
Abstract
Introduction:
Lesbian and bisexual (LB) women are at greater risk of obesity than heterosexuals. However, few studies have examined sexual orientation differences in physical activity (PA) and even fewer have examined differences in sedentary behaviors. This study assessed PA more comprehensively than previous research by including aerobic PA, strengthening PA, and sitting time, to explore sexual orientation differences among adult women.
Methods:
Nearly 100,000 women from Nurses' Health Study II were included in multivariable-adjusted repeated measures analyses. PA and sedentary behaviors were assessed in 1989, 1991, 1997, 2001, 2005, and 2009 (age range: 24–64 years). Aerobic PA was converted to metabolic equivalent task (MET)-hours/week, whereas strengthening PA and sedentary behaviors were measured in hours/week. About 1.3% of the sample identified as lesbian (n = 926) or bisexual (n = 415).
Results:
On average over repeated measures, LB women reported engaging in 2–3 MET-hours/week more of total aerobic PA (β [95% confidence interval, CI]: lesbian: 2.0 MET-hours/week [0.6–3.4]; bisexual: 2.8 MET-hours/week [0.7–4.7]) than heterosexual women. Bisexual women reported engaging in 0.2 hours/week more of strengthening PA (95% CI: 0.06–0.42) than heterosexuals; there were no differences between lesbians and heterosexuals in strengthening PA. LB women reported sitting an average of 4–5 hours/week more than heterosexuals (lesbian: 4.1 hours/week [3.1–5.2]; bisexual: 5.1 hours/week [3.6–6.7]).
Conclusions:
Interventions promoting less sitting time among LB women may be warranted. Additionally, findings highlight need for more research into other modifiable factors besides PA, such as minority stress or disordered eating behaviors that may contribute to greater obesity among LB women.
Introduction
P
It has been well documented that lesbian and bisexual (LB) women have greater risk of overweight and obesity than heterosexual women. 6 –12 Sexual minority stress is the most common explanation for this disparity; that is, exposure to discrimination, bias, stigma, and prejudice due to the social status of being a sexual minority, negatively impacts mental, behavioral, and physical health. 13,14 However, when examining existing research on behavioral risk factors for overweight and obesity among sexual minority women, the relationship between sexual orientation, weight-related behaviors (such as PA and sedentary behaviors), and weight is complicated. In addition to minority stress, differences between heterosexual and sexual minority women in community norms that are more proximal to weight-related behaviors may also be important. For example, some literature suggests that lesbian women may be more likely than heterosexual women to reject traditional notions of femininity, including a desire for “thinness,” and to have more positive attitudes regarding their body image. 15 –18
The complexity of the relationship between sexual orientation and PA is reflected in mixed findings of existing adult population- and community-based studies that have sought to estimate differences between sexual minority and heterosexual women. 6,8,10,11,19 –29 Of 13 population-based studies of adults we identified, 8 found no differences between LB and heterosexual women in their aerobic PA, 6,8,10,20,22,23,25,29 whereas 3 found less aerobic PA 11,19,21 and 2 found more aerobic PA 24,28 among LB than heterosexual women. Of two community-based samples with a heterosexual or general population comparison group, one found more aerobic PA among lesbians than the general population of women, 26 whereas the other found no differences based on sexual orientation. 27
Studies examining sexual orientation differences in strengthening PA or sedentary behaviors are particularly lacking. Two population-based studies of adults have examined strengthening PA, 11,24 and only one has examined sedentary behaviors among sexual minority adults. 11 One study found more strengthening PA among bisexual women, 24 whereas another study found less strengthening PA among bisexual women than heterosexual women. 11 One study found no sexual orientation differences in sedentary behavior. 11
Collectively, the existing research on PA and sedentary behaviors among sexual minority women highlights several challenges and limitations. First, given the importance of engaging in strengthening PA and limiting sedentary behaviors for overall health, it is critical to understand levels of behavioral engagement among sexual minority women to identify and address this potential risk for obesity and related chronic health conditions. However, studies examining these behaviors are notably lacking with regard to sexual orientation.
Second, studies examining PA patterns in diverse populations have documented that PA decreases with increasing age, 30 –34 whereas a smaller body of research has found increasing sedentary behaviors with increasing age. 30,35 As a result, null effects in sexual orientation differences in aerobic PA could be due to a masking of important age effects. Despite this, little work has examined whether sexual orientation differences in aerobic and strengthening PA and sedentary behaviors are modified by age. One study cross-sectionally examined the interaction between PA and age and found that compared with heterosexual women, more lesbian women ages 18–49 years old reported engaging in moderate-intensity PA in the past week and more bisexual women 18–49 years old reported engaging in strengthening PA in the past week than same-aged heterosexual women. There were no sexual orientation differences in PA among participants 50 years or older. 24 We identified only one study that used longitudinal data and results suggested that on average between ages 12 and 22, sexual minority youth had lower aerobic PA than heterosexuals. 36 Findings from these two studies highlight the need for more studies that examine the effect of age on the relationship between sexual orientation and PA. We identified no studies that examined age effects on strengthening PA or sedentary behaviors by sexual orientation.
Another important consideration is the limited exploration of rurality on the relationship between sexual orientation and PA and sedentary behaviors. Rural living is a particularly important factor associated with greater obesity 37 –39 and less PA. 38,40,41 Limited evidence suggests that among LB women, rural as compared with urban living is associated with less social support, fewer community ties, and riskier health behaviors. 42 –46 Therefore, rurality has been emphasized by the Institute of Medicine as an area for further exploration with regard to sexual orientation-related health disparities. 47 One community-based study examining lesbian women's weight status and dietary behaviors found higher body mass index and PA among rural-residing lesbians than urban-residing lesbians, 48 suggesting a need to further examine rural–urban differences in sexual orientation-related health disparities. Strengthening PA and sedentary behaviors have not been explored with regard to sexual orientation and rurality.
Given the gaps in knowledge about strengthening PA and sedentary behaviors, as well as understanding aerobic PA differences over time among adults, the purpose of this study was to estimate differences in aerobic and strengthening PA and sedentary behaviors by sexual orientation among women ages 24–64. Furthermore, we tested for effect modification by age and rural living status to examine if sexual-orientation patterns in PA and sedentary behaviors were consistent or different across age periods and rural versus urban living.
Materials and Methods
Study population
The Nurses' Health Study II (NHSII) was established in 1989 and is a prospective cohort study of 116,671 female registered nurses living in 15 states in the United States who were 24–44 years of age in 1989. Nurses were recruited from state nursing boards based on age and gender. The baseline questionnaire was mailed to 517,000 women, of which 123,000 responded (24%); of these, women who returned incomplete questionnaires or reported breast cancer were excluded from the cohort. Biennial mailed questionnaires were used for follow-up, with a follow-up rate that exceeds 90% for every 2-year period. The analytic sample included participants reporting their sexual orientation (n = 99,658), although individual models vary slightly due to missing PA and sedentary behavior information and exclusion of participants reporting being pregnant for that wave.
Sexual orientation
Sexual orientation was assessed in 1995 and 2009 using the following question, “Whether or not you are currently sexually active, what is your sexual orientation or identity? (Please choose one answer).” Response options included “Heterosexual,” “Lesbian, gay, or homosexual,” “Bisexual,” “None of these,” and “Prefer not to answer.” For these analyses, reported sexual orientation in 2009 was used, except where there was missing information (i.e., not identifying as heterosexual, lesbian, or bisexual), in which case, sexual orientation reported in 1995 was used. “Heterosexual,” “lesbian,” and “bisexual” were examined separately. Participants reporting “None of these” or “Prefer not to answer” in both years were excluded from analysis. We conducted additional analyses examining results with an alternative assignment of sexual orientation. In alternative analyses, we used participants' sexual orientation reported in 1995 for waves 1991–2007 and then used 2009-reported sexual orientation in 2009. Study conclusions were similar for the two different sexual orientation categorizations.
Aerobic PA
The NHSII activity questionnaire was administered in 1989, 1991, 1997, 2001, 2005, and 2009. Participants reported their average time/week during the preceding year spent doing the following nine activities: walking, jogging, running, bicycling, lap swimming, tennis, calisthenics/aerobics/aerobic dance/rowing machine, squash or racquet ball, and performing other vigorous activities (e.g., mowing the lawn). Response options for each activity included the following 10 categories: 0, 1–4, 5–19, 20–59 minutes, 1, 1–1.5, 2–3, 4–5, 7–10, and 11+ hours. Each activity was assigned a metabolic equivalent task (MET) value, which estimates the intensity or energy expenditure required to perform a task, according to established criteria. 49 MET-hours/week for each activity were calculated by multiplying the MET value for each activity by the median response value of participant's reported category of range of PA hours/week, therefore, estimating a participant's overall energy expenditure for each activity. The MET-hours/week from all nine activities were summed to estimate total aerobic PA. Total vigorous PA included all activities, except walking.
A previous validation study of the PA questionnaire found correlations between activity reported on questionnaires and those reported through past-week activity recall or by 7-day activity diaries were 0.79 and 0.62, respectively. 50
Strengthening PA
Strengthening PA items were included in 2001, 2005, and 2009. Participants reported time spent engaging in: “lower intensity exercise (yoga, stretching, toning)” and “weight training or resistance exercise (include free weights or machines such as Nautilus).” Weight training was reported for arm weights and leg weights. Response options were the same as for aerobic PA; the midpoint of each response category was taken and summed to estimate total time spent in strengthening PA.
Sedentary behaviors
Sedentary behaviors were assessed in 1989, 1991, 1997, 2001, 2005, and 2009. Participants reported hours/week spent in sitting activities. In 1989, sitting at home was collected with one question, “How many hours per week do you spend sitting at home?” which was expanded to two items beginning in 1991, “Sitting at home while watching TV/VCR?” and “Other sitting at home [e.g., reading, meal times, at desk]?” In 1989, participants were asked, “How many hours per week do you spend sitting at work or while driving?” This question was rephrased in 1991 to, “sitting at work or away from home or while driving.” Nine response categories included: 0, 1, 2–5, 6–10, 11–20, 21–40, 41–60, 61–90, and 90+ hours. To estimate total sitting time, the midpoint of each response category was summed across types of sitting. We also examined time spent watching TV separately, given evidence this is a particularly salient behavior for chronic diseases. 5
Covariates
Age in years at time of survey completion (categorized as 24–30, 31–35, 36–40, 41–45, 46–50, 51–55, 56–60, and 61–64), race/ethnicity (non-Hispanic white vs. other), rural versus urban living (based on zip code, defined as <500 persons/square mile), 51 region of residence (Northeast, Midwest, South, and West), and household income in 2001 (<$50,000, $50,000 to <$75,000, $75,000 to $100,000, >$100,000, and missing) were included as covariates. Age, rural living, and region of residence were updated at each wave of data. Income was only assessed in 2001 and therefore, not time varying.
Statistical analyses
Six data waves of aerobic PA and sedentary behavior (1989, 1991, 1997, 2001, 2005, and 2009) and three waves of strengthening PA (2001, 2005, and 2009) were used in these analyses.
To assess sexual orientation differences in sociodemographic characteristics, Wald chi-square tests were performed. In examining the relationship between sexual orientation and PA and sedentary behaviors, several models were fit. We first estimated age-standardized means of PA and sedentary behavior measures across available waves of data and tested for differences using age-adjusted likelihood ratio tests. We then examined general patterns of PA and sedentary behavior measures using unadjusted means for each age group across sexual orientation categories. Finally, to test for sexual orientation differences in PA and sedentary behaviors, repeated measures analyses using generalized estimating equations (to account for within-person correlation) were conducted to estimate the population average over multiple waves of data. Linear regression models were fit for all outcomes. Both crude and covariate-adjusted models were fit and results were similar, therefore, we present adjusted results only. Heterosexuals were the referent group and each parameter estimate for lesbians and bisexuals are differences compared with heterosexuals. Additionally, we examined two sets of interaction models to assess sexual orientation differences by age period and by rural living. Furthermore, in sexual orientation-by-age interaction models, we further controlled for age at baseline to account for cohort effects; however, this did not change results. Analyses were conducted using SAS version 9.3 (2010; SAS Institute, Inc.). This study was approved by the Institutional Review Board at Brigham and Women's Hospital and the Human Subjects Committee at the T.H. Chan Harvard School of Public Health.
Results
Sociodemographic differences across sexual orientation are presented in Table 1. In this sample, heterosexual women were younger at baseline than lesbian women, a smaller proportion of bisexual women were white, and a larger proportion of heterosexual women reported household incomes more than $100,000/year in 2001 than LB women. Using available waves of data, more heterosexuals lived in the Midwest than LB women, and a greater proportion of heterosexual women lived in rural areas than lesbians.
Calculated from Wald chi-square test; compared with heterosexual women.
Age-standardized prevalence over all available waves for region of residence and rural living.
p-Values for region of residence were calculated from separate logistic regression repeated measures models.
Age-standardized means of PA measures and sitting time across available waves are presented in Table 2. Adjusting for age only, there were significant differences in PA and sitting time across sexual orientation for nearly every measure, except walking, running, and weight training. Lesbians engaged in less aerobic activities such as dance, ski, or stair machine, although they played more tennis/squash/racquetball and other vigorous activities than heterosexuals. There were no differences between bisexuals and heterosexuals for these activities. Generally, LB women reported engaging in more PA and sitting time (particularly sitting at work or away from home) than heterosexuals.
Values are means (SD) and are standardized to the age distribution of the study population.
p-Values were generated from likelihood ratio test of age-adjusted repeated measures models.
MET, metabolic equivalent task; SD, standard deviation.
Figure 1 shows unadjusted mean levels of PA and sitting time from ages 24 to 64 by sexual orientation. Total aerobic PA and vigorous PA levels were lowest among heterosexuals. Bisexuals reported spending most of the time in strengthening PA. Finally, while there were differences in total sitting time across sexual orientation, with heterosexuals reporting the least amount of sitting, there did not appear to be sexual-orientation differences in time spent watching TV.
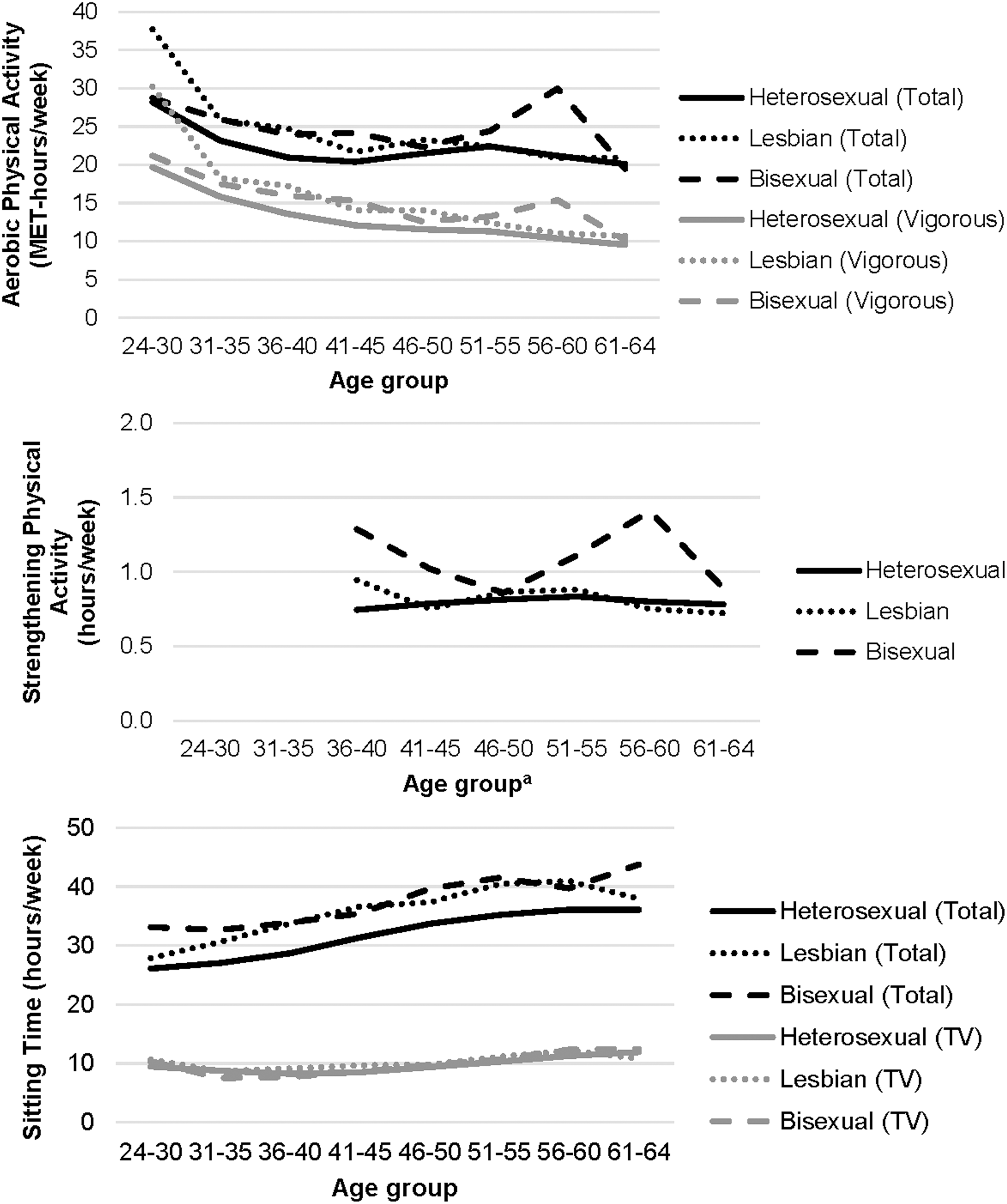
Unadjusted means of aerobic physical activity, strengthening physical activity, and sitting time by sexual orientation among women participating in the Nurses' Health Study II (1989–2009). MET, metabolic equivalent task. aEstimates not available before ages 36–40 because strengthening physical activity was not assessed until 2001.
Results from multivariable adjusted regression models are presented in Table 3. Compared with heterosexual women, lesbian women reported engaging in 2.0 more MET-hours/week (95% confidence interval [CI]: 0.6–3.4) of total aerobic PA, whereas bisexual women reported even more (2.8 MET-hours/week: 0.8–4.8). When examining vigorous PA specifically, both LB women reported about 2.3 MET-hours/week more than heterosexual women. There were notable findings from interaction models that can be observed in crude models (Fig. 1). A greater difference in total aerobic PA existed between lesbians and heterosexuals between ages 24 and 40 years, with lesbians engaging in more PA; by age 41, a substantial decrease in total aerobic PA among lesbians yielded similar PA to heterosexuals. Furthermore, sexual orientation-by-rurality models (Fig. 2) indicated a greater difference between bisexuals and heterosexuals in rural settings than urban, with bisexuals engaging in significantly more aerobic PA in rural settings (p = 0.02). There were no sexual orientation-by-rurality differences for lesbians. Similar differences in total vigorous PA were observed.
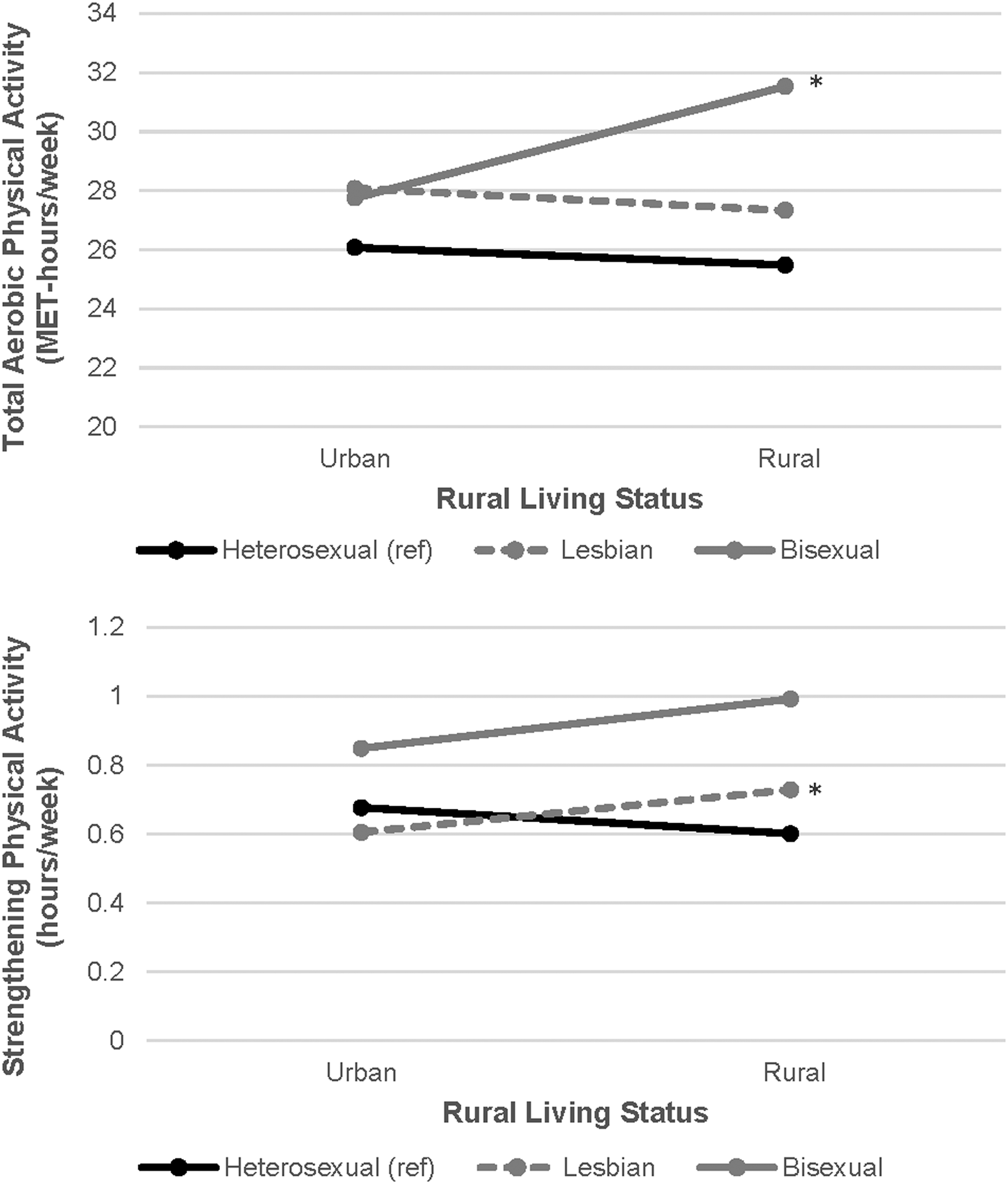
Interaction effects of sexual orientation-by-rural living status on total aerobic physical activity and strengthening physical activity among women participating in the Nurses' Health Study II. *Interaction is significant at p < 0.05 compared to hetrosexual women.
Adjusted for age group at outcome measurement, race/ethnicity, rural living, region of residence, and household income in 2001.
Includes walking, jogging, running, biking, other aerobic activity, swimming, tennis, and other vigorous activity.
Excludes walking.
Includes sitting at work or away from home, sitting at home to watch TV, and other sitting at home.
p < 0.05; ** p < 0.01; *** p < 0.001.
For strengthening PA, bisexuals engaged in about 0.2 more hours/week than heterosexuals. Lesbians and heterosexuals engaged in similar amounts of strengthening PA. Sexual orientation-by-rurality interaction models (Fig. 2) suggested that while urban-residing lesbians engaged in less strengthening PA than urban-residing heterosexuals, rural-residing lesbians engaged in more strengthening PA than rural-residing heterosexuals (p = 0.04). Both LB women reported more time sitting than heterosexuals (lesbian: 4.1 hours/week [3.1–5.2]; bisexual: 5.1 hours/week [3.6–6.7]). Lesbians spent 0.6 hours/week more watching TV than heterosexuals (95% CI: 0.1–1.1); however, there were no differences between bisexuals and heterosexuals. There were no significant sexual orientation-by-age differences for strengthening PA or sitting time and no sexual orientation-by-rurality differences for sitting time.
Discussion
Based on over 20 years of longitudinal data from a large cohort of women with a >90% follow-up rate, we found that LB women evidenced greater PA, particularly for aerobic PA than heterosexuals. However, we also found that LB women reported more sedentary behaviors than heterosexuals. Furthermore, aerobic PA among lesbians decreased more rapidly during middle adulthood than among heterosexuals. Findings from our study do not seem to be entirely consistent with the hypothesis that LB women may experience disparities in PA and sedentary behaviors due to their likelihood of adopting unhealthy behaviors to cope with minority stress. Rather, our findings underscore the importance of considering more complex models, possible by incorporating other important determinants, including sociocultural and community-oriented norms (e.g., rejection of heteronormative body image ideals among lesbian women) 15 –18 that uniquely relate sexual identity to PA and sedentary behaviors and potentially provide more context for our descriptive findings.
More PA in our sample of LB women compared with heterosexuals is inconsistent with previous cross-sectional studies which largely found no difference or less PA. 6,8,10,11,19 –23,25,27 This inconsistency in findings could be due to differences in PA measurement. We used MET-hours/week to quantify intensity and time. Brief screeners were used in population-based studies and measurement varied between studies, with some quantifying PA time within an intensity category and dichotomizing based on PA recommendation categories, whereas others examined whether participants reporting engaging in PA at all. Recent PA recommendations were based on the minimum amount needed for a substantial decrease in morbidity and mortality compared with no PA at all. 52 Recommendations additionally highlight the importance of a dose–response, where more PA than the minimum provides further health benefits. Using MET-hours/week allows us to more robustly examine changes in activity level over a time period (1989–2011) when PA recommendations have evolved from a performance focus to a more health-oriented and public health focus. 52 Most population-based studies examining PA and sexual orientation have been since 2000, when PA recommendations were more public health focused. 6,8,10,11,20 –25
Interestingly, one finding was the marked decline in aerobic PA among lesbians from young to middle adulthood. The majority of young adults in our sample were in this age group during the 90s, when the obesity epidemic was first being recognized and PA recommendations were starting to focus on health benefits. It is unclear if these sociocultural changes may have more adversely impacted PA among lesbians than other sexual orientation groups. However, this further highlights the importance of using a life course approach to understand how individual trajectories and cohort effects affect sexual minority health. 47,53
While rurality has been frequently conceptualized as a social context that could yield riskier health behaviors due to exposure to increased stigmatization and discrimination toward sexual minorities, existing research findings that support this general idea of a negative association between rurality and sexual minority health have been mixed. For example, in qualitative interviews with rural-residing gay and lesbian adults in the Midwest, participants highlighted unique ways in which lesbian and gay rural residents have integrated their sexual identity with their rural environment and how it may differ in urban environments. Furthermore, participants identified how certain characteristics of rural living, such as the “close-knit nature” created a sense of implicit acceptance and safety. 54 Our findings contribute to the nuanced role of rural settings on the health of sexual minorities, as we found that rural-residing LB women may be more physically active than rural-residing heterosexuals. 47 PA in rural populations is understudied, although some studies suggest lower PA in rural than urban residents. 38,40,41 The rural context for LB women is unique 15,54 and may partially explain our findings. For example, rural-residing LB women may have more body satisfaction 15 than in general, predominantly urban, community samples, 55 although, these issues remain highly understudied. Further examination of sociocultural factors within rural-residing LB communities could inform PA promotion interventions in rural settings generally.
Our finding that LB women spent more time than heterosexuals sitting is an area of concern, as this behavior may increase their diabetic, cardiometabolic, and mortality risk. 2 –4 Interestingly, when we examined time spent watching TV, differences in sitting time diminished substantially across sexual orientation, with lesbians watching about half an hour/week more TV than heterosexuals. This finding suggests that multifaceted interventions are likely needed that address the social and cultural aspects of sitting time in settings besides TV viewing. From a more clinical perspective, interventions that improve healthcare provider knowledge and understanding of behaviors that negatively affect sexual minority women's health, such as sitting time, is critical in helping to shift some of the social and cultural factors negatively influencing health.
This study was novel because we longitudinally examined PA, including strengthening PA, and sitting time during adulthood by sexual orientation. Findings add to the scant literature on disparities in PA and sedentary behaviors by sexual orientation. However, the sample of nurses is not representative of the general population, thus limiting generalizability of findings. This may explain why our findings differ from population-based studies; yet, because examination and assessment of PA and sedentary behaviors is inconsistent across studies, more research is needed to examine this issue. Furthermore, data were self-reported; therefore, measurement error and misclassification may exist, most notably, measurement of activity is a crude estimate compared with more objective measures such as accelerometry.
Conclusions
Overall, findings from the NHSII cohort suggest that LB women are more physically active than heterosexuals; although, there is a significant decline in PA among lesbians during middle adulthood such that the amount of PA between lesbian and heterosexual women are similar during middle adulthood and older. Understanding factors that promoted PA during young adulthood and that contributed to the decline in PA may be beneficial in developing PA interventions to improve PA among other sexual orientation groups and to help prevent significant declines in PA levels. Moreover, interventions to reduce sitting time among LB women, particularly away from home, may be needed. Given existing research documenting more overweight and obesity among LB women than heterosexuals, additional work is needed to understand the complex relationships between weight-related behaviors, minority stress, weight status, and health outcomes among sexual minority women.
Footnotes
Acknowledgments
The research presented in this article is that of the authors and does not reflect the official policy of the NIH. This study was supported by Award Numbers DK099360, DK58845, and UM1CA176726 from NIH.
Author Disclosure Statement
No competing financial interests exist.