
Abstract
Background:
Flibanserin, a 5-HT1A agonist and 5-HT2A antagonist, is indicated for the treatment of acquired, generalized hypoactive sexual desire disorder (HSDD) in premenopausal women. This post hoc analysis evaluated the effect of flibanserin treatment on body weight in premenopausal and postmenopausal women with HSDD.
Materials and Methods:
This analysis included three 24-week, double-blind, placebo-controlled studies of flibanserin 100 mg each bedtime (qhs) in premenopausal women, a similarly designed study in postmenopausal women, and a 52-week, open-label extension study in premenopausal women.
Results:
In a pooled analysis of premenopausal women, mean baseline body mass index (BMI) was 27.0 kg/m2 in the flibanserin group (n = 1227) and 26.8 kg/m2 in the placebo group (n = 1238). Among patients who completed 24 weeks of treatment, least squares (LS) mean weight change was −1.4 kg in the flibanserin group (n = 1010) and −0.1 kg in the placebo group (n = 1066; p < 0.0001). Weight loss ≥5% from baseline was reported in 21.0% of patients who received flibanserin and 7.8% of patients who received placebo; weight loss ≥10% was reported in 3.8% and 2.0% of patients, respectively. In postmenopausal women, mean baseline BMI was 27.7 kg/m2 in the flibanserin group (n = 467) and 27.3 kg/m2 in the placebo group (n = 480). LS mean weight change at week 24 was −1.8 kg in the flibanserin group (n = 385) and −0.1 kg in the placebo group (n = 425; p < 0.0001), with weight loss ≥5% reported in 24.7% and 7.3% of patients, respectively, and weight loss ≥10% reported in 5.2% and 1.7%, respectively. In HSDD patients with >12 months (n = 880) and >18 months (n = 637) of exposure to flibanserin, mean weight change was −1.0 and −1.2 kg, respectively; 25.4% and 26.9% of patients, respectively, experienced weight loss ≥5% from baseline, and 7.8% and 8.4%, respectively, experienced weight loss ≥10%.
Conclusions:
Women treated with flibanserin for HSDD may experience weight loss.
Introduction
F
By modulating these neurotransmitters, flibanserin is hypothesized to restore balance to the activity of excitatory and inhibitory influences on the regulation of a healthy sexual response. 7,8 The efficacy and safety of flibanserin in the treatment of HSDD have been demonstrated in randomized clinical trials of premenopausal and postmenopausal women 9 –13 ; however, flibanserin is not approved by the FDA for use in postmenopausal women.
Serotonin neurons play a complex role in the regulation of weight and metabolism, and pharmacologic agents with serotonin-related activity have been shown to increase or decrease body weight. 14 –19 Some serotonergic medications (e.g., certain selective serotonin reuptake inhibitors [SSRIs]) are associated with weight gain. 20,21 However, the selective 5-HT2C agonist lorcaserin is an FDA-approved weight-loss treatment for patients who are obese (body mass index [BMI] ≥30 kg/m2) or overweight (BMI ≥27 kg/m2 in the presence of ≥1 weight-related comorbid condition, such as hypertension or type 2 diabetes). 22 The receptor binding profile of flibanserin suggests that it may have an impact on body weight as well.
Data collected in the clinical development program for flibanserin were utilized to retrospectively investigate the effect of flibanserin treatment on body weight in women with HSDD. Analyses included change in body weight associated with flibanserin in premenopausal women (pooled data from three randomized, placebo-controlled, 24-week trials 9 –11 ) and postmenopausal women (in a randomized, placebo-controlled, 24-week study 13 ), and during long-term flibanserin use (in a 52-week, open-label, extension study 23 ).
Materials and Methods
Study design and participants
This retrospective analysis included data from five studies from the flibanserin clinical development program in HSDD (Table 1). 9 –11,13,23 Study conduct was in compliance with the principles of the Declaration of Helsinki (1996) in accordance with the International Conference on Harmonisation Good Clinical Practice guidelines. All study protocols were approved by an institutional review board or independent ethics committee, and all participants provided written informed consent before the initiation of study procedures.
Analyses of the placebo-controlled studies excluded patients who received flibanserin at doses other than 100 mg qhs.
bid, twice daily; DB, double-blind; DSM-IV-TR, Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition, Text Revision; HSDD, hypoactive sexual desire disorder; OLE, open-label extension; PBO, placebo-controlled; qhs, each bedtime; R, randomized.
Three patient populations were included in this analysis: (1) premenopausal women ≥18 years old who were diagnosed with HSDD and enrolled in one of three randomized, double-blind, placebo-controlled trials that evaluated the safety and efficacy of flibanserin (study names: VIOLET, DAISY, BEGONIA)
9
–11
; (2) naturally postmenopausal women of any age who were diagnosed with HSDD and enrolled in a randomized, double-blind, placebo-controlled trial evaluating the safety and efficacy of flibanserin (SNOWDROP)
13
; and (3) premenopausal women ≥18 years old who were diagnosed with HSDD and had participated in a randomized placebo-controlled trial (VIOLET, DAISY, DAHLIA),
9,10
a randomized withdrawal study (ROSE),
12
or a pharmacokinetic study of flibanserin and were subsequently enrolled in a 52-week, open-label extension study (SUNFLOWER).
23
The inclusion criteria for all studies in this analysis required that participants were diagnosed with generalized acquired HSDD of ≥24 weeks' duration (or ≥6 months' duration for the SNOWDROP study) according to the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition, Text Revision (DSM-IV-TR) criteria.
Key exclusion criteria included other sexual dysfunctions; major depressive disorder within the previous 6 months; history of suicidal ideation or behavior; pelvic inflammatory disease, urinary tract or vaginal infection/vaginitis, cervicitis, interstitial cystitis, vulvodynia, or significant vaginal atrophy; current pregnancy or pregnancy within the last month (SUNFLOWER 23 study) or last 6 months (VIOLET, 9 DAISY, 10 and BEGONIA studies); a history of cancer within the last 10 years; or blood abnormalities.
Use of certain medications was prohibited, including sex hormones (except for hormonal contraceptives in premenopausal women and systemic hormone therapy in postmenopausal women), dopamine agonists, benzodiazepines, prescription hypnotics, antidepressants, antipsychotics, mood stabilizers, antiepileptics, St. John's wort, metoclopramide, or chronically used narcotics. 11,13,23 None of the studies in this analysis excluded patients on the basis of weight or BMI.
Patients received double-blind flibanserin or placebo in the 24-week randomized controlled trials and open-label flibanserin in the 52-week extension study. To obtain information about weight change associated with the recommended dose of flibanserin (100 mg each bedtime [qhs]), analyses of the placebo-controlled trials included only those patients treated with flibanserin 100 mg qhs or placebo. The long-term, open-label study enrolled patients from a variety of flibanserin dosing regimens (and some patients previously on placebo). All patients received flibanserin 50 mg qhs for 4 weeks, with flexible dosing thereafter to optimize efficacy and tolerability; permitted doses were 50 or 100 mg qhs, or 25 or 50 mg twice per day.
None of the studies in this analysis was designed to evaluate weight loss as a clinical benefit of flibanserin treatment; body weight was measured to assess weight loss and weight gain as potential adverse effects.
Statistical analyses
The analysis population for the 24-week placebo-controlled trials consisted of patients who were randomly assigned to treatment, received at least one dose of study medication, and had at least one assessment of body weight. For the three 24-week studies of premenopausal women, patient-level data were pooled by treatment group (flibanserin 100 mg qhs vs. placebo) for assessments of body weight at baseline, and weeks 8, 16, and 24.
In the premenopausal and postmenopausal patient populations, least-squares (LS) mean change in body weight from baseline to week 24 was compared for flibanserin versus placebo using analysis of covariance (ANCOVA) models with treatment group as a factor and baseline body weight as a covariate. In the premenopausal patient population, additional ANCOVA models were used to explore the effect of potential confounding variables (i.e., use of SSRIs or serotonin norepinephrine reuptake inhibitors [SNRIs], smoking status, baseline BMI level [≤25 or >25 kg/m2], hormonal contraceptive use, and responder status on HSDD efficacy measures) on weight change.
In each model, except that for BMI level, the variable of interest and treatment group were used as factors with baseline body weight as a covariate; because BMI and weight are highly correlated, the model for BMI included baseline BMI (rather than baseline weight) as the covariate.
The analysis population for ANCOVAs of HSDD responder status consisted of patients in the overall analysis population who had at least one postbaseline efficacy assessment. To identify patients with a clinically meaningful benefit in HSDD symptoms, change from baseline to endpoint on measures of sexual functioning (i.e., number of satisfying sexual events [SSE], the Female Sexual Functioning Index-desire domain [FSFI-D], and the Female Sexual Distress Scale-Revised-desire item [FSDS-R13]) was anchored to responses on the Patient Global Impression of Improvement (PGI-I) scale. For each measure of sexual functioning, a responder was defined as a patient with baseline to endpoint score change greater than the corresponding minimal response threshold (i.e., score of 3 [minimally improved]) on the PGI-I.
In the open-label extension study, change in body weight was assessed for patients who had >12 months (365 days) and >18 months (547 days) of exposure to flibanserin.
Results
Patients
Demographic and clinical characteristics of premenopausal and postmenopausal women treated with flibanserin 100 mg qhs or placebo in a 24-week randomized controlled trial are shown in Table 2. In the pooled analysis of premenopausal women, 1210 patients in the flibanserin group and 1218 patients in the placebo group had at least 1 assessment of body weight and were included in this analysis. In the study of postmenopausal women, 467 flibanserin-treated patients and 479 patients receiving placebo had at least 1 assessment of body weight and were included in this analysis. Within the premenopausal and postmenopausal patient populations, characteristics were similar in the flibanserin and placebo groups. In the long-term, open-label extension study, 880 patients received flibanserin for >12 months and 637 patients received flibanserin for >18 months.
Three studies (VIOLET, DAISY, and BEGONIA) pooled.
n = 479.
n = 477.
Protocol violation.
BMI, body mass index; SD, standard deviation; SNRI, serotonin-norepinephrine reuptake inhibitors; SSRI, selective serotonin reuptake inhibitor.
Change in weight after 24 weeks of treatment with flibanserin
At week 24, LS mean change (standard error) in weight was −1.4 (0.1) kg in the flibanserin group and −0.1 (0.1) kg in the placebo group in premenopausal women (p < 0.0001) and −1.8 (0.2) kg in the flibanserin group and −0.1 (0.2) kg in the placebo group in postmenopausal women (p < 0.0001) (Fig. 1). Weight loss differed significantly by BMI in the premenopausal patient population; greater LS mean weight loss was observed in women with higher (>25 kg/m2) versus lower baseline BMI (p < 0.01) (Table 3).
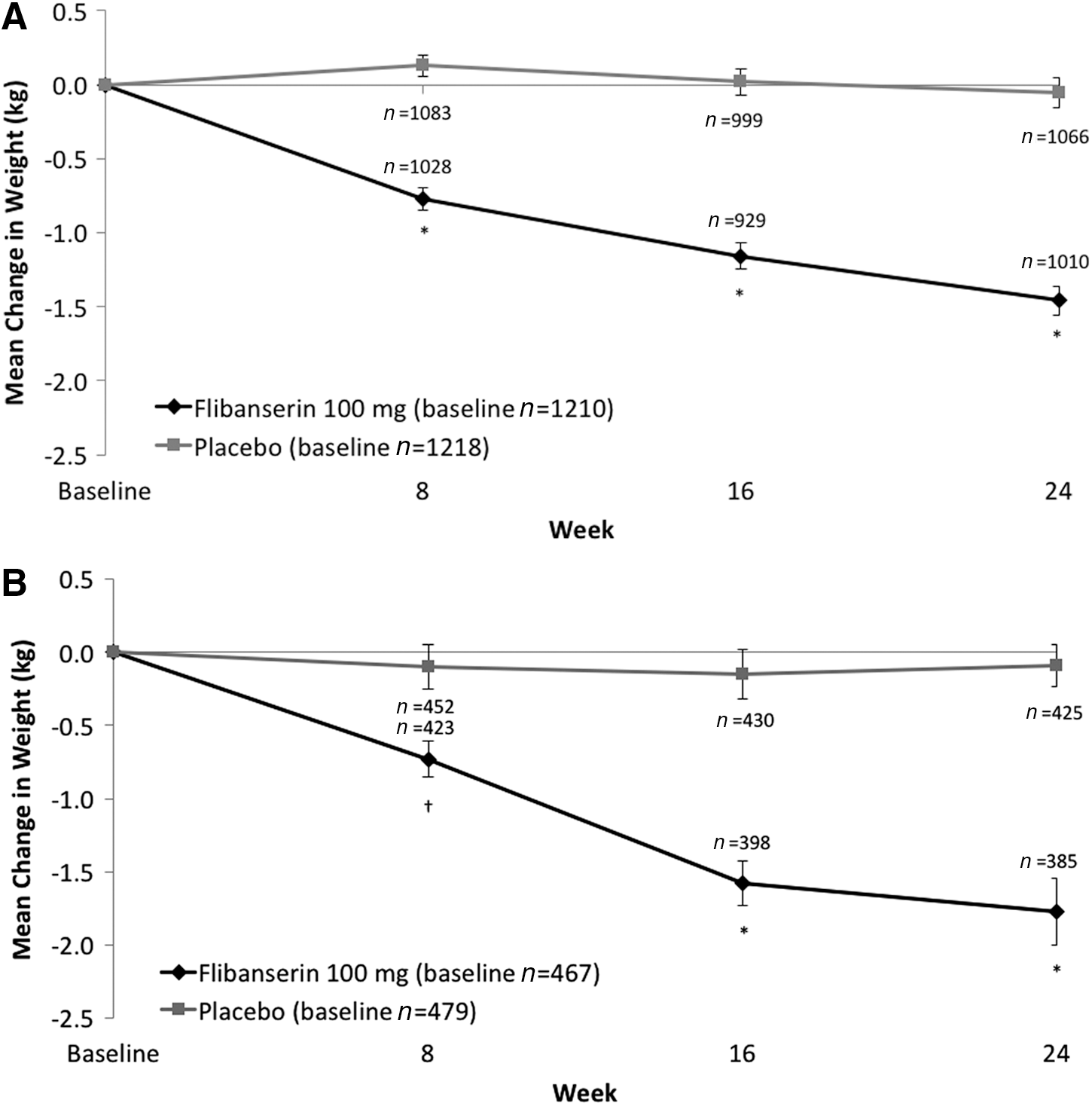
Mean change from baseline weight (kg) after 8, 16, and 24 weeks of treatment with flibanserin 100 mg qhs or placebo in
p Value for the contrast between the two levels of each variable, after accounting for the effects of baseline body weight (or baseline BMI in the model for BMI level) and treatment group.
Protocol violation.
FSDS-R13, Female Sexual Distress Scale-Revised-desire item; FSFI-D, Female Sexual Function Index-desire domain; LS, least squares; SE, standard error; SSE, satisfying sexual events.
None of the other baseline factors investigated (i.e., SSRI/SNRI use, smoking status, and hormonal contraceptive use) had a significant effect on weight change, after accounting for the effects of baseline body weight and treatment group. Similarly, there was no significant difference between treatment responders and nonresponders (as determined by change on HSDD efficacy measures [number of SSE, FSFI-D score, FSDS-R13 score]) in change from baseline body weight.
In each analysis, there was a statistically significant association of weight change at week 24 with baseline body weight and treatment group such that higher baseline body weight and treatment with flibanserin (vs. placebo) were associated with greater weight loss.
At the end of 24 weeks, 21.0% of premenopausal women receiving flibanserin had lost ≥5% of their baseline body weight compared with 7.8% of premenopausal women receiving placebo (p < 0.0001); 3.8% and 2.0% of patients, respectively, experienced ≥10% weight loss (Fig. 2). Similarly, 24.7% of postmenopausal women receiving flibanserin had lost ≥5% of their baseline body weight at week 24, compared with 7.3% of postmenopausal women receiving placebo (p < 0.0001); 5.2% and 1.7% of patients, respectively, experienced ≥10% weight loss. At week 24, weight gain ≥7% (the FDA definition of significant weight gain 24 ) was observed in 1.8% and 3.4% of premenopausal women in the flibanserin and placebo groups, respectively, and in 2.1% and 2.8% of postmenopausal women, respectively.
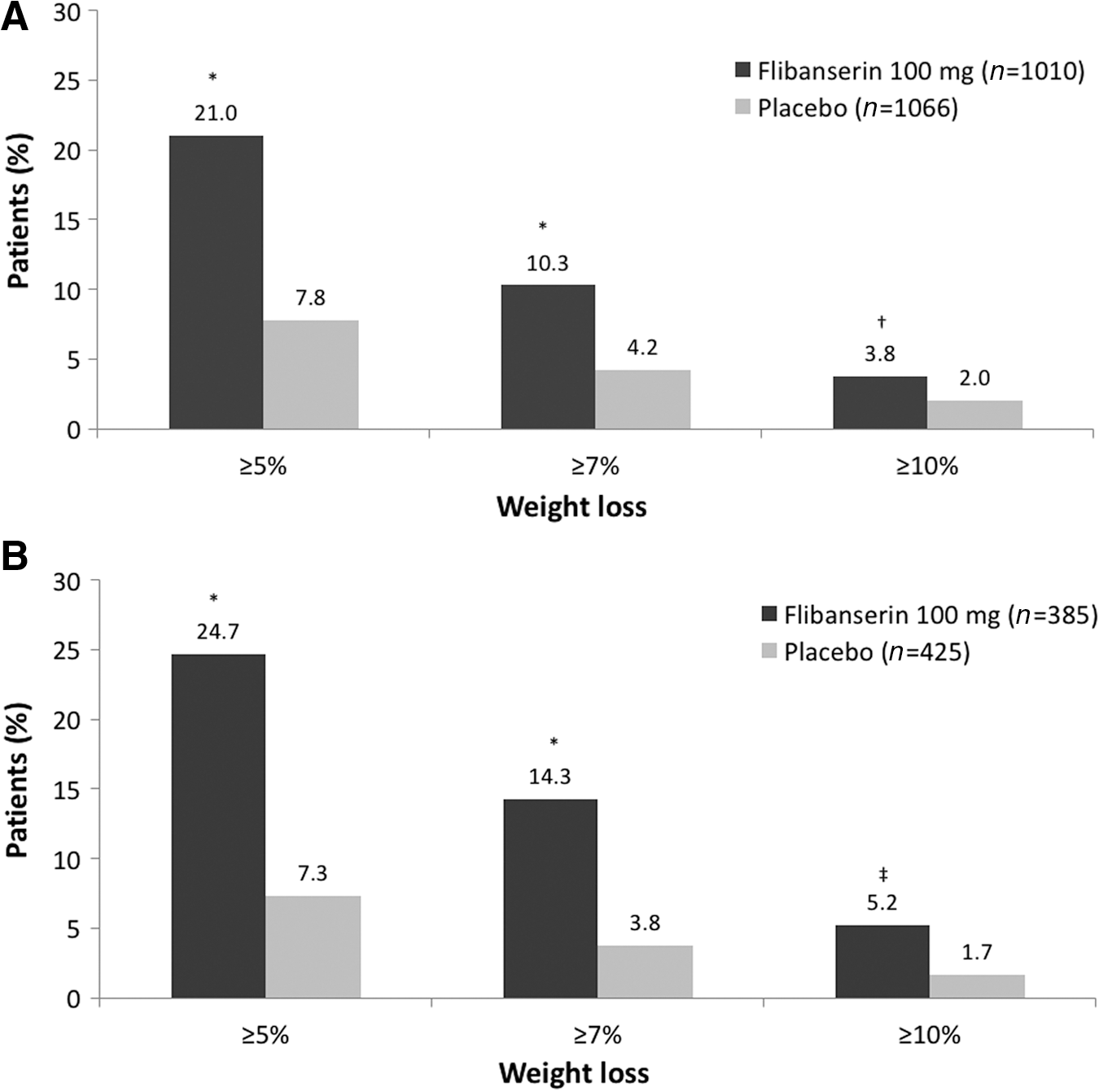
Proportion of patients who lost 5% or more, 7% or more, and 10% or more of their baseline body weight after 24 weeks of treatment with flibanserin 100 mg qhs or placebo in
To evaluate a possible dose–response effect, an analysis of once-daily flibanserin at a dose lower than currently recommended included 295 premenopausal women with HSDD who received flibanserin 50 mg qhs (in the VIOLET study). 9 For flibanserin 50 mg qhs, LS mean weight change at week 24 was −0.6 kg (compared with −0.1 kg for placebo and −1.4 kg for flibanserin 100 mg); weight loss of ≥5% and ≥10% was experienced by 8.9% and 1.9% of women, respectively (compared with 7.8% and 2.0%, respectively, for placebo and 21.0% and 3.8%, respectively, for flibanserin 100 mg).
Nausea, a common adverse event with flibanserin, was assessed as a possible contributor to weight loss. However, the incidence of nausea in premenopausal women with HSDD who received flibanserin 100 mg in the 24-week randomized, placebo-controlled trials was somewhat higher (7.1%) in women with weight loss <5% compared with 5.8% in women with weight loss ≥5%. The incidence of nausea was similar in postmenopausal women with weight loss <5% versus weight loss ≥5% (incidence of nausea 5.3% and 5.6%, respectively).
Change in weight after longer term treatment with flibanserin
In addition, weight loss was observed after 12 and 18 months of treatment with flibanserin (Table 4). In premenopausal patients, mean (standard deviation) weight change from parent study baseline equaled −1.0 (6.1) kg in patients with flibanserin exposure >12 months and −1.2 (5.4) kg in patients with flibanserin exposure >18 months. Weight loss >5% from parent study baseline was observed in 25.4% of patients with >12 months of treatment with flibanserin and 26.9% of patients with >18 months of treatment; weight loss ≥10% was experienced by 7.8% and 8.4% of patients, respectively.
Results at baseline and final study visit include all patients with nonmissing data.
Discussion
In this retrospective analysis of clinical studies, flibanserin was associated with statistically significant weight loss compared with placebo in both premenopausal and postmenopausal women with HSDD who received 6 months of double-blind treatment. In addition, flibanserin-associated weight loss was comparable in both premenopausal and postmenopausal women. Also, there was no evidence of weight regain based on the assessment of patients treated with flibanserin for 18 months. Hormonal contraceptive use, SSRI/SNRI use, BMI level, and smoking status (assessed at baseline); nausea (assessed as an adverse event); and treatment responder status (based on clinically meaningful change in HSDD efficacy measures) did not demonstrate a significant effect on weight change.
The patients with HSDD who participated in these clinical trials of flibanserin were not selected for overweight or obesity, nor did they enter the studies with the goal of losing weight. In the patients with HSDD included in this analysis, baseline BMI ranged from underweight to obese, with rates of overweight (premenopausal women, 27.2%; postmenopausal women, 34.4%) and obesity (premenopausal women, 24.9%; postmenopausal women, 28.2%) somewhat lower than currently observed in the general population of adult women in the United States, 25 which may represent a healthy user type bias in these clinical trials. Nonetheless, comparing these findings with studies of FDA-approved weight-loss drugs may provide some context regarding the magnitude of weight loss observed.
In double-blind, placebo-controlled studies of FDA-approved weight-loss drugs (i.e., lorcaserin, naltrexone/bupropion, phentermine/topiramate, and liraglutide), patients received dietary and exercise counseling, in addition to medication. Mean weight loss in overweight/obese patients (70%–85% of whom were women) ranged from 5 to 10 kg for the active study medication and 1 to 3 kg for placebo after 52 to 56 weeks of treatment. 22,26 –31 Studies that reported mean weight change at interim time points showed similar weight loss at 24–28 weeks and at 52–56 weeks. 26,28,31
Between 40% and 70% of patients treated with FDA-approved weight-loss medications (and 16%–27% of patients receiving placebo) lost ≥5% of their baseline body weight at the typical month-12 study endpoint. 22,26 –31 In these studies of women with HSDD, mean baseline BMI (premenopausal women, 26.9 kg/m2; postmenopausal women, 27.5 kg/m2) was substantially lower than that in studies of weight-loss medications (35.8–38.3 kg/m2); in addition, HSDD patients were generally not attempting to lose weight and did not receive the ancillary therapies provided in weight-loss studies (e.g., nutritional counseling, exercise counseling). 26 –31
The lower BMI in these studies, as well as the lack of patient intent to lose weight, makes the weight loss in the flibanserin-treated patients all the more intriguing. Mean weight loss was 1.5–1.8 kg after 6 months of treatment with flibanserin and 1.0 kg after 12 months of treatment, with mean weight remaining essentially unchanged in patients who received placebo. Weight loss ≥5% from baseline was observed at month 6 in 21%–25% of patients receiving flibanserin and only 7%–8% of patients receiving placebo, and at month 12 in 25% of flibanserin-treated patients. It is possible that weight loss observed in the flibanserin studies was limited by a floor effect, since baseline weight was lower in these studies compared with clinical trials of weight-loss medications.
The mechanism(s) of action by which flibanserin produces weight loss are currently unknown. The receptor binding affinity of flibanserin is highest for 5-HT1A receptors (as an agonist) and 5-HT2A receptors (as an antagonist). 6 Both 5-HT1A agonist activity and 5-HT2A antagonist activity result in the inhibition of glutamate neurons, thereby reducing serotonin release in the prefrontal cortex. 6
The complex role of serotonin in mammalian energy balance has not been completely elucidated at this time. 32 Based on evidence from numerous studies of the serotonin system, it is generally understood that enhanced serotonergic neurotransmission is associated with suppression of food intake and reduction in body weight. 19,26,32 However, mirtazapine, an atypical antidepressant with agonist effects at the 5-HT1A receptor and antagonist effects at the 5-HT2A receptor (similar to flibanserin), is generally known to cause weight gain. 33,34 Furthermore, flibanserin is a minor 5-HT2C receptor antagonist, 1 yet the 5-HT2C receptor agonist lorcaserin has been approved as a weight-loss drug. 22 Thus, the serotonin-related activity of flibanserin does not appear to explain the observed weight loss in this analysis of patients treated with flibanserin. 32
Either flibanserin affects body weight via a serotonin-based process that is as yet unknown or weight loss associated with flibanserin can be accounted for by non–serotonin-related mechanisms (e.g., enhanced cortical norepinephrine release). It is interesting to note that no significant association was observed in this analysis for weight loss and treatment response (defined as clinically meaningful change on HSDD efficacy measures), suggesting that the flibanserin mechanism of action for weight loss may differ from that for improved sexual function.
This analysis has several limitations. The studies included in this analysis were designed to evaluate the efficacy and safety of flibanserin for the treatment of women with HSDD. This analysis of change in body weight is, therefore, post hoc and exploratory in nature. There was no systematic attempt to collect information about the use of medications or supplements known to affect body weight or participation in programs intended to promote weight loss, nor was dietary or exercise counseling provided. Because this analysis included only observed cases, weight change was not assessed in patients who discontinued early from the underlying studies. Further investigation is needed to more rigorously evaluate changes in body weight associated with flibanserin treatment.
Conclusions
This retrospective analysis showed that treatment with flibanserin 100 mg qhs in women with HSDD was associated with statistically significant weight loss compared with placebo in both premenopausal and postmenopausal patients. Weight loss without apparent weight regain was also observed during longer term, open-label flibanserin treatment of up to 18 months. In contrast to more typical serotonergic antidepressants, weight gain does not appear to be a clinical concern with flibanserin. Women treated with flibanserin for HSDD may experience weight loss.
Footnotes
Acknowledgments
Technical editorial and medical writing assistance was provided under the direction of the authors by Nancy Holland, PhD, Synchrony Medical Communications, LLC (West Chester, PA). Funding for this support was provided by Valeant Pharmaceuticals North America, LLC (Bridgewater, NJ).
Author Disclosure Statement
Dr. Kornstein reports receiving research support from Allergan, Palatin Technologies, Pfizer, and Takeda Pharmaceutical Co., Ltd.; and serving as a consultant to or on the advisory board for Allergan, Forest, Eli Lilly and Company, Pfizer, Takeda Pharmaceutical Co., Ltd., Palatin Technologies, Shire, and Sunovion Pharmaceuticals, Inc. Dr. Simon reports receiving grant/research support from AbbVie, Inc., Allergan, plc, Agile Therapeutics, Bayer Healthcare, LLC, New England Research Institute, Inc., ObsEva SA, Palatin Technologies, Symbio Research, Inc., and TherapeuticsMD; serving as a consultant to or on the advisory board for AbbVie, Inc., Allergan, plc, AMAG Pharmaceuticals, Inc., Amgen, Inc., Ascend Therapeutics, Azure Biotech, Inc., Bayer Healthcare Pharmaceuticals Inc., CEEK Enterprises, LLC, Covance Inc., Millendo Therapeutics, Inc., Mitsubishi Tanabe Pharma Development America, Inc., ObsEva SA, Radius Health, Inc., Sanofi S.A., Sebela Pharmaceuticals, Inc., Sermonix Pharmaceuticals, Inc., Shionogi, Inc., Symbiotec Pharmalab, TherapeuticsMD, and Valeant Pharmaceuticals North America, LLC; serving on the speakers' bureau for Duchesnay USA, Novo Nordisk, Shionogi, Inc., and Valeant Pharmaceuticals (Laval, Canada); and being a stock shareholder of Sermonix Pharmaceuticals. Dr. Apfel reports serving as a consultant to Valeant Pharmaceuticals (Laval, Canada). Drs. Yuan, Barbour, and Kissling are employees of Valeant Pharmaceuticals North America, LLC (Bridgewater, NJ).
Funding
This study was supported by Boehringer Ingelheim. Boehringer Ingelheim was involved in study design, data collection, and data analysis. Boehringer Ingelheim had no involvement in interpretation of data, writing of the report, or the decision to submit the report for publication. Funding for technical editorial and medical writing assistance was provided by Valeant Pharmaceuticals. Valeant Pharmaceuticals was involved in interpretation of data and writing of the report.