
Abstract
Background:
Low-income Hispanic women experience elevated rates of high postpartum weight retention (PPWR), which is an independent risk factor for lifetime obesity. Sociocultural factors might play an important role among Hispanic women; however, very few studies have examined this association.
Objective:
The purpose of our study was to examine the associations between acculturation and maternal diet, physical activity, and PPWR.
Design:
This is a cross-sectional study of baseline data from 282 Hispanic women participating in the FitMoms/Mamás Activas study, a randomized controlled trial examining the impact of primarily an internet-based weight control program, in reducing PPWR among low-income women. We performed multivariable linear regression to examine the association of acculturation with diet quality, physical activity, and PPWR at study entry.
Results:
A total of 213 (76%) women had acculturation scores reflecting Mexican orientation or bicultural orientation, whereas 69 (24%) had scores that represented assimilation to Anglo culture. Women who were more acculturated had lower intakes of fruits and vegetables, lower HEI scores, and lower physical activity levels than women who were less acculturated (p < 0.05). We found an association between acculturation and PPWR in that for every 1-unit increase in acculturation score, PPWR increased, on average, by 0.80 kg.
Conclusion:
Higher acculturation was associated with poorer diet and physical activity behaviors and greater PPWR.
Introduction
H
Hispanic immigrants tend to have better health upon arrival to the U.S. compared with U.S.-born individuals; however, this health advantage appears to diminish over time. 14 –16 In fact, the rates of many health outcomes for Hispanic immigrants converge to the rates of U.S.-born individuals as the beliefs and practices of U.S. culture are adopted. 17 This process, known as acculturation, is multidimensional and influences lifestyle behaviors, such as diet, physical activity, and obesity, 18,19 and might contribute to increased PPWR among Hispanic women.
Epidemiologic research suggests that greater acculturation, based on proxy measures, including place of birth, generation status in the U.S., and duration of residency in the U.S., is associated with higher weight gain during pregnancy. 20 –22 However, to our knowledge, only one study has directly assessed the association between acculturation and PPWR among Hispanic women and no association was found. 20 Previous research is limited by the use of single proxy indicators to measure acculturation and lack of validated measures of diet and physical activity. Hispanic practices differ across Hispanic ethnic groups making generalizations across heterogeneous Hispanic populations difficult. Therefore, the objective of our study was to expand upon the limited evidence by examining the association between acculturation and PPWR among Hispanic postpartum women primarily of Mexican descent using an improved, multidimensional acculturation scale and objective measures of diet and exercise. Because acculturation is associated with lifestyle factors (e.g., diet and physical activity), we will also explore the mediating role of postpartum diet and physical activity on the association between acculturation and PPWR.
Materials and Methods
Study design and population
We utilized baseline data from FitMoms/Mamás Activas, a randomized controlled trial examining the effects of primarily an internet-based weight control program, in reducing PPWR in low-income women participating in Women, Infants, and Children (WIC) Nutrition Program. 23 Participants were women recruited from 12 WIC clinics in California (six in Santa Barbara county, four in San Luis Obispo county, and two in Ventura county) between 2013 and 2015 (n = 371). Eligibility criteria included currently being overweight/obese with a BMI >25 kg/m2 or having a BMI between 22 and 24.9 and exceeding prepregnancy weight by at least 4.5 kg (10 lbs.), 24 adult (age >18 years), fluency in English or Spanish, between 6 weeks and 12 months postpartum, and without major psychiatric or medical problems. Women were only included in the analysis if they had complete data for PPWR, acculturation level, dietary intake, and physical activity (n = 349; 94%). All mothers provided written informed consent and all procedures were conducted in accordance with ethical standards for human experimentation. The study was approved by the Institutional Review Board at California Polytechnic State University.
Measures
Assessments were conducted by blinded, bilingual assessors at study entry. Questionnaires were selected based on their prior validity and use in English- and Spanish-speaking postpartum populations. Participants were provided with a $25 honorarium for completing the baseline assessments.
Demographic measures
Participants completed a questionnaire at study entry assessing age, race, ethnicity, nativity, duration of U.S. residency, parity, income, education, food insecurity, breastfeeding, and smoking status.
Acculturation
Acculturation was measured using the Acculturation Rating Scale for Mexican Americans–Version II (ARMSA-II), which assesses an individual's preference for Spanish or English media and contact with their country of origin and people of Latino and Anglo backgrounds using multiple domains of behaviors, identity, and interpersonal relationships. 25 The ARSMA-II can be scored by calculating the difference between the mean of the non-Hispanic White American Oriented Scale of the ARSMA-II and the mean of the Mexican Oriented Scale of the ARMSA-II (range: −4 to 4; mean ± SD of 0.12 ± 2.53). The scores are then converted into five levels of acculturation ranging from 1 to 5 (5 representing most acculturated to Anglo-American orientation). 25
Anthropometric measures
PPWR was calculated as the difference between maternal weight at study entry and prepregnancy weight. Weight at study entry was measured to the nearest 0.1 kg using a calibrated standard digital scale. Two measures are completed with participants weighed in light clothing (without shoes). Standing height was measured twice in patients without shoes in millimeters with a wall-mounted Harpenden stadiometer at WIC clinics. Prepregnancy weight was based on self-report at the time of last menstrual period. 26,27 Total gestational weight gain (GWG) was also self-reported by study participants.
Dietary intake and physical activity
Dietary intake was assessed using 24-hour recalls on 2 random days over a week
28
–30
and completed using the National Cancer Institute (NCI) Automated Self-Administered 24-hour recall (ASA-24;
The 2010 Healthy Eating Index (HEI-2010) was used to assess postpartum diet quality, which is comprised of 12 components (total fruit, whole fruit, total vegetables, greens and beans, whole grains, dairy, total protein foods, seafood and plant proteins, fatty acids, refined grains, sodium, and empty calories). Component scores were calculated directly from the ASA24 data files using the HEI SAS macro provided by NCI (
The ActiGraph GT3X+ (The ActiGraph, Pensacola, FL) accelerometer was used to measure maternal physical activity. The monitor samples time-varying accelerations ranging from ±6 g's at a user-defined rate. The monitors (firmware v2.4.0) were initialized to sample triaxial acceleration at 40 Hz, and data were stored in flash memory on the device until it was downloaded to a computer. Data were initially processed using ActiLife software (v6.11.7). The proprietary software was used to filter the raw data using the low-frequency filter and averaged over 1-second epochs. Data were then exported to comma-separated values files. The remaining processing was completed using a program written in SAS (v9.4 SAS Institute, Cary, NC). Participants were instructed to wear the accelerometer on their waist of their nondominant side for 5–7 days, and were allowed to take it off while sleeping. Wear time was determined using the Choi algorithm. 32 Accelerometer wear time was required to be ≥10 hours per day to be included in the analysis, and total minutes in light and moderate-to-vigorous physical activity were calculated. 33
Statistical analysis
Because the primary focus of our study was the impact of assimilation to U.S. culture, we excluded women from our analysis who did not self-identify as Hispanic (n = 67) resulting in a final analytic sample size of 282. For descriptive purposes only, women were categorized into two groups based on their acculturation level: (1) very or strongly assimilated, defined as acculturation score >3; and (2) bicultural or less assimilated, defined as acculturation score ≤3. This categorization is in line with the ARSMA-II scoring metric used to differentiate Mexican Americans who are either very or strongly assimilated to Anglo culture and Mexican Americans who are less assimilated or bicultural. 25 We compared selected baseline characteristics, dietary intake, physical activity, and pregnancy-related weight by acculturation using two-tailed chi-square tests for categorical variables and one-way analysis of variance for continuous variables. p < 0.05 was considered statistically significant.
We examined the extent to which acculturation (continuously) was associated with dietary intake (total energy intake and HEI-2010), physical activity (total minutes of moderate-to-vigorous physical activity [MVPA], total light minutes of physical activity, total minutes of sedentary behavior), and GWG using a separate linear regression model for each outcome. Potential confounders were identified a priori from the research literature and causal diagrams. 34 Our first model included main effects for acculturation and months postpartum at study entry only. Our second model adjusted for the main effects of months postpartum at study entry, maternal age at study entry, breastfeeding status, education level, parity, and total energy intake (with exception of energy intake model).
To examine the relation between acculturation and PPWR, three separate linear regression models were estimated. Model 1 assessed the association between acculturation and PPWR adjusting only for months postpartum at study entry. Model 2 included main effects for months postpartum at study entry, maternal age at study entry, education, breastfeeding, and parity. Model 3 included variables from model 2 in addition to main effects for prepregnancy BMI as well as the diet and physical activity variables that were significantly associated with acculturation. A fourth model (Model 4) was examined to assess the additional influence of GWG. We also tested nativity as a modifier of the association using the F-test (p < 0.10). All analyses were conducted using SAS version 9.4 (Cary, NC).
Results
Characteristics of the study population
Table 1 shows the baseline characteristics of the study population by level of acculturation. Seventy-six percent of women had acculturation scores less than or equal to 3 (lower acculturation), whereas 24% had scores greater than 3 (higher acculturation). Compared with lower acculturation, women with higher acculturation were slightly younger and more likely to have lived in theU.S. longer (p < 0.05). Additionally, women with higher acculturation levels were more likely to have a high school degree or more and be U.S.-born, and were less likely to breastfeed or have more than one previous birth than women with lower acculturation levels (p < 0.05).
p < 0.05.
p < 0.01.
p < 0.001.
Acculturation in relation to diet, physical activity, and pregnancy-related weight variables
We further assessed differences between dietary intake, physical activity, and pregnancy-related weight by acculturation (Table 2). Women with higher acculturation scores had lower fruit and vegetable consumption and lower HEI scores than women with lower acculturation scores. In addition, higher acculturated women had lower levels of physical activity than women with lower acculturated women (p < 0.05). GWG and PPWR were moderately higher among more acculturated women than less acculturated (p < 0.10).
p-values based on ANOVA.
HEi, Healthy Eating Index; MVPA, moderate-to-vigorous physical activity.
Next, linear regression models were conducted to examine the extent to which acculturation was related to dietary intake and physical activity adjusting for potential confounding factors (Table 3). After adjustment for months postpartum, age at study entry, breastfeeding, education, parity, and total energy intake, higher acculturation was independently and inversely associated with HEI-2010 score (β: −1.99, 95% CI: −3.11 to −0.86, p < 0.01; Model 2) and light physical activity (β: −13.51, 95% CI: −21.88 to −5.14, p < 0.01; Model 2). A positive association was found between acculturation and total sedentary time (β: 15.43, 95% CI: 2.71–28.15, p = 0.02). Acculturation was not associated with total energy intake or total MVPA.
Model 1 adjusts for month's postpartum at study entry.
Model 2 adjusts for month's postpartum, age at study entry, breastfeeding, education, parity, and total energy intake (excluding total energy intake model).
Acculturation in relation to PPWR
Last, we examined the association between acculturation and PPWR (Figure 1). After adjustment for months postpartum at study entry, acculturation was positively associated with PPWR in that for every 1-unit increase in acculturation score, PPWR increased by 0.76 kg (95% CI: 0.22–1.31, p < 0.01; Model 1). This association was slightly attenuated after additional adjustment for maternal age at study entry, education, breastfeeding, and parity (β: 0.58, 95% CI: −0.03 to 1.18, p = 0.06; Model 2). In the Model 3, which included HEI-2010 score, total minutes of sedentary time, and prepregnancy BMI, in addition to variables included in model 2, PPWR increased, on average, by 0.80 kg (95% CI: 0.21–1.39) for every 1-unit increase in acculturation score (p < 0.01). As expected, we found a statistically significant correlation between GWG and PPWR (ρ = 0.55, p ≤ 0.0001). The additional adjustment for GWG (Model 4) resulted in an attenuation of our results, which were no longer statistically significant (β: 0.41, 95% CI: −0.11 to 0.92, p = 0.12). We did not find evidence that nativity modified the association between acculturation and PPWR based on our test of modification.
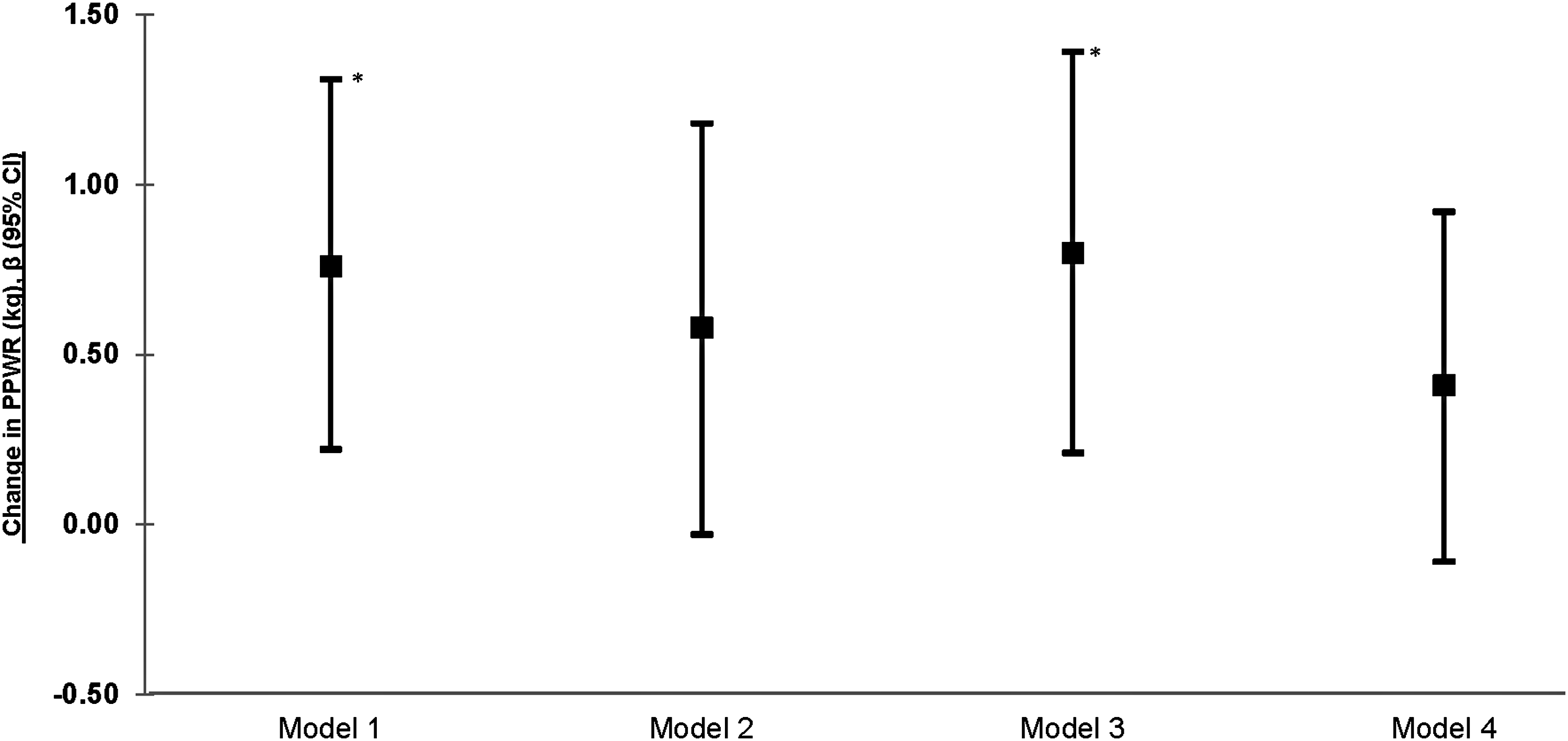
Associations of acculturation with postpartum weight retention. Model 1 adjusts for months postpartum at study entry. Model 2 adjusts for postpartum months at study entry, age at study entry, education level, breastfeeding, and parity. Model 3 adjusts for postpartum months at study entry, age at study entry, breastfeeding, parity, HEI2010 score, total minutes of sedentary activity, and prepregnancy BMI. Model 4 adjusts for postpartum months at study entry, age at study entry, breastfeeding, parity, HEI2010 score, total minutes of sedentary activity, prepregnancy BMI, and gestational weight gain. *p < 0.05.
Discussion
Among a sample of low-income Hispanic women, acculturation was associated with lower healthy-eating scores, lower levels of physical activity, and higher minutes of sedentary time. We also found a positive association between acculturation and PPWR. Specifically, PPWR increased, on average, by 0.80 kg for every 1-unit increase in acculturation score.
Our study adds to the limited body of research examining the association between acculturation and PPWR. Our findings are in contrast to a prior retrospective study, in which no association was found between language preference, a proxy measure of acculturation, and PPWR after adjusting for baseline BMI, age, and smoking status. 20 It is possible that language preference as a proxy measure has limited utility in capturing the complex process of acculturation by which immigrant populations adapt to and integrate into U.S. culture and society. Our study used the ARMSA-II scale to capture the multidimensionality of acculturation. The difference in assessment of acculturation might contribute to the conflicting results.
Our findings that women with higher acculturation had higher PPWR is similar to studies of weight gain during pregnancy. 22,35,36 Hispanic women residing in a U.S.–Mexico border county, a measure of lower acculturation, had a lower risk of excess GWG than women residing in a nonborder county. 36 Hispanic women born in the U.S., a commonly used measure of acculturation, gained more weight during pregnancy than women born outside the U.S. 22,35 A recent study among Puerto Rican women in Massachusetts measured acculturation using the Psychological Acculturation Scale and measures of generation in the U.S., place of birth, and language preference. 22 They found that women with grandparents and at least one parent born in Puerto Rico or the Dominican Republic gained, on average, 2.2 kg and 0.9 kg, respectively, more over the course of pregnancy than women who were born in Puerto Rico or the Dominican Republic; however, no association was found using other acculturation measures. It is important to note that these studies were conducted in diverse Hispanic populations (e.g., Dominican Republican, Puerto Rican, Honduran), whereas our findings are from predominately Mexican American women who have distinct cultural practices. Despite these differences, our findings are consistent.
We also observed inverse associations of acculturation with diet and physical activity behaviors. Higher acculturation was associated with lower diet quality, as measured by the HEI-2010. Similar findings were reported previously in a comprehensive systematic review, which found that Hispanics with higher acculturation consumed more fast food, snacks, sugars, and sugar-sweetened beverages and less fruit and beans than those who were less acculturated. 37 While we did not find an association between acculturation and levels of MVPA, statistically significant associations with light physical activity and sedentary time were observed. Higher levels of acculturation was associated with fewer minutes of light physical activity, which is in contrast to the widespread literature showing a positive relationship between acculturation and physical activity. 19 Moreover, higher acculturation was also associated with increased minutes of sedentary time. These findings provide evidence of the U.S. obesogenic environment's potential impact on unhealthy lifestyle behaviors among low-income Hispanic women.
PPWR and GWG were highly correlated in our study and the inclusion of GWG removed associations. Although previous studies have shown that PPWR is direct of GWG, some women gain weight during the postpartum year and this may be most likely among women of Hispanic ethnicity. 38 Prospective studies are needed to examine these relationships in minority populations, particularly Hispanic women.
Our study had several strengths. First, our study used a validated, multidimensional acculturation scale that accounts for the complex process by which individuals assimilate to U.S. culture, an improvement over previous studies that have used single proxy measures (e.g., language preference, nativity, generation). Second, physical activity was objectively measured using accelerometer data, which reduces potential recall bias. Third, maternal diet was assessed using dietary recalls, which are considered the gold standard in nutrition research. Fourth, postpartum weight was measured and collected at participating WIC clinics using a standardized protocol.
A limitation of our study was the cross-sectional design with retrospective report of GWG, which limits our ability to infer any causal effects. To address this limitation, we examined the robustness of our results after further adjusting for GWG and the effect estimate was attenuated and no longer statistically significant. Future studies utilizing follow-up data from FitMoms/Mamás Activas RCT will be able to better characterize the mediating effect of GWG on the acculturation–PPWR association. In addition, our study population included low-income Hispanic women, which likely limits the generalizability of our findings to postpartum Hispanic women from other socioeconomic groups.
Conclusions
To our knowledge, this was the first study among Hispanic women primarily of Mexican descent to examine the association between acculturation and PPWR using a comprehensive measure of acculturation. Our study showed that greater acculturation was associated with poorer diet quality, lower physical activity levels, and higher GWG and PPWR. Additional research is needed to replicate these findings in other Hispanic cohorts and to identify optimal methods to prevent acculturation-related adoption of unhealthy eating, physical activity, and weight control behaviors in Hispanic women at high risk of obesity-related comorbidities.
Footnotes
Acknowledgments
This study was funded by the National Institute of Diabetes and Digestive Kidney Diseases (KD087889) and the National Cancer Institute's Cancer Health Disparities Training Program (T32CA128582). The participation of the 12 WIC programs (six in Santa Barbara County, four in San Luis Obispo County, and two in Ventura County) is greatly appreciated.
Author Disclosure Statement
No competing financial interests exist.