
Abstract
Background:
Body mass index (BMI) and endometriosis have been inversely associated. To address gaps in this research, we examined associations among body composition, endometriosis, and physical activity.
Materials and Methods:
Women from 14 clinical sites in the Salt Lake City, Utah and San Francisco, California areas and scheduled for laparoscopy/laparotomy were recruited during 2007–2009. Participants (N = 473) underwent standardized anthropometric assessments to estimate body composition before surgery. Using a cross-sectional design, odds of an endometriosis diagnosis (adjusted odds ratio [aOR]; 95% confidence interval [CI]) were calculated for anthropometric and body composition measures (weight in kg; height in cm; mid upper arm, waist, hip, and chest circumferences in cm; subscapular, suprailiac, and triceps skinfold thicknesses in mm; arm muscle and fat areas in cm2; centripetal fat, chest-to-waist, chest-to-hip, waist-to-hip, and waist-to-height ratios; arm fat index; and BMI in kg/m2). Physical activity (metabolic equivalent of task-minutes/week) and sedentariness (average minutes sitting on a weekday) were assessed using the International Physical Activity Questionnaire-Short Form. Measures were modeled continuously and in quartiles based on sample estimates. Adjusted models were controlled for age (years, continuous), site (Utah/California), smoking history (never, former, or current smoker), and income (below, within 180%, and above of the poverty line). Findings were standardized by dividing variables by their respective standard deviations. We used adjusted models to examine whether odds of an endometriosis diagnosis were moderated by physical activity or sedentariness.
Results:
Inverse relationships were observed between endometriosis and standardized: weight (aOR = 0.71, 95% CI 0.57–0.88); subscapular skinfold thickness (aOR = 0.79, 95% CI 0.65–0.98); waist and hip circumferences (aOR = 0.79, 95% CI 0.64–0.98 and aOR = 0.76, 95% CI 0.61–0.94, respectively); total upper arm and upper arm muscle areas (aOR = 0.76, 95% CI 0.61–0.94 and aOR = 0.74, 95% CI 0.59–0.93, respectively); and BMI (aOR = 0.75, 95% CI 0.60–0.93), despite similar heights. Women in the highest versus lowest quartile had lower adjusted odds of an endometriosis diagnosis for: weight; mid-upper arm, hip, and waist circumferences; total upper arm and upper arm muscle areas; BMI; and centripetal fat ratio. There was no evidence of a main effect or moderation of physical activity or sedentariness.
Conclusion:
In a surgical cohort, endometriosis was inversely associated with anthropometric measures and body composition indicators.
Introduction
A
Researchers have questioned whether body composition as indicated by BMI has an etiologic role or is a reflection of other factors that may be associated with the development of endometriosis, such as physical activity, parity, or cigarette smoking. 7,11,13 –19 Nevertheless, BMI has been associated with gynecological functioning. Underweight young adult women are at increased risk for menstrual dysfunction relative to normal weight women 20 while women who are overweight are at increased risk for various gynecological disorders, including menstrual dysfunction 20 and impaired fecundity. 21
Despite its near universal acceptance as a proxy for body composition (i.e., level of adiposity), BMI does not directly measure body composition, especially the amount and distribution of adipose and muscle tissue. Tissue type in the context of obesity is important to distinguish; the biological activity of adipose and muscle tissue depends on the amount, distribution, 22 and type of muscle fiber, which differs based on amount of adipose tissue. 23
A more accurate measurement of body composition to distinguish between adipose tissue and muscle mass requires anthropometric or other more specialized assessments (e.g., dual-energy x-ray absorptiometry [DXA], bioelectric impedance, or hydrostatic weighing). 24 Anthropometry and some types of specialized assessments, such as DXA, may also capture the location and regional distribution of adipose tissue, 25 which may be informative about the pathophysiology of endometriosis.
In addition, much of the research on the relationship between BMI and endometriosis has not considered physical activity, although such activity has been associated with endometriosis in some 11,13,14,19 but not all studies. 26,27 In addition, physical activity and BMI have associated in a bidirectional relationship. 28 However, the relationships among physical activity, BMI, and disease are unclear. 29
To address the gaps in current research regarding body habitus and endometriosis, we assessed the relationship between anthropometric body composition indicators and a surgical diagnosis of endometriosis. We used anthropometric measures, body composition indicators, and body fat distribution ratios. In addition, we investigated whether physical activity may moderate the association between body composition and endometriosis.
Material and Methods
Study design and populations
Data were used from the Endometriosis, Natural History, Diagnosis and Outcomes (ENDO) Study; these methods have been described elsewhere. 1 Our study sample comprised 475 women scheduled for gynecologic laparoscopy or laparotomy irrespective of surgical indication (e.g., pelvic pain, pelvic mass, and menstrual irregularities) from 14 clinical sites located in the Salt Lake City, Utah and San Francisco, California metropolitan areas between 2007 and 2009. Eligibility criteria were as follows: aged 18–44 years, currently menstruating, no history of cancer except for nonmelanoma skin cancer, no breastfeeding for 6 months or more, and no injectable hormone treatment within the past 2 years. By design, women with previously surgically visualized endometriosis (prevalent disease) were excluded to capture incident diagnoses. Two women cancelled their surgeries resulting in a sample of 473 women.
Data collection and operational definitions
Upon enrollment and ∼2 months before surgery, trained research staff conducted in-person computer-assisted interviews with women to capture sociodemographic, lifestyle, and medical history information. Next, staff performed standardized anthropometric assessments with a protocol, 25 as illustrated in Figure 1a. The following measurements were taken using calibrated and certified equipment: height (centimeters; cm) using a fixed stadiometer (214 Road Rod portable stadiometer [seca Corporation, Hamburg, Germany; US office, Hanover, MD] or the wooden Shorr Board [Shorr Productions, Olney, MD]); weight (kilograms; kg) using a balance scale; triceps, subscapular, and suprailiac skinfold thicknesses (millimeters; mm) using a Lange Skinfold Caliper (Beta Technology, Inc., Santa Cruz, CA); and mid-upper arm, waist, and hip body circumferences (cm) using tape measures. Chest circumference (cm) was estimated from self-reported bra size using well-established algorithms. 30 Bra size was used instead of directly measuring chest size to (a) decrease women's discomfort that could arise when measuring around the chest and (b) address variability in the possible position of breasts on the chest. Waist circumference measurements were taken at the natural indentation of the waist. 25 To maximize reliability, all measurements were taken twice. If the first two measurements differed by ≥0.5 cm for height, ≥0.1 kg for weight, ≥4 mm for any skinfold thickness, or ≥0.5 cm for body circumferences, then a third measurement was taken.
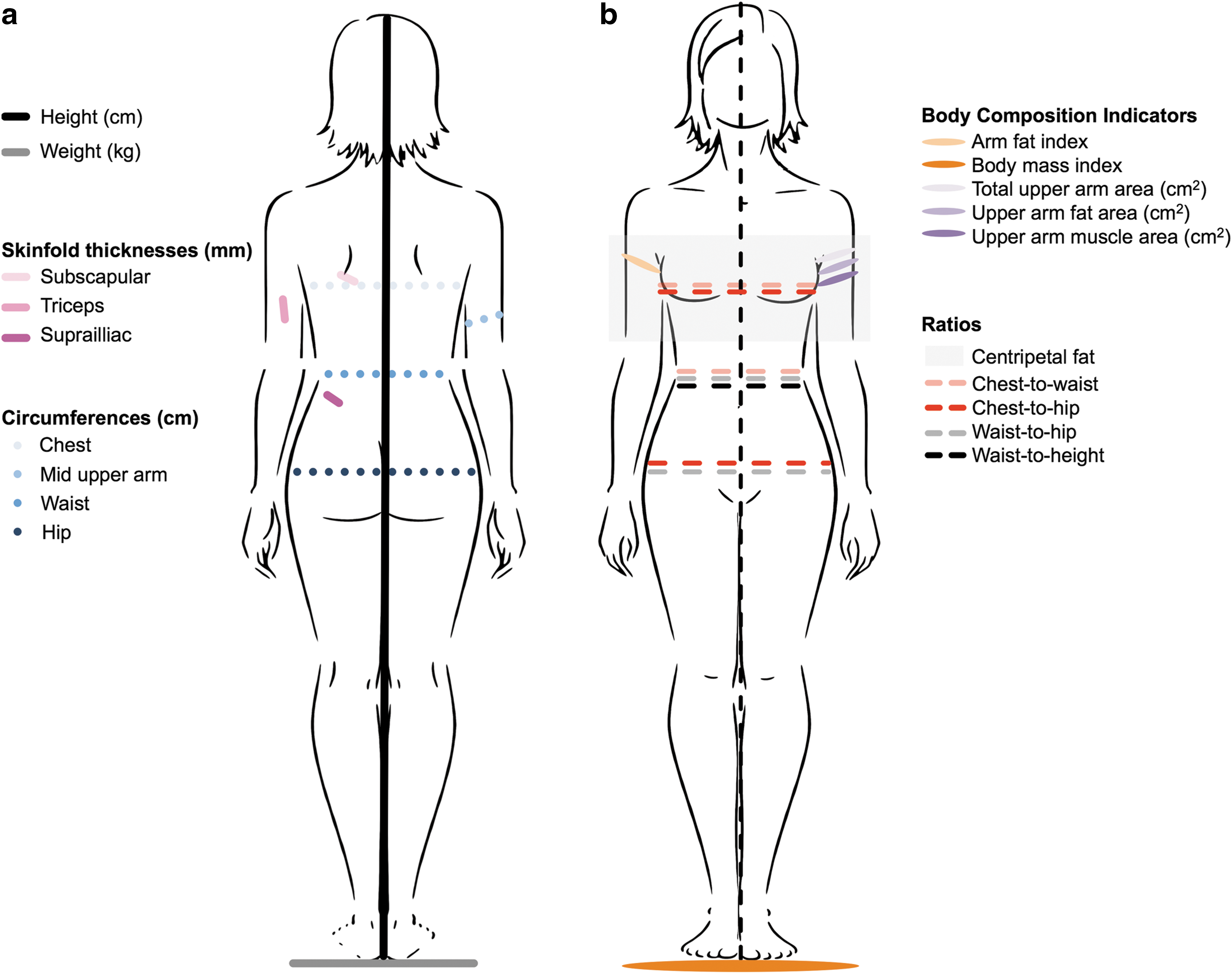
Anthropometric measurements were averaged for analysis and then converted to various indicators of muscularity and adiposity (described below), called body composition indicators hereon in this article. 31 –33 Body circumferences were used to derive ratios indicating body fat distribution. Body composition indicators and body fat distribution ratios are illustrated in Figure 1b. Formulas used to derive body composition indicators are as follows: arm fat index = (upper arm fat area/total upper arm area) × 100; BMI = weight (kg)/height (m)2; total upper arm area = mid upper arm circumference (cm)2/(4 × π); upper arm fat area = total upper arm area − upper arm muscle area; upper arm muscle area = ([mid upper arm circumference(cm)] − [(triceps skinfold thickness[cm]) × π]2)/(4 × π). BMI categories were defined as follows: underweight <18.5 kg/m2; normal weight ≥18.5 and ≤25.0 kg/m2; overweight ≥25.0 and ≤30 kg/m2; and obese ≥30 kg/m2. 34 Formulas used to derive body fat distribution ratios were as follows: centripetal fat = subscapular skinfold thickness (mm)/(subscapular skinfold thickness [mm] + triceps skinfold thickness [mm]); chest-to-waist = chest circumference (cm)/waist circumference (cm); chest-to-hip = chest circumference (cm)/hip circumference (cm); waist-to-hip = waist circumference (cm)/hip circumference (cm); and waist-to-height = waist circumference (cm)/height (cm).
Women completed the International Physical Activity Questionnaire-Short Form (IPAQ-SF) to assess degree of physical activity and inactivity. 35 The IPAQ-SF captures physical activity as frequency (days), duration (hours and minutes), and intensity of physical activity, which were used to compute metabolic equivalent of task (MET)-minutes of weekly physical activity (continuous). Importantly, the IPAQ enabled us to assess inactivity as frequency (days) and duration (hours and minutes) sitting on a weekday (continuous) to assess sedentariness. 28,35 Finally, women provided serum samples to assess serum cotinine (ng/mL) as a biomarker of current nicotine exposure; this measure can differentiate active from either passive or no cigarette smoking. The institutional review boards for all participating sites approved this study. Participants gave written informed consent before enrollment and any data collection.
Endometriosis diagnosis
Endometriosis was defined as disease visualized during surgery, which is the U.S. gold standard. 36,37 Surgeons completed standardized operative reports specifically designed to capture postsurgical diagnoses and accompanying morbidity. The report also included the revised American Society for Reproductive Medicine (r-ASRM) scoring system for staging endometriosis, which was categorized as follows: stage I/minimal (scores 1–5); stage II/mild (scores 6–15); stage III/moderate (scores 16–40); or stage IV/severe (scores ≥40). 38 The inter-rater agreement for postoperative diagnosed endometriosis among specialized expert surgeons in this study was good (Fleiss kappa = 0.69, 95% confidence interval [CI] 0.64–0.74). 39
Statistical analysis
The descriptive phase of the analysis included inspection of data for completeness and distributions. Missing data were minimal for anthropometric data (n ≤ 11) and IPAQ-SF (n = 91) and were missing at random. To minimize potential bias, we addressed missing physical activity data by imputing the mode for the same activity type among women with the same endometriosis diagnosis. 40
We examined associations between anthropometric measures and endometriosis status using the Wilcoxon nonparametric rank-sum and Fisher's exact tests for continuous and categorical variables, respectively. We utilized logistic regression analysis to model each anthropometric measurement in relation to the odds of an endometriosis diagnosis adjusting for age (continuous) and site (Utah/California), as well as smoking history (never, former, or current smoker) and income (below, within 180%, and above of the poverty line) based on prior research, 41 –47 and because the added confounders changed the beta coefficient of the adiposity variables by more than 10% when included in our models. 48 To support interpretability of the findings for continuous variables, we standardized the variables by dividing them by their respective standard deviations (the resulting unit for these variables is one standard deviation). We assessed associations between odds of an endometriosis diagnosis and anthropometric and body composition measures continuously and as quartiles based on sample estimates (first quartile as the reference).
We empirically assessed the main effects of physical activity and sedentariness and for potential effect modification between anthropometric and body composition measures and both physical activity (weekly MET-minutes) and sedentariness (average weekday minutes spent sitting). We assessed for significant changes in the adjusted odds ratio (aORs) and accompanying 95% CIs. When we assessed potential moderation, we used hierarchical clustering methods to identify a reduced set of anthropometric measures that were most strongly associated with odds of an endometriosis diagnosis within each cluster to minimize multicollinearity. To investigate if pain could be a confounding factor for physical activity engagement, we assessed for differences in self-reported chronic or cyclic pain by endometriosis diagnosis among different activity levels (high, moderate, and low as indicated by the IPAQ-SF).
We conducted sensitivity analyses to assess the robustness of our findings. This included assessing for significant changes in findings based on choice of comparison group. We compared women with endometriosis to women with a (a) postoperative diagnosis of a normal pelvis (no pathology found) and (b) specific gynecologic disorder, fibroids. Other supporting analyses included using categorized measurements for waist circumference, waist-to-hip ratio, waist-to-height ratio, and BMI, 31,33,34,49 –51 replacing self-reported smoking with serum cotinine concentrations modeled continuously and categorically (none [9–9.99 ng/mL], passive [10.00–99.99 ng/mL], and active [100.00–595.31 ng/mL] exposure), 52 and restricting physical activity analyses among participants for whom data were not imputed. Finally, we assessed model fit and whether the anthropometric measures and body composition measures increased explained variance beyond BMI and weight as measured by Pseudo R2 values, which estimate goodness of fit. All analyses were performed using either Stata (v. 11; College Station, TX) or SAS (v. 9.4; Cary, NC).
Results
Compared with participants without endometriosis, affected women were younger and more likely to be nulligravida, nulliparous, and nonsmokers, have lower cotinine concentrations, and reside in households above the poverty line (Table 1). Overall, women with endometriosis had lower adiposity and lower muscle mass compared with women without endometriosis (Table 2). Preoperative diagnoses for surgery were as follows: pelvic pain (n = 206, 42%), pelvic mass (n = 74, 15%), menstrual irregularities (n = 60, 12%), fibroids (n = 49, 10%), tubal ligation (n = 48, 10%), and infertility (n = 35, 7%). The incidence of endometriosis was 40% (n = 190) and varied from 50% of women with stage 1%–21% with stage 2, 18% with stage 3, and 11% with stage IV. About 31% of women were diagnosed with other gynecologic pathologies (e.g., uterine fibroids, pelvic adhesions, and benign ovarian cysts) while 29% had postoperative diagnoses of a normal pelvis.
p < 0.05. Significance for the bivariate analyses was assessed using the Wilcoxon nonparametric rank-sum and Fisher's exact tests for continuous and categorical variables, respectively.
MET, metabolic equivalent of task; SD, standard deviation.
P < 0.05. Significance for bivariate analyses was assessed using the Wilcoxon nonparametric rank-sum and Fisher's exact tests for continuous and categorical variables, respectively.
Arm fat index = (upper arm fat area/total upper arm area) × 100.
Body mass index = [weight (kg)]/[height2 (m2)].
Presented as number (%). Body mass index categories were defined as: underweight <18.5 kg/m2, normal weight 18.5–24.5 kg/m2, overweight 25–29.9 kg/m2, and obese ≥30 kg/m2 (National Health, Lung, and Blood Institute, 1998).
Total upper arm area = [mid upper arm circumference (cm)2]/(4 × π).
Upper arm fat area = [total upper arm area − upper arm muscle area].
Upper arm muscle area = ([mid upper arm circumference (cm)] − [(triceps skinfold thickness [cm]) × π]2)/(4 × π).
Centripetal fat ratio = [subscapular skinfold thickness (mm)]/([subscapular skinfold thickness (mm)] + [triceps skinfold thickness (mm)]).
Chest-to-waist ratio = [chest circumference (cm)]/[waist circumference (cm)].
Chest-to-hip ratio = [chest circumference (cm)]/[hip circumference (cm)].
Waist-to-hip ratio = [waist circumference (cm)]/[hip circumference(cm)].
Waist-to-height ratio = [waist circumference (cm)]/[height (cm)].
The odds of an endometriosis diagnosis were inversely associated with several anthropometric measures and body composition indicators in adjusted models (Table 3). These measures and indicators included standardized: weight (aOR = 0.71, 95% CI 0.57–0.88); subscapular skinfold thickness (aOR = 0.79, 95% CI 0.65–0.98); mid-upper arm, waist, and hip circumferences (aOR = 0.76, 95% CI 0.61–0.93, aOR = 0.79, 95% CI 0.64–0.98, and aOR = 0.76, 95% CI 0.61–0.94, respectively); total upper arm and upper arm muscle areas (aOR = 0.76, 95% CI 0.61–0.94 and aOR = 0.74, 95% CI 0.59–0.93, respectively); and BMI (aOR = 0.75, 95% CI 0.60–0.93).
Continuous variables are standardized (variables divided by their respective standard deviation. Original units: weight in kg; height in cm; mid-upper arm, waist, hip, and chest circumferences in cm; subscapular, suprailiac, and triceps skinfold thicknesses in mm; arm muscle and fat areas in cm2; and body mass index in kg/m2. Standardized by dividing variables by their respective standard deviation. Standardized unit = one standard deviation. Bold numbers indicate significant findings.
Odds ratios (ORs) adjusted for age in years (continuous), smoking history (never, former, or current smoker), income (below, within, or above the poverty line), and site (California/Utah).
In original units. Body mass index categories were defined as: underweight <18.5 kg/m2, normal weight 18.5–24.5 kg/m2, overweight 25–29.9 kg/m2, and obese ≥30 kg/m2. 34
CI, confidence interval; OR, odds ratio.
Women in the highest quartiles for several anthropometric measurements, body composition indicators, and body fat distribution ratios had lower adjusted odds of an endometriosis diagnosis than those in the lowest quartile (Fig. 2). These measures, indicators, and ratios included: weight; mid upper arm, hip, and waist circumferences; total upper arm and upper arm muscle areas; BMI; and centripetal fat ratio. Quartile ranges for anthropometric and body composition measures related to first, second, third, and fourth quartiles, respectively, were as follows: Subscapular skinfold thickness ≤13.00, 13.00−20.00, 20.00−30.00, ≥30.00; Suprailiac skinfold thickness ≤13.00, 13.00−22.20, 22.20−33.20, ≥33.20; Triceps skinfold thickness ≤22.00, 22.00−28.60, 28.60−35.00, ≥35.00; Height ≤160.8, 160.8−165.0, 165.0−169.8, ≥169.8; Mid-upper arm circumference ≤27.20, 27.20−30.40, 84.00−98.20, ≥35.00; Chest circumference ≤78.06, 8.06−83.86, 83.86−91.42, ≥91.42; Waist circumference ≤74.60, 74.60−84.00, 84.00−98.20, ≥98.20; Hip circumference ≤98.00, 98.00−106.0, 106.0−117.8, ≥117.8; Waist-to-hip ratio ≤0.74, 0.74−0.79, 0.79−0.85, ≥0.85; Chest-to-waist ratio, ≤0.92, 0.92−1.00, 1.00−1.08, ≥1.08; Chest-to-hip ratio ≤0.75, 0.75−0.79, 0.79−0.83, ≥0.83; Waist-to-height ratio ≤0.45, 0.45−0.51, 0.51−0.59, ≥0.59; BMI ≤22.00, 22.00−26.00, 26.00−31.60, ≥31.60; Total upper arm area ≤58.87, 58.87−73.54, 73.54−97.48, ≥97.48; Upper arm muscle area ≤30.14, 30.14−37.35, 37.35−47.95, ≥47.95; upper arm fat area ≤26.68, 26.68−36.95, 36.95−50.34, ≥50.34; Arm fat index ≤42.17, 42.17−48.19, 48.19−53.64, ≥53.64; and Centripetal fat ratio ≤0.35, 0.35−0.43, 0.43−0.49, ≥0.49.
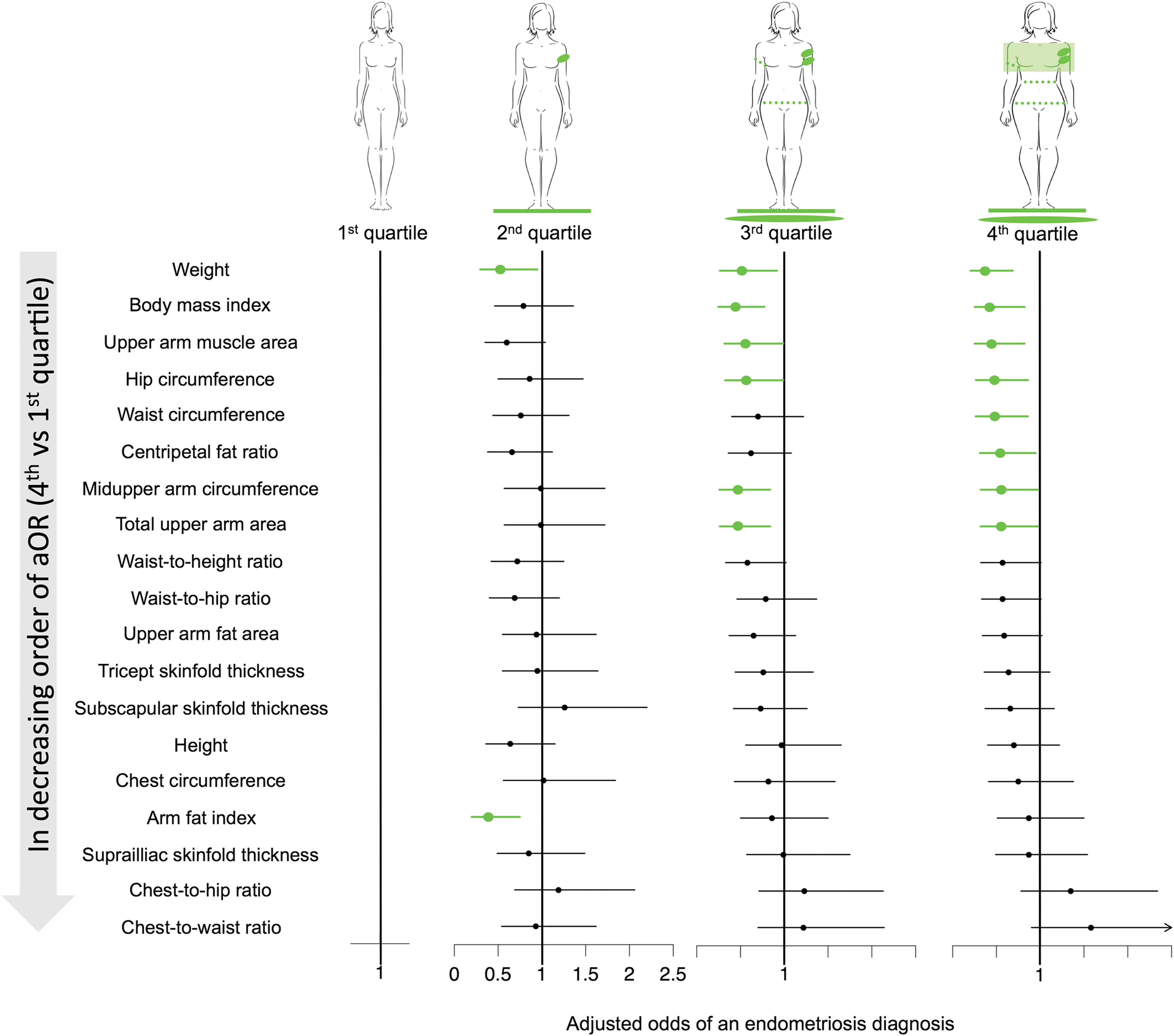
Anthropometric measurements in quartiles and adjusted odd ratios of endometriosis. Green indicates significant findings.
There was no evidence of a main effect of physical activity or sedentariness (data not shown). There was also no evidence of moderation between anthropometric and body composition measures and both physical activity and sedentariness (data not shown). We observed no differences by endometriosis diagnosis status for all but one comparison (data not shown); the sole exception was that among women who reported engaging in “high” physical activity, those with endometriosis were more likely to report cyclic pain compared to women without endometriosis; n = 46 (46.5%) and n = 35 (24.0%), respectively. Significance of the findings was lost when restricting the comparison group to either having fibroids or no pathology, yet general patterns were still observed in that aOR's remained ≤1.0. For the adjusted models, Pseudo R2 values were between 0.0545 and 0.0757. There was no significant improvement in explained variation when accounting for anthropometric and body composition measures beyond weight and BMI (data not shown). All findings were upheld in sensitivity analyses.
Discussion
In the first study known to us to use multiple anthropometric measurements to assess adiposity and muscle mass, we observed inverse relationships between body composition measures and odds of endometriosis without effect modification from physical activity. Findings were similar across standardized continuous measures and measures in quartiles. Although previous researchers have reported an inverse association between BMI and endometriosis, our study is the first to suggest that being lean in adipose tissue and muscle mass are associated with greater odds of an endometriosis diagnosis. Our findings are strengthened by our assessment of body composition with standardized anthropometric measures and our definition of endometriosis using the United States gold standard of surgical visualization.
Using data from a study that had an exposure cohort design, we found that women without endometriosis had greater adiposity and upper arm muscle mass than women with the disease. Our findings corroborate earlier findings of inverse associations between body compositions as measured by BMI 7 or self-measured waist-to-hip ratio 53 and endometriosis as measured via surgical visualization or self-reported physician diagnosed, respectively. In addition, in adjusted models, we found an absence of a relationship between waist-to-hip ratio and endometriosis diagnosis; these findings are similar to those in a study that included friend controls and an operative sample. 54
Our novel research suggests that a more nuanced understanding of body composition–adipose tissue amount and distribution, as well as muscle mass–might help characterize gynecologic disease risk, as opposed to simpler and more global measures of obesity, such as BMI. Many researchers who study obesity use BMI as a measure, including in the context of gynecologic disease. For example, low BMI appears to be protective against ovarian cancer in premenopausal women. 55 However, we found that low adiposity was associated with disease: women with endometriosis were more likely to be lean than women without endometriosis. Interestingly, women with endometriosis have the same or greater risk for ovarian cancer than women without endometriosis. 56 –58 We suggest that future researchers could advance understanding of relationships between obesity and gynecologic disease by looking more precisely at body composition rather than BMI alone. In our study, low BMI was associated with increased odds of an endometriosis diagnosis. When considering estimates for body composition, adiposity measures were not only inversely associated with endometriosis but also with muscle mass. Thus, by looking at estimates of both adipose tissue and muscle mass, we provide a more comprehensive understanding of what tissue types may contribute to the increased odds of an endometriosis diagnosis.
By studying body composition, researchers and healthcare providers may gain understanding of disease mechanisms. Questions for future research include: why is leanness not protective in endometriosis whereas it is in other gynecologic diseases? How can clinicians assess patients for endometriosis risk more effectively? To date, there are no known biomarkers or noninvasive diagnostic methods of incident endometriosis suitable for population research or clinical care. 59 –62 Body composition provides another means for researchers to investigate potential involvement of an altered adipose tissue milieu in endometriosis characterized by a different immunological profile 63 –66 or omental fat protease expression. 67 –70 Studying body composition also could open new research avenues into the role of muscle mass in mechanisms related to the development of endometriosis.
Clinicians could benefit from recognizing that the extremes in body composition may have implications for gynecologic diseases, with a lean body habitus now being associated with endometriosis building upon long-standing recognition that obesity is associated with polycystic ovarian syndrome. 71 Healthcare providers could also consider incorporating anthropometric measures of adiposity and muscle mass that could offer a more global understanding of women's disease risk profile. Incorporating body composition into clinical decision-making could be helpful given that no screening tools exist and the only way to definitively diagnose endometriosis is via surgery.
Despite the study's many strengths, careful interpretation of the findings is needed relative to important study limitations, most notably its cross-sectional analysis. The natural history of endometriosis is unknown; it is possible that body habitus, physical activity, and sedentariness in childhood and/or adolescence are important to the development of endometriosis, 11 consistent with a possible in utero origin for endometriosis. 72,73 In addition, while measurements were taken about 2 months before surgery, women were unaware of their postoperative diagnoses at the time of measurement. This is an important consideration for self-reported data, including bra size, given the potential for reporting errors. 74 Another key limitation is reliance on a clinical population comprising women who sought care and underwent surgery. The extent to which the findings are upheld at the population level remain to be established, particularly because 11%, or more, of women may have unrecognized disease. 1 As is the case with observational research in general, we recognize the potential for residual confounding. This includes variables related to behaviors, including dietary intake, a factor important for body composition and for which we had little data, and disease related symptoms such as pain, which was likely not a factor in our sample given that we observed no differences in pain and physical activity engagement by endometriosis diagnosis status.
Conclusions
Using established protocols for assessing body composition and endometriosis, we found that a lean body habitus is associated with endometriosis, when controlling for potential confounders and considering physical activity. This study is the first, to our knowledge, to include comprehensive anthropometric assessments to assess adiposity, as well as muscle mass, thereby overcoming limitations from previous research. Our research can support future research into mechanisms of the disease, which could support our understanding of the role of body composition in development of disease and the care of women at risk for developing or diagnosed with endometriosis.
Footnotes
Acknowledgments
The authors gratefully acknowledge Denise Lamb, RN, Study Coordinator and other study personnel for their attention to quality when collecting these data. Sponsorship: The study was funded by the Intramural Research Program, Eunice Kennedy Shriver National Institute of Child Health and Human Development (NICHD), National Institutes of Health (NIH) (contracts NO1-DK-6-3428; NO1- DK-6-3427; 10001406-02). Dr. Backonja was funded as a doctoral fellow through the NIH/National Institute of Nursing Research (NINR) Graduate Partnership Program and as a postdoctoral fellow through the NIH, National Library of Medicine (NLM) Biomedical and Health Informatics Training Program at the University of Washington (Grant No. T15LM007442).
Author Disclosure Statement
None of the authors have any commercial associations that might create a conflict of interest in connection with submitted article.