
Abstract
Background:
Untreated and subclinical hypothyroidism (SCH) has been associated with adverse pregnancy complications such as increased risk of miscarriage, hypertension, preeclampsia, and preterm delivery. However, in Sweden, screening for thyroid dysfunction during pregnancy is only recommended for women with a high risk of thyroid disease. Therefore, the aim of this study was to determine the incidence of clinical and SCH in women in the first trimester of pregnancy.
Materials and Methods:
In this prospective study, 1298 pregnant women were divided into three groups: one unselected general screening group (n = 611), one low-risk group comprising women without risk factors for thyroid disorder (n = 511), and one high-risk group comprising women with an inheritance or suspicion of thyroid disease or undergoing treatment for thyroid disease (n = 88). Serum was obtained up to gestational week 13, and thyrotropin (TSH) was analyzed.
Results:
The incidences of thyroid dysfunction in the three screening groups were 9.8% in the general screening group, 9.6% in the low-risk group, and 10.2%, p = 0.948, in the high-risk group. In the women with known hypothyroidism on levothyroxine treatment, 50.6% had serum TSH levels above 2.0 mIU/L.
Conclusions:
High-risk screening is not useful in predicting which women are at risk of thyroid disease in early pregnancy since ∼10% of women with SCH or hypothyroidism could not be diagnosed in this way.
Introduction
T
SCH has been associated with infertility and recurrent miscarriage. 6 Overt hypothyroidism and SCH have been associated with adverse pregnancy outcomes such as hypertension, preeclampsia, preterm delivery, low birth weight, intrauterine growth retardation, and neurological disorders in offspring. 7 –9
The reference value of TSH is lower in pregnant than in nonpregnant women due to the thyrotrophic effect of human chorionic gonadotropin, and it changes throughout pregnancy.
10
The current guidelines consider a serum TSH level above 2.5 mIU/L as the upper reference limit during the first trimester and a TSH 3.0 mIU/L as the upper limit during the second and third trimesters of pregnancy.
11
–13
However, the American Thyroid Association guidelines have recently been changed to 4.0 mIU/L (
Since the normal range of TSH varies according to geographic region and ethnic background, the incidence of clinical and SCH varies among studies, and the number of patients with undiscovered overt hypothyroidism/SCH remains unknown. 14 Data on the incidence of overt hypothyroidism/SCH in Swedish pregnant women are scarce; one retrospective study suggests that targeted screening for thyroid disease is unsatisfactory. 15 Therefore, the aim of the present study was to prospectively estimate the incidence of overt hypothyroidism/SCH during the first trimester of pregnancy.
Materials and Methods
Study population
The Regional Ethical Review Board in Stockholm approved the study (2009/2:6) and all participants gave informed oral and written consent before participation.
There were 1311 pregnant women with gestational ages up to 12 weeks and 6 days who were eligible for the study after seven women declined being included in the study. Women with diabetes, severe cardiovascular diseases, or systemic lupus erythematosus do not attend antenatal care units, as they attend special care units for women with high-risk pregnancies, and were therefore not included in the study. Of the remaining women, seven refused to participate and six were excluded due to loss of sample; thereby, 1298 pregnant women were included in the study. The included women were divided into three groups depending on which antenatal care unit they attended: one general screening group, one low-risk group, and one high-risk group. All women attending the two antenatal care units during the selected time period were included in the study.
The antenatal care unit north of Stockholm was in a high-income area while the unit south of Stockholm included all socioeconomic areas, both in a city and more rural parts of southern Stockholm.
General screening group
Six hundred ninety-nine unselected pregnant women from an antenatal care unit south of Stockholm were screened for serum TSH from 2009 to 2011. Women with known overt hypothyroidism/SCH and treated with LT4 (n = 48) were excluded and analyzed separately. Thus, 651 women were included in this group.
Low-risk and high-risk screening groups
Five hundred ninety-nine selected pregnant women from the northeast area of Stockholm were screened for TSH from 2009 to 2010. The selection procedure involved targeted screening for risk of thyroid dysfunction, and the women were thereafter divided into one high-risk group and one low-risk group.
The high-risk group (n = 88) included women with risk factors for thyroid dysfunction based on family history of thyroid dysfunction or previous treatment with LT4, propylthiouracil, methimazole, radioiodine, previous surgery, or goitre and women with clinical suspicion of thyroid disease, according to local guidelines in Stockholm. Twenty-nine hypothyroid women on LT4 treatment were excluded and analyzed separately. Thus, the high-risk group included 59 women. Five hundred eleven women without known risk factors, as mentioned above, were included in the low-risk group.
Serum collection and TSH analyses
Maternal serum samples were obtained at women's first visit to the antenatal care units (5–12 weeks of gestation). All blood samples were obtained before noon and were allowed to clot at room temperature for at least 30 minutes before centrifugation at 3300 rpm for 10 minutes. The samples were sent to the laboratory of clinical chemistry at Karolinska University Hospital, Solna (northeast of Stockholm), or to Karolinska University Hospital, Huddinge (south of Stockholm) and were kept at 4°C until assayed on the same or the following day. TSH was analyzed at Karolinska University Hospital, Solna, by DxI Access HYPERsensitive TSH-assay (Beckman Coulter AB, a chemiluminescent immunoenzymatic one-step sandwich assay) with an intra/interassay variation of 3.12% and 3.86%, respectively. At the Karolinska University Hospital, Huddinge, TSH was analyzed by immunoassay (Modular E 170; Roche) with an intra/interassay variation of 2.7% and 3.2%, respectively.
Reference value and treatment
The reference value of TSH was <2.0 mIU/L during early pregnancy, in accordance with the local guidelines at the time. All women with TSH ≥2.0 mIU/L (n = 81, 13.5%) at the antenatal units northeast of Stockholm were treated with LT4. TSH, fT4, and thyroid peroxidase antibodies (TPO-Ab) levels were checked 4–6 weeks after the start of treatment, with dose adjustment if necessary.
Statistics
Descriptive statistical data were compared using independent t-test, one-way analysis of variance (for continuous data), or chi-square test (for categorical data). Comparisons of the two TSH levels in the three groups were performed using chi-square test. All statistical differences with p values ≤0.05 were considered statistically significant. Statistical analyses were performed using SPSS Predictive Analytics Software PASW Statistics version 21.0 (SPSS, Inc., Chicago, Illinois).
Results
Subject's clinical characteristics
Women in the general screening group were significantly younger, with a mean age of 31 (16–50) years versus 32 (17–49) years in the low-risk group and 34 (22–44) years in the high-risk group (p < 0.001 for both). The women in the low-risk group were significantly younger than those in the high-risk group (p = 0.046). The number of smokers was higher in the general group compared with the low-risk group, p = 0.006.
Screening
There were no significant differences between the incidences of newly diagnosed cases with SCH, regardless if the TSH limit was set to 2.0 or 2.5 mIU/L (Table 1). In the low-risk group, two women had TSH levels >10 mIU/L and one woman had hyperthyroidism. In the general screening group, two women had TSH levels >10 mIU/L (Fig. 1). TPO-Ab was not measured, and hence not included.
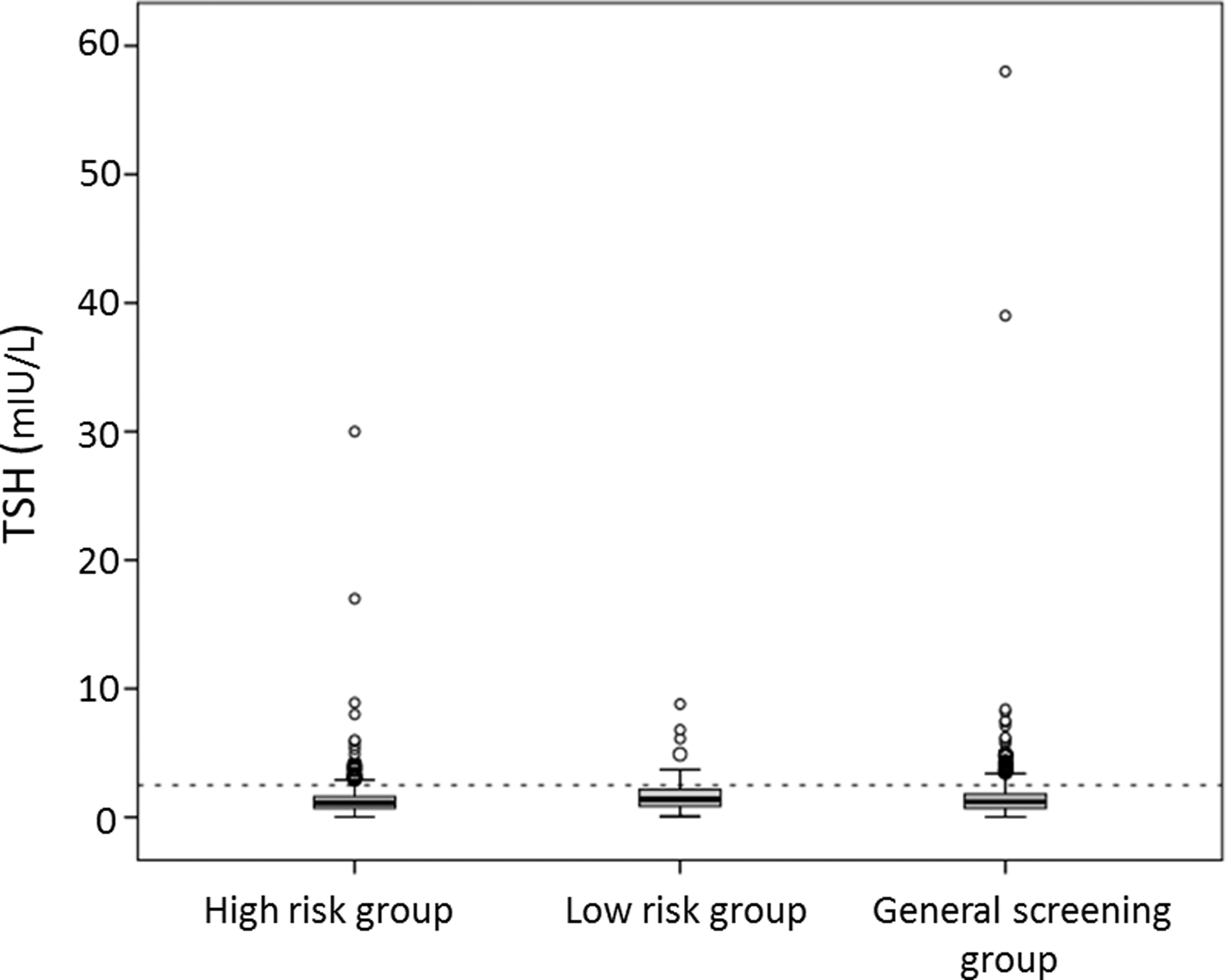
This figure shows the incidence of SCH and hypothyroidism in all study groups. The dotted line is placed at 2.5 mIU/L. There was no significant difference between the groups, p = 0.948. Statistical evaluation was performed by chi-square test. SCH, subclinical hypothyroidism.
Women with previously known hypothyroidism were not included in these groups. Data are presented as n (%), and statistical evaluation was determined using chi-square test.
TSH, thyrotropin.
Women with high TSH levels
Women with known hypothyroidism on LT4 treatment (n = 77) showed TSH levels ≥2.0 mIU/L (range 2.0–8.8) in 50.6% of cases.
Women with diagnosed SCH/hypothyroidism during the time of the study (n = 81, 13.5%) were treated with LT4 followed up with repeated serum TSH analysis during pregnancy. The incidence of pregnancy and delivery outcomes in this group did not differ from the general population.
Discussion
In the present study, the incidence of pregnant women with SCH was evaluated and found to be almost the same among the three study groups: ∼10% in women with risk factors for hypothyroidism as well as in women without these risk factors. Therefore, targeted thyroid screening cannot be used to identify women at risk of overt hypothyroidism/SCH.
It is well known that overt hypothyroidism/SCH is related to an increased risk of pregnancy complications, 7 –9 and there are also studies suggesting that there might be a risk of decreased intelligence and motor scores also in the offspring, 9,16,17 which makes it important to identify women with overt hypothyroidism/SCH. 18 However, our study shows that by applying the current guidelines as many as 10% of affected pregnant women will remain undiagnosed. In Reid et al.'s recent Cochrane review of different screening methods in early pregnancy, it was shown that, based on existing evidence, universal screening for thyroid dysfunction in pregnancy increases the number of women diagnosed and subsequently treated for hypothyroidism, but there is no clear evidence of how treatment negatively or positively affects maternal and infant outcomes. 19
To our knowledge, there are only two studies on the incidence of SCH in pregnant women in Nordic countries: one retrospective study from Sweden and one from Finland. In the retrospective cohort study conducted in the Uppsala community in Sweden, Granfors et al. showed a 12.1% incidence of elevated trimester-specific TSH in a targeted screening and 12.6% in an unselected screening group. The cutoff value was 2.5 mIU/L according to the guidelines from the Endocrine Society (ES), 15 but the incidence is similar to what is seen in the present study where 2.0 mIU/L was used. Männistö et al. performed a prospective study of a large cohort in Finland (the northern Finland birth cohort), but only 61% of samples were analyzed. In their study, the incidence of SCH was 3.9% and hypothyroidism 0.9%, which is considerably lower than that found in the present study and in the previous Swedish study. 15,20 The reason for the discrepancy with the Finnish results may be due to the samples being stored for 20 years before analysis or that the cutoff value was set to 3.9 mIU/L. However, this could also be due to population differences, or it could be that the incidence of SCH is lower in Finland than in Sweden.
It is also remarkable that half of the women with known hypothyroidism were treated with an inappropriately low dose of LT4. Thus, it is evident that a high number of women do not receive the treatment they need. The fetal thyroid gland begins to incorporate iodine late in the first trimester of pregnancy, but the fetus does not start to secrete its own thyroid hormones until the 18th to 20th week of pregnancy; therefore, the fetus is totally dependent on the circulation of maternal thyroid hormone levels. 21
The maternal production of thyroxin increases by 30%–50% from the fifth week of pregnancy. Women with known hypothyroidism usually need to increase their dose of LT4 during the first trimester. 22 However, the present study showed that the group of hypothyroid women receiving LT4 were inadequately treated in 50% of cases. Our findings are in agreement with studies by Hallengren et al. and Vadiveloo et al., who reported that 30% of women on LT4 substitution had elevated TSH levels during early pregnancy. 23,24
This indicates a need to improve thyroid management both before and during early pregnancy. Primary healthcare providers, who are responsible for prescribing LT4, should inform these women about the need for early adjustment of LT4 treatment during pregnancy and recommend measuring their TSH serum level as soon as pregnancy is confirmed.
Socioeconomic factors differ between the two antenatal care units, which might be a reason why there are more women smoking in south of Stockholm. The numbers of smokers was slightly higher, and although a meta-analysis found a trend toward increased risk for hypothyroidism, 25 the number is too small to influence the results of the present study.
The women in the low-risk group were slightly younger than the women in the high-risk group, which might affect the outcome. However, a recent Spanish study on 2509 pregnant women showed that the prevalence of thyroid dysfunction does not increase with maternal age. 26 Therefore, the age difference is not likely to influence the results of the present study.
A weakness of the study is that not all women were initially selected as being at risk of thyroid disease at the antenatal care unit. Another weakness of the study is that, due to the low number of treated women in the study and the lack of a control group of untreated women, it is not possible to draw conclusions on the effect of treatment. However, for ethical reasons, it was not possible to leave the women in need of LT4 untreated. Pregnancy outcome was not the main objective of the study. Another limitation was that free T4 was not assessed until after initiation of LT4 treatment, and therefore, the effects of maternal hypothyroxinemia were not assessed.
The major strength of this study is that the study population was representative of all pregnant women in Sweden. A cross linking of the Swedish Medical Birth Register and the Pregnancy Register showed that almost all pregnant women in Sweden are registered in antenatal care units during pregnancy.
According to ES clinical practice guideline 2012 and European Thyroid Association (ETA) guidelines 2014, all pregnant women with SCH (TSH >2.5 mIU/L) should be treated with LT4 before conception and during pregnancy. 11 –13 However, according to local clinical guidelines in Stockholm, all pregnant women in the present study with serum TSH above 2.0 mIU/L (n = 81, 13.5%) were treated with LT4 from the first trimester of pregnancy and were monitored throughout pregnancy. These women had an incidence of pregnancy and delivery complications similar to what could be expected in a healthy population without SCH. However, the number of study subjects was low, so more data are needed to verify this conclusion.
Conclusions
It can be concluded that screening only high-risk women in their first trimester of pregnancy fails to detect almost 10% of pregnant women who have SCH and overt hypothyroidism. Therefore, general screening for TSH in early pregnancy may be appropriate, and should be verified by future adequately powered randomized controlled trials. Furthermore, to facilitate sufficient treatment of women with known hypothyroidism, serum TSH levels should be analyzed at antenatal care units as soon as pregnancy is confirmed.
Footnotes
Acknowledgments
The authors appreciate the valuable comments and discussions of Jan Calissendorff, Rickard Ljung, and the late Danuta Gross Witkow and the statistical assistance provided by Fredrik Johansson. The study was financed by the Department of Obstetrics and Gynecology, Danderyd University Hospital, Stockholm, Sweden. The authors thank the Department of Obstetrics and Gynecology at Danderyd University Hospital, Stockholm for providing funding for this project.
Author Disclosure Statement
No competing financial interests exist