
Abstract
Objectives:
We retrospectively evaluated the prognostic significance of dual-time point (DTP) 18F-FDG positron emission tomography/computed tomography (PET/CT) parameters compared with clinicopathological findings in premenopausal women with invasive ductal breast carcinoma (IDC).
Materials and Methods:
Sixty-six premenopausal women (mean age: 42.7 ± 5.6, range: 29.5–51.8 years) who had pathologically confirmed IDC were enrolled. The maximum standardized uptake value (SUVmax), metabolic tumor volume (MTV), and total lesion glycolysis (TLG) were measured and used to calculate percentage changes over the DTP time interval. We analyzed the prognostic significance of DTP PET/CT parameters, clinicopathological factors of pathologic tumor diameter (pTD), axillary lymph node status (ANS), nuclear grade, histologic grade, and immunohistochemistry findings using univariate and multivariate analyses.
Results:
Disease recurrence was observed in 22 patients. In univariate analysis, SUVmax > 7.39, MTV > 4.28, TLG > 52.38, %ΔSUVmax > 20.44, %ΔTLG > −13.86, pTD > 2.8 cm, positive ANS, estrogen receptor (ER) negativity, and triple negativity were associated with worse prognosis than those of opposite groups in recurrence-free survival (all p < 0.05). %ΔSUVmax (>20.44, p = 0.0042), TLG (>52.38, p = 0.0002), and ER negativity (p = 0.0003) were independent prognostic variables after multivariate analysis.
Conclusion:
Percentage changes in SUVmax using DTP PET/CT and TLG were significant independent prognostic factors of disease recurrence along with ER negativity in premenopausal women with IDC.
Introduction
B
Breast cancer evaluation using PET/CT is usually performed as a single-time point study ∼1 hour after intravenous 18F-FDG injection. Using this protocol, however, we found a somewhat variable clinical significance for PET/CT of 63%–96% sensitivity and 75%–100% specificity to discriminate malignant lesion. 14,15 This variability could be related to the heterogeneous invasiveness of tumor cells and the variable glucose metabolic activity of certain breast cancer types. These features can lead to false negatives. Previous studies demonstrated that FDG accumulation in tumor cells, which could reflect the retention index of radiopharmaceutical isotopes, continues to increase over time from an early to a delayed phase after intravenous administration. This finding may improve the diagnostic performance as well as the prognostic value in breast cancer. 16 –18
Identification of optimal variables to predict disease outcome is a great challenge in determining appropriate treatment strategies, especially in premenopausal women with breast cancer. We hypothesized that percentage changes in PET/CT parameters using dual-time point (DTP) imaging acquisition have significant prognostic value for predicting disease recurrence. Therefore, the purpose of the present study was to demonstrate the prognostic significance of metabolic parameters using DTP 18F-FDG PET/CT compared with well-established clinicopathological factors in premenopausal women with invasive ductal breast carcinoma (IDC).
Materials and Methods
Patients
We retrospectively reviewed clinical information from all patients who were newly diagnosed with IDC and underwent preoperative DTP 18F-FDG PET/CT between November 2010 and April 2014. We identified 262 eligible patients. Among these patients, we excluded patients with previous history of any other malignancy (n = 11), multifocal or multicentric breast cancer (n = 33), neoadjuvant chemotherapy or radiotherapy before PET/CT (n = 3), pathological tumor diameter (pTD) 2 cm or less (n = 74), or initial suspicion of distant metastasis (n = 2). Patients with bilateral breast cancers (n = 7), follow-up less than 6 months (n = 3), and postmenopausal patients (n = 63) were also excluded. In total, 66 women (mean age 42.7 ± 5.6 years; range, 29.9–51.8 years) were enrolled in the current study.
In 66 patients, IDC was pathologically confirmed after surgery (47 breast-conserving surgeries followed by subsequent radiotherapy, 16 modified radical mastectomies, and 3 skin-sparing mastectomies with or without axillary lymph node dissection). After surgery, patients were followed every 3–6 months in the first 2 years and then every year for regular examinations and imaging studies such as breast ultrasonography, mammography, bone scan, and chest X-ray. When recurrence was suspected, additional imaging modalities with or without histological confirmation were ordered at the corresponding physician's discretion. We identified disease recurrence through imaging studies or pathology biopsies.
This retrospective clinical review was approved by the Institutional Review Board of Ewha Womans University Hospital (blinded).
DTP 18F-FDG PET/CT
18F-FDG PET/CT was performed for initial breast cancer staging workup from skull base to proximal thigh in the supine position. Before PET/CT, all patients were required to fast for at least 6 hours to obtain a blood glucose level less than 140 mg/dL. Early-phase PET/CT imaging acquisition started 1 hour after 5.18 MBq/kg 18F-FDG intravenous administration using a Siemens Biograph mCT with 128-slice CT (Siemens Medical Solutions, Erlangen, Germany). The PET/CT scanner comprised a dedicated PET with full-ring bismuth germanate detector and multislice CT. First, total body low-dose CT was used for attenuation correction. Second, an emission scan of 5–7 bed positions with 2 minutes per bed position was obtained to acquire PET image parameters. PET images were reconstructed to 200 × 200 matrices and 3.4 × 3.4 mm pixel size with 3.0-mm slice thickness using CT data and a three-dimensional iterative algorithm. Integrated PET/CT images were interpreted by commercial software using a Syngo.via workstation (Siemens Medical Solutions, Erlangen, Germany). Two hours after radioisotope injection, delayed-phase imaging was performed only on the chest region, including bilateral breasts, in the same supine position as early-phase imaging. During the interval between imaging acquisitions, patients remained in a resting position on a bed to minimize FDG consumption by muscle.
Image analysis
DTP PET/CT images were interpreted by two experienced nuclear medicine physicians who were unaware of the clinicopathological information. Consensus was reached for each patient. Semiquantitative and volumetric parameters of PET/CT were analyzed using the automatic method in Syngo.via for delineating the three-dimensional volume of interest (VOI), with increased FDG uptake on PET/CT images obtained 1 hour after radiotracer injection.
VOIs were drawn to cover lesions that did not encase nonavid FDG lesions. The SUVmax, which is the highest FDG uptake value, was estimated. SUV was defined as the decay-corrected activity/tissue volume/injected dose/body weight. MTV and TLG were measured based on an automatic spherical-shaped delineation of VOI with an isocontour fixed threshold of SUV 2.5. Voxels with threshold-based automated VOIs were used to define MTV simultaneously in the axial, sagittal, and coronal images. TLG was calculated by multiplying MTV by the average SUV within selected VOIs of the primary tumor.
These semiquantitative parameters were analyzed at delayed phase by the same method. Percentage changes over time for early and delayed phases were calculated for SUVmax and TLG by subtracting early from delayed measurements and dividing by early measurements.
Clinicopathological characteristics
We analyzed clinicopathological characteristics, including age, pTD, axillary lymph node status (ANS), nuclear grade, and histological grade defined by the modified Bloom–Richardson scoring system. Immunohistochemistry was evaluated by an indirect immunoperoxidase process using antibodies against estrogen receptor (ER), progesterone receptor (PR), and Her-2. We determined the Allred score, a semiquantitative system for the percentage of cells positive for hormone receptors (scored from 0 to 5), and staining intensity (scored from 0 to 3) for each patient. ER and PR status was assessed as a combined total score from 0 to 8. A score of 0–2 was considered negative hormone status and 3–8 was considered positive. 19 Her-2 positivity was classified using the American Society of Clinical Oncology/College of American Pathologists guidelines, defined as higher intensity of cell membrane staining for at least 10% of cells. 20 Triple negativity (TN) was defined as negative for ER, PR, and Her-2.
Statistical analyses
All data are described as mean ± standard deviation. Recurrence-free survival (RFS) was defined as time from date of initial IDC diagnosis to date of the objective report, suggesting disease recurrence during follow-up. Receiver operating characteristic (ROC) curve analysis was used to assess optimal cutoff values of continuous variables such as age, pathologic tumor diameter, SUVmax, MTV, TLG, %ΔSUVmax, and %ΔTLG. In univariate analysis, the Kaplan–Meier method was performed using a log-rank test. After that prognostic factors with a p-value of less than 0.05 in univariate analysis were selected for multivariate analysis using Cox proportional hazards regression model to evaluate independent prognostic factors of RFS. To avoid collinearity in multivariate analysis, simple correlation analysis was performed between each semiquantitative parameter. A threshold of >0.7 for the correlation coefficient was considered to remove collinear variables. 21 All statistical analyses were performed using MedCalc software package (Ver. 96.5, MedCalc Software, Mariakerke, Belgium). A p-value less than 0.05 was considered statistically significant.
Results
Patient characteristics
For patient pathological stage, 61 (92.4%) had T2 and 5 (6.6%) had T3 (Table 1). Axillary lymph node metastases were observed in 37 (56.1%). The mean follow-up periods were 30.9 ± 14.0 months (range, 6.6–61.8 months). During this study, disease recurrence occurred in 22 patients with recurrence confirmed through tissue biopsy in 19 patients and the remaining 3 diagnosed through imaging studies. Of patients with recurrence, eight experienced axillary lymph node metastasis, four had locoregional breast recurrence, three had chest wall metastasis, three had bone metastasis, two had pulmonary metastasis, and two had liver metastasis.
ANS, axillary lymph node status; ER, estrogen receptor; PR, progesterone receptor; Her-2, human epidermal growth factor receptor 2; TN, triple negative.
Clinicopathological characteristics and RFS
The results of univariate analysis are listed in Table 2. Premenopausal patients with a pTD greater than 2.8 cm (p = 0.0010) or metastatic ANS (p = 0.0077) had poor RFS compared with those without. In premenopausal status, ER negativity (p = 0.0127) and TN (p = 0.0103) also showed significantly poor prognosis. Otherwise, age (p = 0.1184), nuclear grade (p = 0.1021), histologic grade (p = 0.2770), PR (p = 0.5459), and Her-2 status (p = 0.2631) did not show prognostic significance in univariate analysis.
p < 0.05.
pT, pathological tumor.
DTP PET/CT parameters and RFS
Cutoff values for continuous DTP parameters were determined by ROC curve analysis. The optimal cutoff values were SUVmax, 7.39 (p = 0.0206; 95% confidence interval [CI], 0.548–0.785; AUC [area under the ROC curve], 0.675); MTV, 4.28 (p = 0.0123; 95% CI, 0.567–0.800; AUC, 0.693); TLG, 52.38 (p = 0.0093; 95% CI, 0.576–0.807; AUC, 0.701); %ΔSUVmax, 20.44 (p = 0.0092; 95% CI, 0.564–0.798; AUC, 0.690); and %ΔTLG, −13.86 (p = 0.9209; 95% CI, 0.381–0.633; AUC, 0.507), in premenopausal women (Table 3).
AUC, Area under the receiver operating characteristic (ROC) curve; MTV, metabolic tumor volume; SUV, standardized uptake value; TLG, total lesion glycolysis.
Kaplan–Meier curves for RFS are shown in Figure 1. Using the cutoff values for PET/CT parameters, DTP parameters SUVmax (p = 0.0130), MTV (p = 0.0137), TLG (p = 0.0003), %ΔSUVmax (p = 0.0069), and %ΔTLG (p = 0.0463) were significant predictors of poor prognosis (Table 4). The RFS of the higher SUVmax, MTV, TLG, %ΔSUVmax, and %ΔTLG than cutoff values was significantly lower than those of opposite groups.
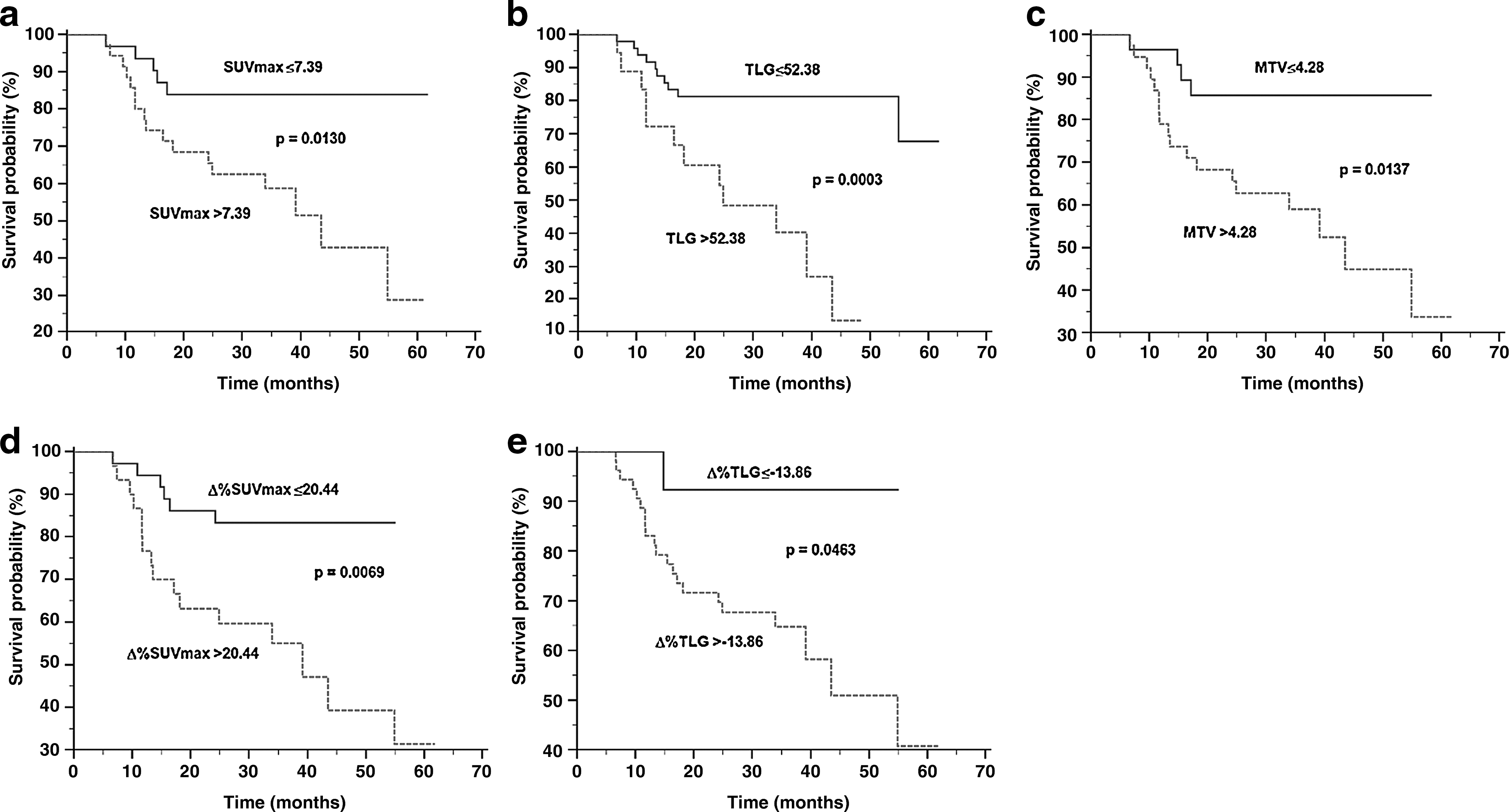
Kaplan–Meier curves of recurrence-free survival for optimal cutoffs of DTP PET/CT parameters.
p < 0.05.
Multivariate analysis
All significant prognostic factors assessed by univariate analysis were selected for multivariate analysis. The results of simple correlation test revealed significant collinearity between MTV and TLG (r = 0.9520; p < 0.0001). According to this result, TLG was chosen for further evaluation since its accuracy for predicting prognosis was greater than that of MTV (75.8% vs. 63.6%). After Cox proportional hazards regression model excluding MTV, ER negativity (p = 0.0003), TLG (p = 0.0002), and %ΔSUVmax (p = 0.0042) were significant independent prognostic factors (Table 5). Representative cases with different prognostic variables are demonstrated in Figures 2 and 3.
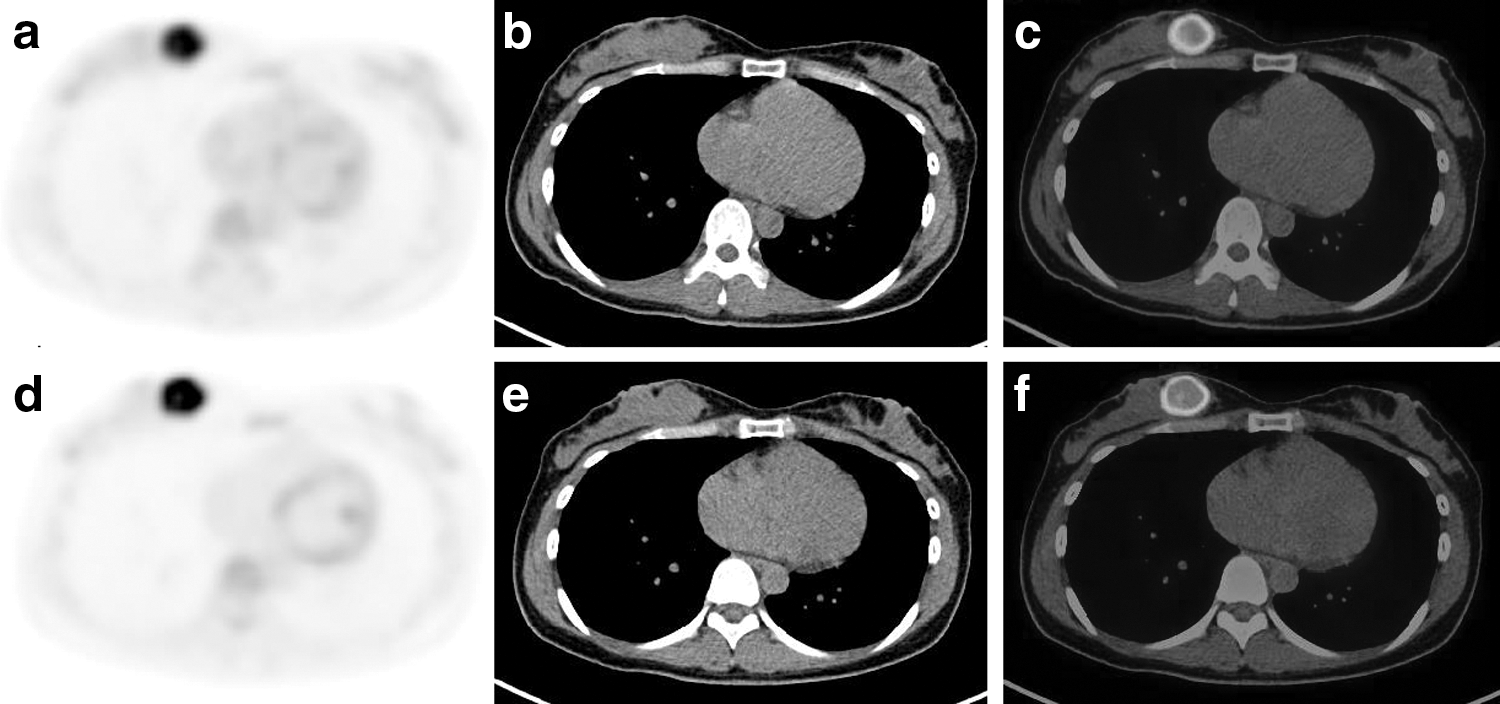
A 41-year-old premenopausal patient with invasive ductal breast cancer (%Δ SUVmax 53.07, TLG 119.33, negative ER).
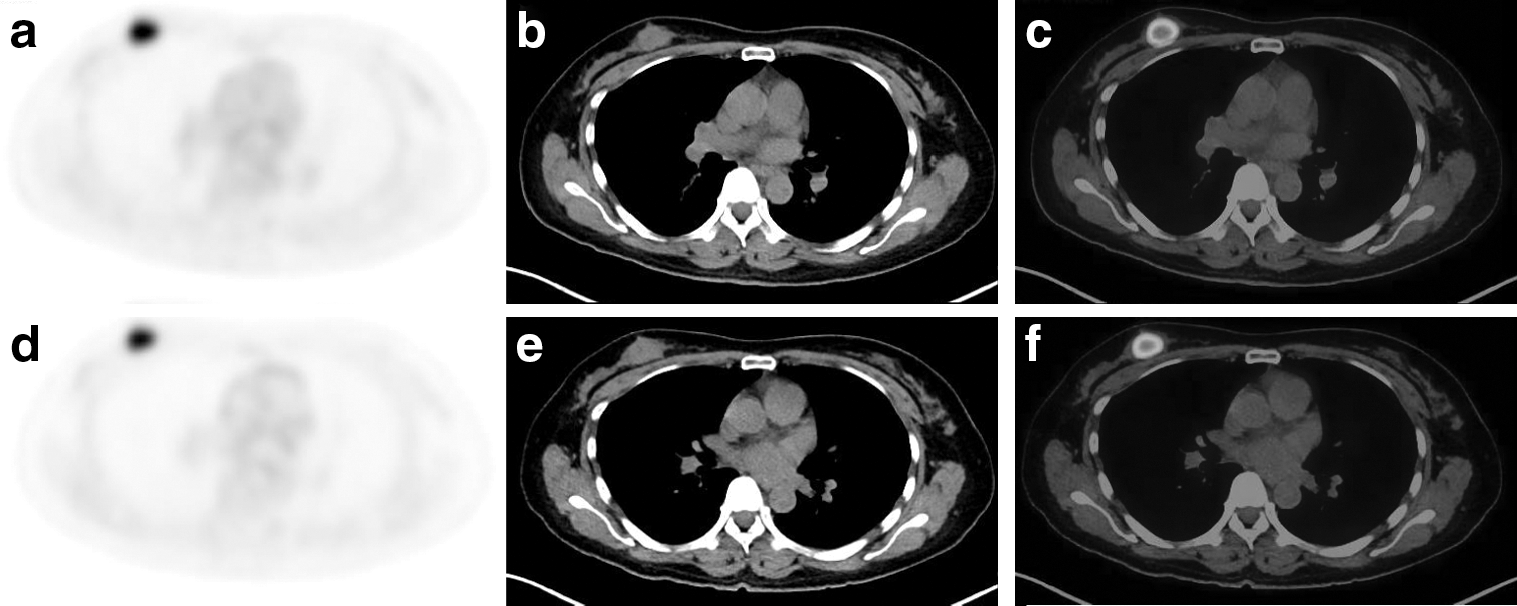
A 46-year-old premenopausal patient with invasive ductal breast cancer (%ΔSUVmax −9.98, TLG 39.02, positive ER).
Variables excluding MTV were entered stepwise into the multivariate regression model if p < 0.05 and were removed if p > 0.1.
p < 0.05.
HR, hazard ratio; CI, confidence interval.
Discussion
Several new concepts derived from 18F-FDG PET/CT have been used to improve diagnostic value and predictive effectiveness in oncology. One parameter is based on the metabolic tumor burden representing all tumoral metabolic activity. Another parameter is the percentage change in radiotracer uptake, which could reflect neoangiogenesis and blood vessel permeability. 9,22 For this reason, a number of PET/CT protocols have been proposed using a combination of the above characteristics of PET parameters simultaneously. Several publications have demonstrated that FDG uptake increases continuously in malignancies for a time after radioisotope administration. 23,24 Compared with single-time point image acquisition, DTPs can illustrate changes in glucose metabolism over time. We assumed that increasing radioisotope uptake would cause enhanced expression of hexokinase II and glucose transporter I activity in malignant cancer cells. This feature could represent the aggressiveness of cancer cells. Based on this assumption, more aggressive cancer cells could indicate a highly significant FDG enhancement on delayed PET/CT images. Conversely, less aggressive cancer cells could have more FDG clearance, depending on the time period.
We evaluated the prognostic ability of DTP parameters using 18F-FDG PET/CT in premenopausal women with IDC compared with well-known clinicopathological factors. Our study demonstrated that TLG as a volumetric parameter and %ΔSUVmax as percentage changes of PET/CT parameter were independent prognostic factors of RFS.
Although both MTV and TLG were identified as significant prognostic factors in current study, TLG had higher predictive value than MTV for RFS. We postulated that TLG, which was calculated by multiplying MTV by the average SUV of a corresponding target lesion, would be corrected by tumor metabolic activity and reflect both tumor volume and metabolic tumor cell glucose activity.
Our results are consistent with those of an earlier study by Abgral et al., 25 which reported that the percentage changes of SUVmax and single static volumetric parameter are independently correlated with RFS. However, current results are somewhat different from those, suggesting that percentage changes of volumetric parameter can also show prognostic significance in univariate analysis. This difference is presumed as we used the fixed threshold method to measure volumetric parameters and not relative threshold level (e.g., 40% of SUVmax within VOI). We should be aware of potential error in relative threshold. The percentage changes of metabolic volumetric parameters might be falsely corrected by higher average SUV in tumors that tend to have a very small value of MTV using a threshold of 40% of SUVmax on delayed images. We have noticed that the %ΔTLG profile using relative threshold does not seem to be significantly different, depending on disease recurrence using an independent t-test (p = 0.8503).
For RFS, percentage changes in SUVmax seemed to be superior predictive factors to single-time point SUVmax, which can be important clinically for risk stratification and treatment outcomes. This factor based on percentage changes in tumor glucose metabolism could provide effective information for functional imaging interpretation of breast cancer independently of volumetric PET parameter. Our results were in close agreement with those of previous studies, suggesting that a high retention index for SUVmax can be a predictive factor in patients with head and neck squamous cell carcinoma, malignant lymphoma, and breast cancer. 26 –28
This study had some limitations. First, we used a relatively small number of patients and retrospective design to include individual physiological features such as age, menstrual cycle, and breast tissue densities. Second, our study may have had a patient selection bias due to avoidance of partial volume effects for PET/CT, which may have led to an underestimation of FDG accumulation for small tumor lesions. 29 Third, DTP PET/CT was performed 1 and 2 hours after 18F-FDG intravenous injection, respectively. This protocol may cause somewhat inaccurate findings, especially in tumors with poor FDG uptake. However, a consensus on imaging acquisition timing has not been established.
Despite these limitations, to the best of our knowledge, this is the first study to investigate the independent prognostic significance of percentage changes in DTP PET/CT parameters, including volumetric factors and clinicopathological variables, in premenopausal patients with IDC. We demonstrated that percentage changes of SUVmax by DTP PET/CT and single time point of TLG might be considered complementary clinical factors to molecular biomarkers associated with tumor aggressiveness in IDC for predicting disease prognosis and determining individual treatment strategies. Our findings underscore the importance of identifying a subgroup with poor prognostic factors in premenopausal women who may benefit from more aggressive therapeutic strategy aimed at improving their RFS.
Footnotes
Acknowledgment
The scientific guarantor of this publication is B.S.K. The authors of this article have no relationships to declare with any companies whose products or services may be related to the subject matter of the article. This research was supported by grants from the National Research Foundation (2015R1C1A1A02037051, 2012M3A9B6055379, NRF-2015R1C1A2A01054113). Institutional review board approval was obtained and written informed consent was waived.
Author Disclosure Statement
No competing financial interests exist.