
Abstract
Background:
Counseling for appropriate medication use and folic acid consumption are elements of preconception care critical for improving pregnancy outcomes. Hispanic women receive less preconception care than women of other race/ethnic groups. The objective of this analysis is to describe differences in these two elements of preconception care among Hispanic subsegments.
Materials and Methods:
Porter Novelli's 2013 Estilos survey was sent to 2,609 U.S. Hispanic adults of the Offerwise QueOpinas Panel. Surveys were completed by 1,000 individuals (calculated response rate 42%), and results were weighted to the 2012 U.S. Census Hispanic proportions for sex, age, income, household size, education, region, country of origin, and acculturation. Responses were analyzed with weighted descriptive statistics, linear regression, and Rao–Scott chi-square tests.
Results:
Of the 499 female respondents, 248 had a child under the age of 18 years and were asked about healthcare provider discussions concerning medication use before or during their last pregnancy. Timing of discussions varied by maternal age, marital status, income, youngest child's country of birth, and acculturation. Discussions before pregnancy were reported by 47% of the female respondents; high acculturated women more often reported never having such discussions. Among female respondents, 320 were of reproductive age, and 27% of those reported daily multivitamin use. Multivitamin use varied by pregnancy intention and youngest child's country of birth, but did not vary significantly by acculturation.
Conclusions:
Differences in discussions concerning medication use in pregnancy and multivitamin use exist among Hispanic subsegments based on pregnancy intention, marital status, income, youngest child's country of birth, and level of acculturation.
Introduction
G
Somewhat surprisingly, few studies were found that examined the role of racial and ethnic disparities on preconception health and healthcare, 7 and those that were found focused primarily on the outcomes of birth weight and preterm birth. For example, a report by the March of Dimes found rates of preterm births for black, Hispanic, and Native American mothers to be higher than those for white mothers. 8 Furthermore, among women of certain race/ethnic subpopulations, unintended pregnancy rates are especially high, making preconception care of critical importance. 8
As of 2011, rates of unintended pregnancies resulting in births were higher among Hispanic women in the United States compared with non-Hispanic white women (45.3% vs. 36.6%, respectively). 9 Even for intended pregnancies, Hispanic women were more likely than non-Hispanic white women to report that a pregnancy was mistimed (i.e., occurred earlier than desired) (27.0% vs. 20.8%, respectively). 9 Finally, among Hispanics, the fastest growing minority group in the United States, 10 preconception health behaviors might be impacted as the level of acculturation to life in the United States increases.
Some studies have found conflicting evidence about the impact of acculturation in the United States on both health behaviors and birth outcomes. 11 –15 Other studies have found acculturation to be protective. 16 –18 In this article, we focus on two preconception interventions—discussions about medication use and multivitamin consumption—that impact all women, but are of particular importance to Hispanic women and may be affected by acculturation.
Studies have shown the positive impact of preconception counseling on health behaviors before pregnancy. 19 –21 Although this counseling is important for all women, the presence of race/ethnic health disparities for certain health outcomes can indicate particular importance of the need for preconception counseling around issues such as medication use and folic acid consumption. 22
Discussions about medication use
Preconception discussions with healthcare providers should address the issue of safe medication use and effective treatment alternatives. 23 This is because taking certain medications during early pregnancy can increase the risk of having a child with a birth defect. 24 Currently, 11.7 million prescriptions of potentially teratogenic medications are given to women of reproductive age annually. 25 Because many healthcare providers do not inquire about women's pregnancy intention or provide contraception counseling when prescribing potentially teratogenic medications, they might miss opportunities to promote safe alternatives to women who are taking potentially harmful medications. 26 Additionally, disparities in counseling exist, with Hispanic women being less likely than non-Hispanic black women to report being counseled by a healthcare provider about medication use during the preconception period. 20
Multivitamin consumption
In 1992, the U.S. Public Health Service issued a recommendation that all women in the United States capable of becoming pregnant should consume 400 μg of folic acid daily by consuming a combination of fortified foods and/or supplements such as multivitamins that contain folic acid. 27 Consuming folic acid before conception is key to preventing NTDs because they occur within the first 28 days of pregnancy, most often before a woman knows she is pregnant. 28 In the United Sates, however, only 28.5% of women of reproductive age report consuming a folic acid-containing supplement and, of those, only 13.8% report consuming a supplement containing ≥400 μg daily. 29 In addition, disparities in folic acid knowledge and consumption exist. Hispanic women report lower knowledge about the benefits of folic acid and lower folic acid consumption than women of other ethnic groups. 20,30 –32 Hispanic women also have higher rates of certain types of NTDs. 17,33 –35
Objective
Given the significant size of the Hispanic population in the United States 36 and the recognized disparities in selected preconception health behaviors among race/ethnic groups, we sought to better understand two risk reduction preconception health behaviors—discussions about medication use and multivitamin consumption—among Hispanics.
Materials and Methods
During October and November 2013, Porter Novelli's 2013 Estilos survey was sent to 2,609 Hispanic adults aged 18 years or older. Estilos is a web-based survey of U.S. Hispanic adults designed to measure attitudes and behaviors spanning a range of issues, including health and wellness. Estilos participants are drawn from the Offerwise QueOpinas Panel, * the largest online U.S. Hispanic panel with over 210,000 active panelists who are recruited nationally through both English and Spanish network television. To prevent unbalanced results, limits on the numbers of panelists were used for age, language, level of acculturation, region, gender, and heritage.
The survey took a median of 42 minutes to complete. Respondents could choose to respond to the survey in either English or Spanish, were not required to answer any of the questions, and could exit the survey at any time. Those who completed the survey received reward points worth approximately $15. A total of 1,000 individuals completed the survey for a calculated response rate of 42%, which takes into account surveys that were not completed due to filled quotas. The resulting data were weighted to match the 2012 U.S. Census American Community Survey Hispanic proportions for sex, age, household income, household size, education level, census region, country of origin, and level of acculturation.
The acculturation level, predetermined by Offerwise and classified as low, medium, and high, was assessed from responses provided to four questions: (1) How many years have you lived in the United States? (2) What language do you usually speak at home? (3) Thinking of your overall cultural identification, would you say you feel… (Likert scale responses ranged from Much Closer to the Hispanic/Latino Culture to Much Closer to U.S. Culture), and (4) Thinking of your media habits, including television, radio, newspapers, and magazines, or the internet, would you say you use…(Likert scale responses ranged from Spanish media only to English media only).
This analysis focused on two questions in the survey among two overlapping groups of respondents (Fig. 1). The first question assessed the presence and timing of discussions about medication use in pregnancy: Either before or during your last pregnancy, did your healthcare provider (nurse, doctor, or other professional) speak with you about medication use during pregnancy? This question was only asked of women who had a child under the age of 18 years at the time of the survey. The second question assessed multivitamin use: Please tell us approximately how often you usually take a multivitamin. Do you do it daily, weekly, monthly, less than once a month, or never? This question was asked of all survey respondents; however, because the focus of this article is on preconception health behaviors, we only analyzed responses provided by women of reproductive age (18–44 years). Additionally, because the survey only asked about multivitamin use and we were interested in folic acid consumption as a preconception health behavior, we used multivitamin intake as a proxy for folic acid consumption.

Derivation of study cohort.
To better understand whether the risk reduction behaviors might have occurred in the United States, we wanted to know whether a woman's youngest child was born in the United States. We calculated this variable based on whether the age of the respondent's youngest child was less than, or greater than, the range of years that the respondent stated she had lived in the United States. Because the survey question was designed to collect the number of years living in the United States based on 5-year ranges (i.e., 0–4, 5–9, 10–14, 15–19, and 20+), if the child's age fell within the range of years since the respondent moved to the United States, the child's country of birth could not be ascertained. Therefore, we classified this variable as unknown in such situations. Because of the potential for misclassification, we conducted a sensitivity analysis in which we ran two additional tests, one in which we added all of the children with unknown birth countries into the U.S.-born group and another in which we added all of the children with unknown birth countries into the non-U.S.-born group.
We analyzed the following demographic characteristics: age at survey, pregnancy intention, marital status, education level, employment status, annual household income, youngest child's country of birth, level of acculturation, and year of youngest child's birth. All descriptive statistics are presented as weighted percentages, means, and standard errors. We analyzed continuous variables using simple linear regression and categorical variables using Rao–Scott chi-square tests. p-Values <0.05 were considered significant. All analyses were carried out using SAS, version 9.3 (SAS Institute, Inc., Cary, NC).
Results
Discussions about medication use
Among the 1,000 Estilos respondents, 499 were female. A weighted 39% of women surveyed reported having a child under the age of 18 years at the time of the survey and were, therefore, eligible to be asked about discussions with their healthcare provider regarding medication use and their last pregnancy. Of those women, approximately one-fifth (19.6%) reported never having these discussions with their healthcare provider, while 80.4% reported ever discussing medication use and pregnancy. We stratified the ever response category into before pregnancy and during pregnancy only and found that 46.7% reported discussions before pregnancy, while 33.7% reported discussions during pregnancy only (Table 1).
Weighted percentages: Data weighted to match the 2012 U.S. Census American Community Survey Hispanic proportions for sex, age, household income, household size, education level, census region, country of origin, and acculturation level.
Simple linear regression was used for the continuous age and year of youngest child's birth variables, Rao–Scott chi-square tests were used for all other variables analyzed.
Women who reported being currently pregnant (1.4% ever, 1.3% before pregnancy, 1.4% during pregnancy only, and 0% never) were excluded from analysis of this variable because of small numbers.
Includes “I do not want to have any/anymore” and “Not applicable: hysterectomy/menopause.”
Other includes Argentina, Bolivia, Chile, Colombia, Costa Rica, Dominican Republic, Ecuador, El Salvador, Guatemala, Honduras, Nicaragua, Panama, Paraguay, Peru, Spain, Uruguay, and Venezuela.
Calculated based on whether the age of the respondent's youngest child was less than or greater than the range of years that the respondent stated that she had lived in the United States. Years in the United States was collected based on 5-year ranges (i.e., 0–4, 5–9, 10–14, 15–19, and 20+); therefore, if the child's age was within the range of years since the respondent moved to the United States, this variable was considered unknown.
Acculturation level (predetermined by Offerwise) was based on the number of years living in the United States, language spoken at home, cultural self-identification, and the use of Spanish language media.
When the discussion of medication use was categorized into ever and never, it was significantly associated with marital status (less frequent among single women), youngest child's country of birth (less frequent among women whose youngest child was born in the United States), and acculturation (less frequent among women with high acculturation) (Table 1). When the discussion of medication use was categorized into before pregnancy, during pregnancy only, and never, it was significantly associated with age, marital status, income, country of origin, and youngest child's country of birth (Table 1). For both categorizations, the discussion of medication use was significantly associated with acculturation among women whose youngest child was born between 1996 and 2005 (children born 8–17 years before the survey), but was not significantly associated with acculturation among women whose youngest child was born between 2006 and 2013 (0–7 years before the survey) (Table 1). The trend of decreased proportions of women from low to high acculturation having these discussions with their healthcare provider remained regardless of the length of time between the child's birth and the survey (Figs. 2 and 3).
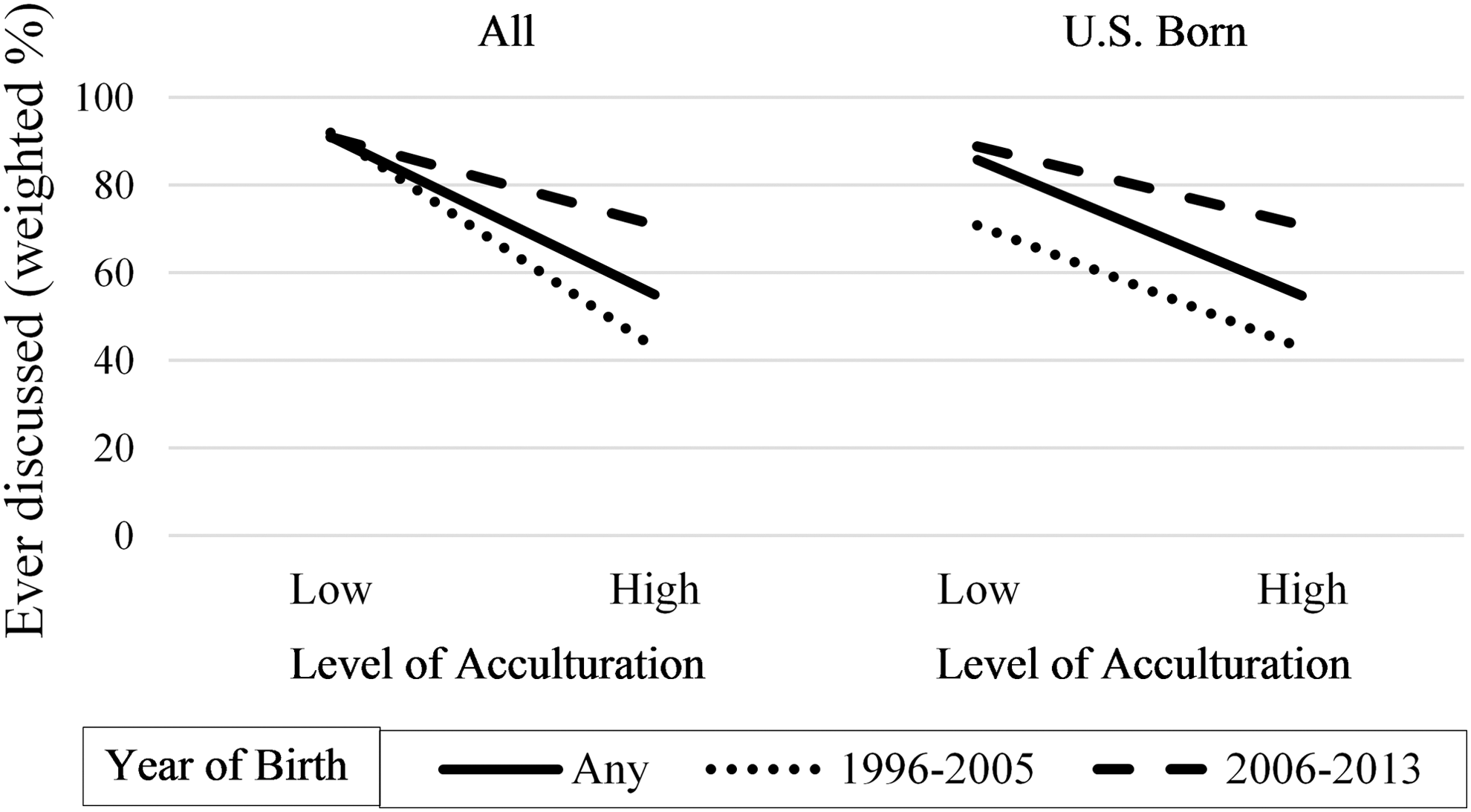
Association between ever having a discussion with healthcare providers about medication use and pregnancy, level of acculturation, and year of child's birth among female participants in the Estilos survey with children under the age of 18 years. Year of birth: any (solid line), 1996 through 2005 (dotted line), and 2006 through 2013 (dashed line).
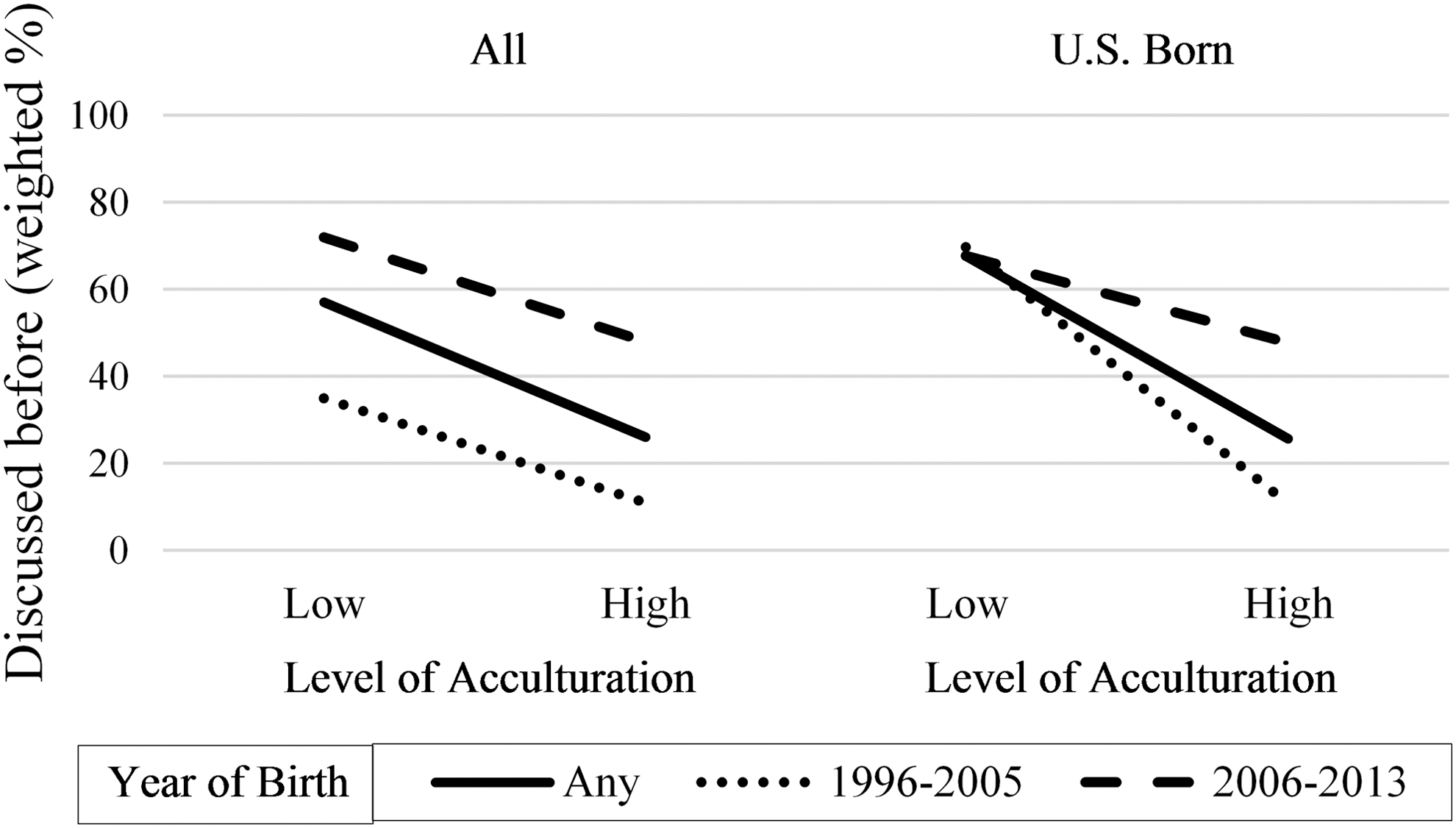
Association between a discussion with healthcare providers before pregnancy about medication use in pregnancy, level of acculturation, and year of child's birth among female participants in the Estilos survey with children under the age of 18 years. Year of birth: any (solid line), 1996 through 2005 (dotted line), and 2006 through 2013 (dashed line).
Multivitamin consumption
Among the 499 female respondents who were asked about their multivitamin use, 320 were of reproductive age and were included in the analysis. As specified in Table 2, 26.7% indicated daily multivitamin consumption, while 73.3% reported less than daily consumption. Among the demographic factors examined, daily multivitamin consumption only varied significantly by youngest child's country of birth (more frequent among women whose youngest child was born in the United States). However, among women intending to become pregnant within a year, only 26% reported daily multivitamin consumption.
Weighted percentages: Data weighted to match the 2012 U.S. Census American Community Survey Hispanic proportions for sex, age, household income, household size, education level, census region, country of origin, and acculturation level.
Simple linear regression was used for the continuous age at survey and age of youngest child variables, Rao–Scott chi-square tests were used for all other variables analyzed.
Women who reported being currently pregnant (1.6% daily, 1.9% less than daily, 3.2% weekly, 0% monthly, 1.4% less than once a month, and 1.9% never) were excluded from analysis because of small numbers.
Includes “I do not want to have any/any more” and “Not applicable: hysterectomy/menopause.”
Other includes Argentina, Bolivia, Chile, Colombia, Costa Rica, Cuba, Dominican Republic, Ecuador, El Salvador, Guatemala, Honduras, Nicaragua, Panama, Paraguay, Peru, Spain, Uruguay, and Venezuela.
Calculated based on whether the age of the respondent's youngest child was less than or greater than the range of years that the respondent stated that she had lived in the United States. Years in the United States was collected based on 5-year ranges (i.e., 0–4, 5–9, 10–14, 15–19, and 20+); therefore, if the child's age was within the range of years since the respondent moved to the United States, this variable was considered unknown.
Acculturation level (predetermined by Offerwise) was based on the number of years living in the United States, language spoken at home, cultural self-identification, and the use of Spanish language media.
We stratified the less than daily response category into weekly, monthly, less than once a month, and never. Approximately 13% reported consuming a multivitamin weekly, 7.0% reported monthly, and 14.2% reported less than once a month, while 39.2% reported never consuming a multivitamin (Table 2). The frequency of multivitamin consumption varied significantly only by timing of pregnancy intention.
Sensitivity analysis
For ∼20% of the women in the study, we were not able to calculate whether a woman's youngest child was born in the United States. Because this variable was significantly associated with both preconception health factors that we studied, we conducted a sensitivity analysis for these factors. First, we assumed that all of the unknown responses were in the U.S.-born group. Under this assumption, only the discussion of medication use categorized into before pregnancy, during pregnancy only, and never was significant (Table 3), whereas multivitamin consumption was not significant (Table 4). Then, we assumed that all of the unknown responses were in the non-U.S.-born group. Under this assumption, the discussions of medication use categorized into ever and never and multivitamin consumption categorized into daily and less than daily were significant (Tables 3 and 4).
Weighted percentages: Data weighted to match the 2012 U.S. Census American Community Survey Hispanic proportions for sex, age, household income, household size, education level, census region, country of origin, and acculturation level.
Rao–Scott chi-square tests were used for all variables analyzed.
Calculated based on whether the age of the respondent's youngest child was less than or greater than the range of years that the respondent stated that she had lived in the United States. Years in the United States was collected based on 5-year ranges (i.e., 0–4, 5–9, 10–14, 15–19, and 20+); therefore, if the child's age was within the range of years since the respondent moved to the United States, this variable was considered unknown.
Weighted percentages: Data weighted to match the 2012 U.S. Census American Community Survey Hispanic proportions for sex, age, household income, household size, education level, census region, country of origin, and acculturation level.
Rao–Scott chi-square tests were used for all variables analyzed.
Calculated based on whether the age of the respondent's youngest child was less than or greater than the range of years that the respondent stated that she had lived in the United States. Years in the United States was collected based on 5-year ranges (i.e., 0–4, 5–9, 10–14, 15–19, and 20+); therefore, if the child's age was within the range of years since the respondent moved to the United States, this variable was considered unknown.
Discussion
In our survey of Hispanic women in the United States, we identified key missed opportunities for improved preconception care in the areas of discussions about medication use and multivitamin (as a proxy for folic acid) consumption for this audience. Fewer than half of the women in the survey reported having discussed medication use with their healthcare provider before their pregnancy. As a result, many were likely to be unaware of the risks and contraindications of potentially teratogenic medications they might have been using at the time of conception or might have used during the course of their pregnancies. Furthermore, almost one-fifth of women never had these discussions with a healthcare provider, suggesting that for future pregnancies, they would remain unaware of potential risks from medication use. Healthcare providers could increase awareness and decrease ethnic disparities in preconception care by ensuring that they discuss medication use and pregnancy before pregnancy with all Hispanic women of reproductive age.
In addition to gaps in discussing medication use, we found that nearly three-quarters of women intending to become pregnant within a year reported not taking a multivitamin daily, including nearly one-quarter who reported no multivitamin use. Taking a daily multivitamin that contains folic acid is one way that women can ensure that they are getting enough folic acid every day, which is of particular importance for the prevention of NTDs. Thus, the low daily multivitamin use reflected in our findings might suggest that many Hispanic women of reproductive age are at a potentially elevated risk of having an NTD-affected pregnancy. This missed opportunity for prevention could be addressed through more effective messages about the importance of taking folic acid supplements. 37
We also found that some demographic factors were associated with preconception care among Hispanic women. For example, youngest child's country of birth, either within or outside of the United States, was related to both medication discussions and multivitamin consumption. Women whose youngest child was born in the United States more often reported daily multivitamin consumption. These women also more often reported discussions about medication use before pregnancy if they ever had such discussions, yet these same women more often reported that they never had these discussions compared with women whose youngest child was not born in the United States. While these mixed findings are difficult to interpret, missed opportunities for preconception care could be related to language or other cultural barriers that need to be overcome. Furthermore, these barriers could be tied to women's level of acculturation.
The impact of acculturation on a myriad of health behaviors has received a great deal of attention in the recent literature; however, findings are mixed. 11 –18 In this study, while we did not find an association between multivitamin consumption and level of acculturation, we did find that the relationship between acculturation and discussions about medication use is complex. Generally, discussions of medication use were lower as acculturation was higher. It appears, however, when categorized into ever and never, this association was primarily driven by women who gave birth between 1996 and 2005 compared with births between 2006 and 2013. This could be due to recall bias.
When specifically examining medication discussions before pregnancy, discussions were more often reported among women who gave birth between 2006 and 2013. This could represent clinical practice changes by healthcare providers in which they have only more recently begun to discuss medication use with patients before they become pregnant, as supported by a study utilizing data from the Pregnancy Risk Assessment Monitoring System. 38 However, discussions of medication use before pregnancy were still lower among women with high acculturation, regardless of the year of birth. Furthermore, when restricted to women whose youngest child was born in the United States, results were similar. These large differences by level of acculturation suggest that more studies are needed to better understand the role acculturation plays in preconception health behaviors and what public health professionals can do to address the needs of women at all levels of acculturation.
Our findings are subject to several limitations. First, because women were asked about discussions of medication use around the time of their last pregnancy, and the mean year of youngest child's birth was 2006, there is potential for inaccurate recall. However, when we restricted analyses to women whose children were born closer to the time of the survey, while no longer significant, women with high acculturation reported fewer medication discussions than women with low acculturation. Second, our findings probably overestimate the utility of discussions about medication use since it is unknown whether a respondent's healthcare provider was knowledgeable about whether and which medications are unsafe during pregnancy. Third, we were unable to identify if women had medical conditions for which they were prescribed medication, and women with medical conditions would likely have conversations with healthcare providers and recall those conversations. Fourth, the question about multivitamin use asked respondents whether they took a multivitamin without specifying its folic acid content. Although most multivitamins sold in the United States contain at least 400 μg folic acid, 39 the actual percentage of women taking multivitamins with folic acid may be lower than our estimates. Fifth, the multivitamin use question asked women about their current multivitamin use and not about their multivitamin use during pregnancy. We cannot assume that because a woman reports taking a multivitamin now, she also took it during pregnancy, or vice versa. However, when examining only women reporting intending pregnancy within the next 2 years, there were no changes in significance for any of the variables examined. Sixth, because we were unable to calculate whether a woman's youngest child was born in the United States for a substantial portion of the women in the study, there is a potential for information bias. However, because the results did not greatly change in the sensitivity analyses, this bias is likely minimal. Seventh, because this was a web-based survey, only individuals with a computer or device with Web accessibility would have been able to respond. Eighth, more than 60% of Hispanics were of Mexican origin, 10% were of Puerto Rican origin, and the other 18 countries reported were lower than 3% each, making it difficult to distinguish between differences in country-specific practices. Ninth, because this is a secondary analysis of survey data, the results likely reflect biases of the original survey itself. However, the use of these data provides insight into an area that has been underexamined to date (i.e., preconception health behaviors within the Hispanic population) and highlights the need for continued examination. Last, the acculturation variable was predefined in the database (i.e., not developed by the authors). It is unknown whether the variables used to develop the acculturation variable were the optimal variables to support the determination of an acculturation classification, and it is unknown how low versus medium versus high acculturation were specifically defined. Despite these limitations, our study helps further an understanding about racial and ethnic disparities within the Hispanic population related to preconception health behaviors.
Conclusions
We identified missed opportunities for improved preconception care in the areas of discussions about medication use and folic acid consumption. These preconception health behaviors remain critically important to ensuring healthy pregnancies. Within the Hispanic population, disparities in these behaviors persist, underscoring the need for healthcare providers to ensure that women are well informed about how to have a healthy pregnancy even when they are not actively considering becoming pregnant. Seizing these opportunities will be necessary to reduce race/ethnic disparities that currently exist in pregnancy outcomes. 22,40 Healthcare providers and public health professionals are often a primary source of information about preconception health behaviors that can help women reduce their risk of having a pregnancy affected by a birth defect. Ensuring that women who take potentially teratogenic medications are counseled about their options before pregnancy and encouraging all women of reproductive age to consume folic acid daily are two ways that healthcare providers and public health professionals can help women lower their risk of having an adverse pregnancy outcome.
Footnotes
Acknowledgment
This project was supported, in part, by an appointment to the Research Participation Program at the National Center on Birth Defects and Developmental Disabilities, U.S. Centers for Disease Control and Prevention (CDC), administered by the Oak Ridge Institute for Science and Education through an interagency agreement between the U.S. Department of Energy and CDC.
Disclaimer
The findings and conclusions in this report are those of the author(s) and do not necessarily represent the official position of the U.S. Centers for Disease Control and Prevention.
Author Disclosure Statement
No competing financial interests exist.