarks of the results
CV diseases
Mortality and/or survival (CV diseases, in general; AMI, ACS, and CAD): married subjects generally had lower mortality rates compared with other conditions. Studies with separate analysis by gender did not report significant differences.
Dilated cardiomyopathy, heart failure, and heart transplantation: the few, small-sized available studies showed that married subjects had longer survival.
Risk and outcome: according to the limited number of studies, being married was associated with a lower risk of cardiac arrest and with a better outcome of PCI.
CV risk factors
Being married was associated with lower risk factors (contrasting results only for obesity) and a better health status. However, many confounding effects of the different studies, for example, sample size, ethnicity, and cultural habits, including diet and smoking, may significantly influence the final results especially in consideration of possible implications by gender.
Discussion
At least to the best of our knowledge, this is the first study systematically collecting all the available evidence on the impact of MS on CV diseases and CV risk factors, confirming the important role of MS. The amount of data deserves a brief detailed report of results.
CV diseases
Mortality and/or survival
CV diseases (in general)
Mendes de Leon et al. screened middle-aged men in Holland and found that nonmarried, never married, and widowed had higher risk for coronary mortality (RR 2.2, 2.9, and 2.9, respectively) than married subjects. 4 Ebrahim et al. investigated the effect of MS on mortality among ≥7,000 middle-aged British men. Single (never married) men had a higher risk of CV disease (CVD) mortality (RR = 1.5), but divorced/separated men had not. Moreover, men who divorced during the follow-up period were at increased risk of CVD mortality (RR = 1.9), whereas those who became widowed were not. 5 In a large Japanese study on ≥94,000 patients, never married W showed a smaller but significant increased risk of mortality for all causes.
As for risk of mortality for CVD, never married men compared with married men showed an increased risk of mortality from CVD. Divorced and widowed women showed moderately increased risks of mortality from CVD, compared with married women. 6 In a Scottish study, the risk of CV mortality was greatest in single never married men and separated/divorced women compared with those that were married in gender stratified models. 7 In particular, behavioral factors had a particular relevance for the relationship between being separated/divorced and CV mortality in both men and women. 7
Even in particular subgroups of patients, such as those in hemodialysis, patients who were single and those who were divorced/widowed patients had higher risk than married patients for mortality from CVD. 8 In a US study on 10-year coronary heart disease incidence and mortality, even after adjusting for classical risk factors, married men were almost half as likely to die during follow-up compared with the unmarried. 9
AMI, ACS, and CAD
Acute myocardial infarction
A study conducted in the United States, in the early ‘80 s, reported an adjusted inhospital case fatality rate for AMI of 19.7% and 26.7%, respectively, for married and unmarried males. 10 Similar findings were confirmed also for married and unmarried females (23.3% and 37.4%, respectively). A 10-year follow-up of subjects discharged alive also confirmed a better survival rate for married compared with unmarried males and females. 10 More recently, in a Spanish study the condition of widow, compared with married, was independently associated with higher all-cause death (HR = 1.29) in contrast to single (HR = 1.04) and divorced (HR = 0.84), and gender did not show interaction with MS. 11 In Germany, overall MS showed an insignificant protective HR of 0.76. However, stratified analyses revealed strong protective effects only among men and women aged <60 years and diagnosed with hyperlipidemia. Interestingly, the same protective effect (HR = 0.52) was confirmed also for subjects with cohabitation status. 12
Acute coronary syndrome
In a national cohort study in the United Kingdom, Cox analysis comparison of MS and mortality showed lower mortality rates for married (OR = 0.863), widowed (OR = 0.959), and unmarried (OR = 0.973) compared with single patients. 13 Moreover, divorced patients had significantly ↑ mortality rate compared to single patients (OR = 1.068). 13 Two Greek studies focused on ACS, with very similar results. Panagiotakos et al. found that never married patients had 2.8 times and 2.7 times higher risk of dying during hospitalization and during the first 30 days following hospitalization, respectively, compared with married patients. 14 Notara et al. reported that married patients had approximately 1/3 lower risk of ACS mortality compared with single, widowed, or divorced patients. 15
Results from a large study conducted in Middle East countries found that MS was an independent predictor for inhospital mortality and, in particular, widowed MS was associated with worse CV risk profile and both inhospital and 1-year outcome. 16 Also in Sweden, unmarried status in men, but not in women, was significantly associated with increased risk of suffering a coronary event (HR 1.10, 1.42, and 1.77 for never married, divorced, and widowed, respectively). Moreover, unmarried status was also related with an increased case fatality rate (1st day) in both men and women (M: OR = 2.14, 1.91, 1,49; W: 2.32, 1.87, 1.87, for never married, divorced, and widowed, respectively). 17 In a large study in the United Kingdom on ≥700,000 women, those who were married or living with a partner had a similar risk of a first ischemic heart disease event as women who were not (RR = 0.99), but a significantly lower risk of mortality (RR = 0.72). 18
Dilated cardiomyopathy, heart failure, and heart transplantation
In patients with idiopathic dilated cardiomyopathy, the cumulative survival at 12 and 24 months was, respectively, 54.6% and 48.5% in widowed patients, 75.8% and 59.0% among single patients, and 80.0% and 71.2% among married patients. MS was a statistically significant independent predictor of survival, with single patients having a poorer survival than those who were married (RR = 2.5). 19 As for heart failure (HF), married patients experienced longer event-free survival than unmarried ones. 20,21
However, when medication adherence entered in the model, MS was not a significant predictor of event-free survival, demonstrating a strong mediation effect on the relationship of MS to survival. 21 Once again, also in subjects with heart transplantation, it was reported a significantly improved 1-year and 5-year survival (p < 0.05 and 0.02, respectively) for married patients compared with unmarried patients. 22
Risk and outcome
Results from a cohort of ≥2,000 subjects with out-of-hospital cardiac arrest showed that cases were more likely to be unmarried than the controls (30.2% vs. 21.0%), defined as being separated or divorced, single or widowed. Unmarried participants had a higher risk of sudden cardiac arrest (OR = 1.53). 23 As for clinical outcome of patients survived to an inhospital cardiac arrest, females, especially those without a living spouse, had worse neurological outcomes than males. 24
A Chinese study showed that also after adjustment for age, sex, body mass index (BMI), psychosocial factors, lifestyle, and other risk factors, the OR for AMI associated with being single was 1.51 overall (1.19 in men and 2.00 in women, respectively). 25 MS has been found to impact also on outcome of PCI, both urgent and elective. Compared with unmarried, married patients exhibited a lower prevalence of hypertension, diabetes, and smoking and a higher prevalence of hypercholesterolemia and family history of CAD. Married patients, compared with unmarried, had significantly reduced early and late major adverse cardiac event rates up to 1 year (13.3% vs. 8.2%, p > 0.01). In multivariate analysis, MS was independently associated with improved outcome (HR = 0.7). 26 As for HF, the results from a small US study found that MS was not a significant variable for inhospital death (HR = 0.71) or for time to readmission for HF (1.16). 27
CV risk factors
Smoking
In large Korean population, smoking rates were higher for unmarried subjects compared with their married ones. The gap in smoking rates between unmarried and married women was much greater than between unmarried and married men. 28 The results showed that MS had a stronger protective influence on smoking in women than men, contrary to the gender pattern previously reported in western countries. The authors hypothesized that these findings could be explained by cultural tradition discouraging married women from smoking, but liberating divorced women. 28 In Sweden, never married and divorced subjects showed a significantly higher prevalence of daily smoking than married/cohabitating respondents 29 and, in Finland, living without a spouse was associated with daily smoking and higher nicotine dependence. 30
Obesity
In a sample of workers in Sweden, obesity was associated with an increased incidence of coronary events and deaths in all diverse occupational groups. However, being single significantly increased the CV risk associated with obesity. The multivariate adjusted RR of coronary events and deaths was, respectively, 1.91 and 2.54 (manual workers) and 4.79 and 3.80 (self-employed workers) compared with those who were cohabitants. 31 In contrast, in Greece, a higher risk of obesity was found in married men (OR = 2.28) and women (OR = 2.31) than in unmarried subjects. 32
Hypertension
A different blood pressure (BP) pattern has also been related to MS. Married subjects showed greater odds of dipping (OR = 2.26) compared with unmarried ones. Moreover, married subjects had a lower nighttime systolic BP (−2.4 mmHg), more pronounced in men than in women (−3.1 mmHg and 1.7 mmHg, respectively). 33 Moreover, single/divorced subjects had greater odds of being unaware and uncontrolled BP levels than married subjects. 34
Miscellanea
A Japanese study compared lifestyle and risk factors between men who were married and those who had never married. 35 Never married men were more likely to skip breakfast, had higher smoking rates, average values of diastolic BP, serum total cholesterol, and fasting plasma glucose. The proportion of participants with three or more risk factors, that is, smoking, hypertension, hypercholesterolemia, and hyperglycemia, was higher in the never married as well. 35
Dietary habits
In a study performed in Hong Kong, single women had lower consumption of vegetables and fish compared with married women. Single men had a better CV risk factor profile, including diastolic BP, triglycerides, and cholesterol/high-density lipoprotein ratio, and lower BMI. 36
Physical activity and fitness
MS represents important determinant for physical activity participation among older adults. Compared with single counterparts, married men reported higher median levels of exercise participation and married women reported higher levels of total activity. 37 In a sample of >8,000 US subjects, the transitions to being married (from single to married or from divorced to remarried) were associated with a modest reduction, while divorce was associated with a modest increase in fitness levels in men. 38
Health behavior
The results of a study on >120,000 US subjects showed that, regardless of any population subgroup or health indicator, married adults were generally found to be healthier than adults in other MS categories. MS differences in health were found in each of the three age groups studied (18–44, 45–64, and 65 years and over), but were most striking among adults aged 18–44 years. 39 The one negative health indicator for which married adults had a higher prevalence was overweight or obesity. Married adults, particularly men, had high rates of overweight or obesity relative to adults in other MS groups across most population subgroups studied. Never married adults were among the least likely to be overweight or obese. 40 In a Korean population of middle-aged adults, the association between MS and health behaviors differed by sex, and it was observed that subjects living with partners were more likely to have healthier behavior than living without a partner. In particular, men living without a partner had lower odds of undergoing health screening and having regular breakfast, whereas women living without a partner had higher risk of smoking and alcohol consumption. 40
The possible relationship between MS and mortality from various causes has been the object of many studies. In a large US series of >280,000 subjects, as for the group of people aged 45–64 years, nonmarried subjects showed a statistically significant higher risk of mortality for various causes compared with married counterparts. 41 Younger age groups showed higher RR than older age groups, and the higher risk in nonmarried was comparable for both females and males. 41 In a cohort of British women, being single was significantly associated with higher all-cause mortality (HR = 1.45), whereas being divorced or widowed showed no excess mortality risk. 42 More recently, also in a Chinese population (approximately 50,000 subjects), unmarried and widowed women had an increased all-cause mortality risk (+11% and +10%, respectively), but never married women showed the greatest excess (+46%).
As for mortality for CV disease, divorce and not being married were associated with elevated risk (+47% and +65%, respectively) in men. 43 Other European studies confirmed these findings as well. In a wide population study in Norway (>800,000 subjects), divorced, never married, and widowed subjects (with respective decreasing odds) had significantly higher mortality for most causes of death compared with married ones. Among the nonmarried subjects, the excess mortality among the nonmarried was higher for men than for women. 44 A study conducted in Switzerland, on nearly 2.5 million subjects, aimed to estimate all-cause mortality hazard ratio (HR) for living arrangements and MS. 47 After stratification by living arrangement, mortality risks were highest for 45–64-year-old divorced and single (HR 1.72 and 1.67, respectively) men who lived alone. In women of the same group by age, the highest risk was present in single and in those living with a partner (HR 1.70 for both). 45
Eating habits may represent a critical factor to health, and MS may have an influence. In their study on 1,514 men and 1,528 women in Greece, classified as never married, married, divorced, and widowed, Yannakoulia et al. found different dietary patterns in different subgroups, associated with BMI and total serum cholesterol. 46 In particular, never married participants showed a preferred consumption of potatoes and red meat, married participants of nuts, legumes, and fish, divorced participants of fruits, cereals, and soft drinks, whereas widowed participants preferred dairy, vegetables, sweets, and poultry. 46 Differences by gender may also exist in eating habits. The results from an important longitudinal study on middle-aged and older adults in United Kingdom showed that unhealthy changes to diet, evaluated with the four indicators of healthy eating, for example, fruit quantity and variety and vegetable quantity and variety, that accompanied divorce, separation, and becoming widowed were more common among men than women. 47
The prevalence, severity, associations, and response to treatment of several emerging CV risk factors, such as inflammatory markers, may also differ between men and women, 48 and inflammatory markers can be considered as a predictor of CV risk in women, 49 but it is not established whether MS may have some effect. A previous Swedish study was conducted on more than 6,000 apparently healthy men, measured for a series of five inflammation-sensitive proteins (fibrinogen, ceruloplasmin, haptoglobin, alpha1-antitrypsin, and orosomucoid) and followed-up over 18 years. 50 All these proteins had higher concentrations in divorced men, and also after adjustment for traditional CV risk factors, divorced men showed a higher incidence of coronary events. 50 Very recently, a study conducted in Singapore evaluated the prospective influence of MS and, among other variables, C-reactive protein (CRP) on the mortality of a cohort of 220 patients with chronic HF. 51 After adjustments for New York Heart Association (NYHA) class, age, and gender, being unmarried and higher CRP predicted mortality (OR = 2.80 and OR = 1.92, respectively). In the combined multivariate model, MS (OR = 2.20), CRP (OR = 1.91), and NYHA class (OR = 2.41) independently predicted mortality. 51 Interestingly, men remaining married in late adulthood exhibited higher protection against elevated levels of CRP. 52
Mood may contribute to poor metabolic control. It has been recently reported that women, who had higher prevalence of depression than men, showed also significant associations with metabolic risk factors, for example, high fasting blood glucose and high glycohemoglobin. 53 Alcohol consumption and MS deserve some considerations apart. Previous evidence is available showing that MS and marital disruption, that is, marital separation, divorce, are associated with a wide range of poor mental and physical health outcomes, including increased risk for all-cause mortality.
Marital disruption and alcohol consumption are tightly connected. On one hand, living alone is associated with an increased risk of alcohol-related mortality, irrespective of gender socioeconomic status or the specific cause of death. 54 On the other, the level of alcohol use is an important predictor of marital dissolution. In fact, heavy drinking among men and women increased the risk of future marital dissolution (HR = 1.39 and 1.41, respectively). The HR for divorce was 1.51 when only the husband was a heavy drinker, while it was 3.07 when only the wife was a heavy drinker. 55
Conclusions
The present study, collecting the available evidence, seems to confirm the importance of MS also for CV diseases and CV risk factors. Most studies showed better outcomes for married persons, and men who were single generally had the poorest results. It is possible that persons who are married may have lower mortality because of protective effects of marriage or even selection of healthy individuals into marriage. It is likely that people who have a spouse may exhibit higher compliance with medical controls, medications, and screening programs. For example, a study conducted in the Unites States on 36,594 adults showed that being unmarried was associated with lower odds of cholesterol screening for both genders. In particular, the widowed status was associated with the lowest likelihood of screening, with quite similar odds for men (OR = 0.56) and women (OR = 0.53). 56 Again, the attendance at outpatients cardiac rehabilitation programs was significantly higher for married/partnered subjects (OR = 1.72). 57 MS could be associated also with biological, behavioral, and also psychological factors.
Many factors could be related, in general, to being married versus loneliness: healthier meals, better sleep, less stress, financial benefits, and better mood. The single individuals who never married deserve further studies on their right as they are a self-selected group likely with their own special needs. Again, single by their choice or persons who did not find a partner to live with are the same thing? Moreover, we do not have information enough on whether the apparently protective effects of marriage are extended also in the case of same-sex spouses or partners in civil union. The recent authorization of these practices should allow more information also in these cases.
Much work is still to be done to understand the real, probably multifactorial, reasons of the connections before marriage on health and to provide convincing evidence of direct cause–effect relationships. And the topic of quality of marriage opens up another series of questions. 58 At present, we do not have enough to draw definite conclusions about recommending specific policies or program interventions. However, further studies are not only needed but also strongly suggested and even encouraged.
Footnotes
Acknowledgment
Supported, in part, by an institutional research grant “Fondo Ateneo Ricerca–FAR,” University of Ferrara, Italy.
Author Disclosure Statement
No competing financial interests exist, and there are no potential conflicts of interest by sponsoring agents, products, technology, or methodologies used in this report submitted for publication by any of the authors.