
Abstract
United Nation's Sustainable Development Goals and the World Health Organization's Global Monitoring Framework support a strong global commitment to reducing the high burden of cervical and breast cancers among low- and middle-income countries. Strategies include vaccination, screening, and early diagnosis. Population-based surveys, such as those conducted by the Demographic and Health Surveys (DHS) Program, can collect the information needed to guide cancer control efforts in a standardized comparable manner. We identified and evaluated the breadth of breast and cervical cancer screening information that was collected by the DHS from 1984 through 2015. Then, we determined if these surveys currently provide the specific and measurable data about both the quantity and quality of cancer screening needed to guide national efforts to reduce the overall effects of cervical and breast cancers. We searched the DHS website to identify surveys conducted between the start of the DHS Program in 1984 and November 2015 that included questions about breast and cervical cancer screening. The relevant questions were extracted from the questionnaire, translated into English, and grouped by themes. Of the 90 countries where DHS surveys have been implemented, cervical cancer screening questions were included in 22 countries (24.4%) and breast cancer screening questions in 18 countries (20.0%). The common themes identified were disease knowledge, screening knowledge, screening practice, and screening outcomes. Most countries with survey questionnaires available for review addressed at least one aspect of screening practice (88.9% of cervical and 87.5% of breast), although few countries queried knowledge and outcomes. Questions that assess varied aspects of breast and cervical cancer screening have been incorporated into relatively few DHS surveys. The themes identified could guide the design of a standard set of questions for use in future population-based surveys and enable evaluation beyond the existence of screening, which would include assessment of the quality and impact of cervical and breast cancer screening.
Introduction
C
The World Health Organization (WHO) recommends a life course approach to global cervical cancer control. 3 This approach includes HPV vaccination for boys and girls aged 9–13 years, a minimum of once in a lifetime cervical cancer screening for women aged 30–49 years, treatment of precancers and cancers, and access to appropriate palliative care, as needed. Cervical cancer screening can include HPV testing, visual inspection methods, and cytology, where available. The Breast Health Global Initiative has developed evidence-based, culturally appropriate, and economically feasible screening guidelines to improve breast cancer outcomes. 5 The WHO position article on mammography screening addresses uncertainties in the evidence base surrounding benefits and harms, and offers specific screening recommendations by age and resource setting, ranging from clinical breast examination to organized, biennial, population-based, mammography screening programs, when the necessary health system requirements exist and in the context of shared decision making. 4 Many countries have created national policies and guidelines for how to implement recommendations for breast and cervical cancer screening specific to their populations, 6 and many countries are taking steps toward establishing nationwide organized screening for cervical and breast cancers. 7
The WHO 2013 Comprehensive Global Monitoring Framework includes 25 indicators that countries can use to monitor their implementation of national strategies to prevent and control noncommunicable diseases (NCDs). 8 The most applicable indicator in the framework assesses the proportion of women screened for cervical cancer. Other nonscreening breast and cervical cancer indicators include the availability of the vaccine against HPV; availability of cancer medicines, technologies, and palliative care; proportion of premature deaths from cancer; and cancer incidence by type. The 17 UN sustainable development goals (SDG) (also known as Transforming Our World: The 2030 Agenda for Sustainable Development) represent a global commitment to transform our world in the areas of poverty reduction, prosperity, and health; the focus of SDG 3 is the assurance of health and well-being across the lifespan, with 13 specific targets. 9 The most relevant targets for cervical and breast cancer control address access to essential health services, including medicines and vaccines, and a one-third reduction in premature deaths from NCDs by 2030.
High-quality behavioral and risk factor surveillance data are necessary to guide and evaluate national cancer control programs and early detection efforts; however, these data are not yet available in many countries. Population-based surveys can collect this information in a standardized comparable manner; however, standardized and cognitively tested questions about cervical and breast cancers are not currently available. Examples of survey tools that can be used to assess behaviors and risk factors for cancer include the WHO STEPwise approach to NCD risk factor surveillance (STEPS) and the Demographic and Health Surveys (DHS) Program, supported by the U.S. Agency for International Development (USAID). 10,11
More than 300 DHS surveys have been completed in 90 low- or middle-income countries since 1985, with the goal of compiling nationally representative data about indicators relevant to local population, health, and nutrition for use in policy and program planning, implementation, and evaluation 11 (Fig. 1). The DHS Program supports population-based surveys covering topics, such as maternal and child health, HIV/AIDS, malaria, nutrition, women's empowerment, fertility, and family planning. The program is funded by USAID and other partners and implemented by each country with technical assistance provided by ICF International. The DHS supports countries with standard methodologies, manuals, and procedures for data collection, including standard model survey questionnaires on population, nutrition, and health, and specific indicator surveys on HIV/AIDS and malaria. Data collection tools are tailored to fit the specific monitoring and evaluation needs of each country.
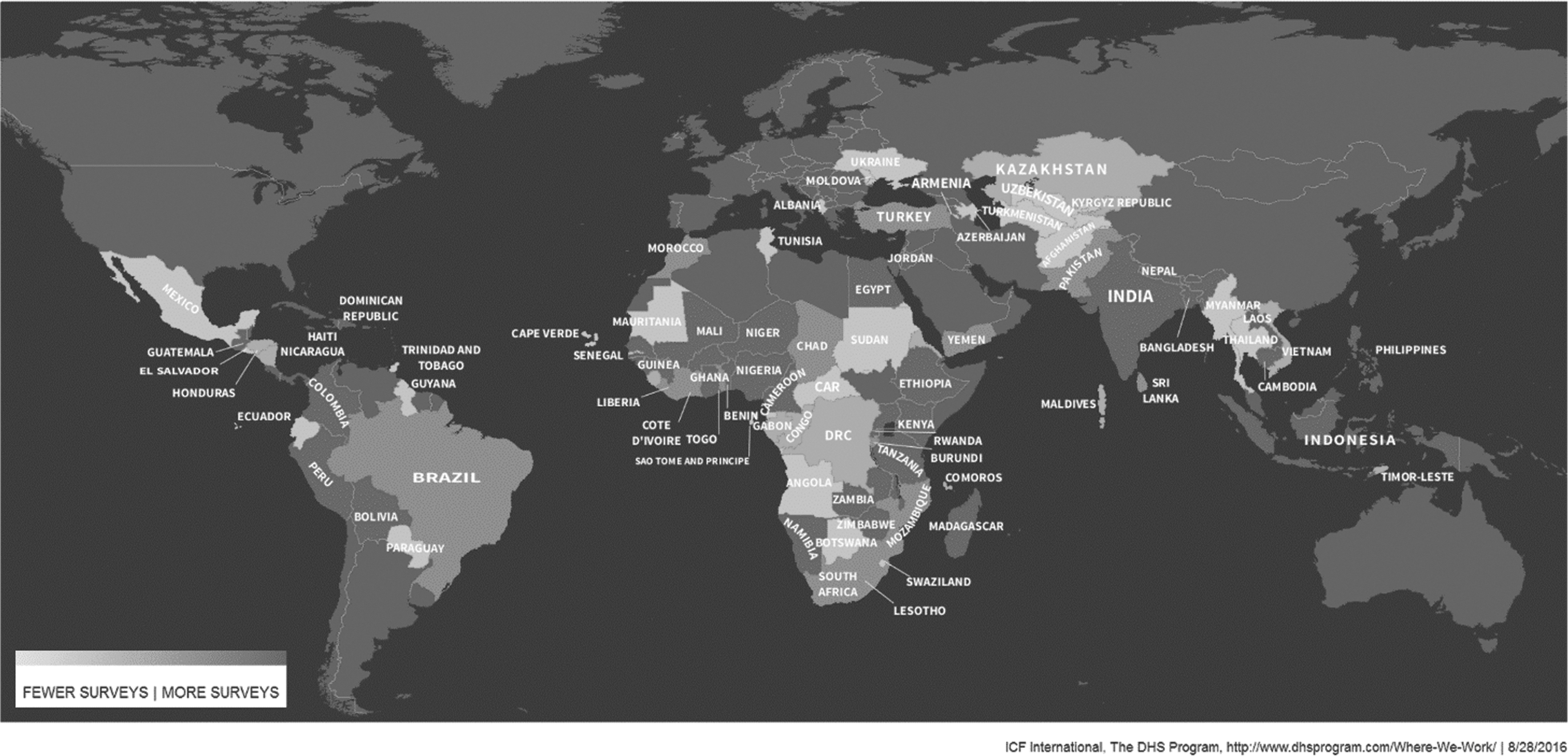
Countries that have conducted one or more Demographic and Health Surveys, 1984–2015.
Materials and Methods
Two independent reviewers searched the DHS Program website by using the keywords breast cancer screening and cervical cancer screening to identify surveys that included these topics between the start of the DHS Program in 1984 and November 2015. Any differences in categorization were resolved collectively. Survey questionnaires were publicly available as final reports published on the DHS Program's website. We downloaded the relevant surveys in English, French, Spanish, and Portuguese and carefully reviewed the sections on NCDs, healthcare utilization, and women's health. The questionnaires were also searched by relevant keywords; the English search included the terms cancer, screening, cervix, vaginal, gynecologist, Papanicolau (Pap), Pap smear, mammogram, and breast. The questions related to cervical and breast cancers were extracted and translated into English if appropriate. They were grouped by themes of disease knowledge, screening knowledge, screening practice, and screening outcomes (Appendix 1). Descriptive statistics were compiled in an Excel worksheet to facilitate the quantitative and qualitative analyses of the data.
Results
Of the 90 countries where DHS surveys have been implemented, cervical cancer screening questions were included in 22 countries (24.4%) and breast cancer screening questions in 18 countries (20.0%) (Fig. 2). The DHS Program website search returned 38 surveys from 22 different countries conducted during 1985–2015 with questions related to cervical and breast cancer screening; 10 countries conducted more than 1 survey during this period (Appendix Table 1). Most of the surveys (30 of 38) asked about both cervical and breast cancers from 18 of 22 countries; 1 survey asked about only breast cancer; and 7 surveys asked just about cervical cancer from 6 of 22 different countries. In other words, nearly all (37 of 38) of these surveys included questions about cervical cancer from all 22 countries, and 31 of 38 surveys included questions about breast cancer from 18 of 22 countries.

Questions about cervical and breast cancer screening in the Demographic and Health Surveys, 1984–2015.
Of those 38 surveys, 32 of the survey questionnaires were available to download from the website from 18 of the 22 different countries. Of the 32 available surveys, 25 of 32 asked about both cervical and breast cancers from 15 of 18 countries; 6 of 32 queried only cervical cancer from 5 of 18 countries; and 1 of 32 asked about only breast cancer from 1 of 18 countries. In other words, nearly all (31 of 32) of these surveys included questions about cervical cancer from all 18 countries, and 26 of 32 surveys included questions about breast cancer from 16 of 18 countries.
Knowledge and awareness of cervical cancer disease were assessed in 8 of the 18 countries with surveys available for review (44.4%), and knowledge and awareness of cervical cancer screening were assessed in 6 of 18 different countries (33.3%) (Fig. 3). Three of the 16 countries with surveys available for review (18.8%) asked about knowledge and awareness of breast cancer disease, and 7 countries (43.8%) asked about awareness and knowledge of breast cancer screening.
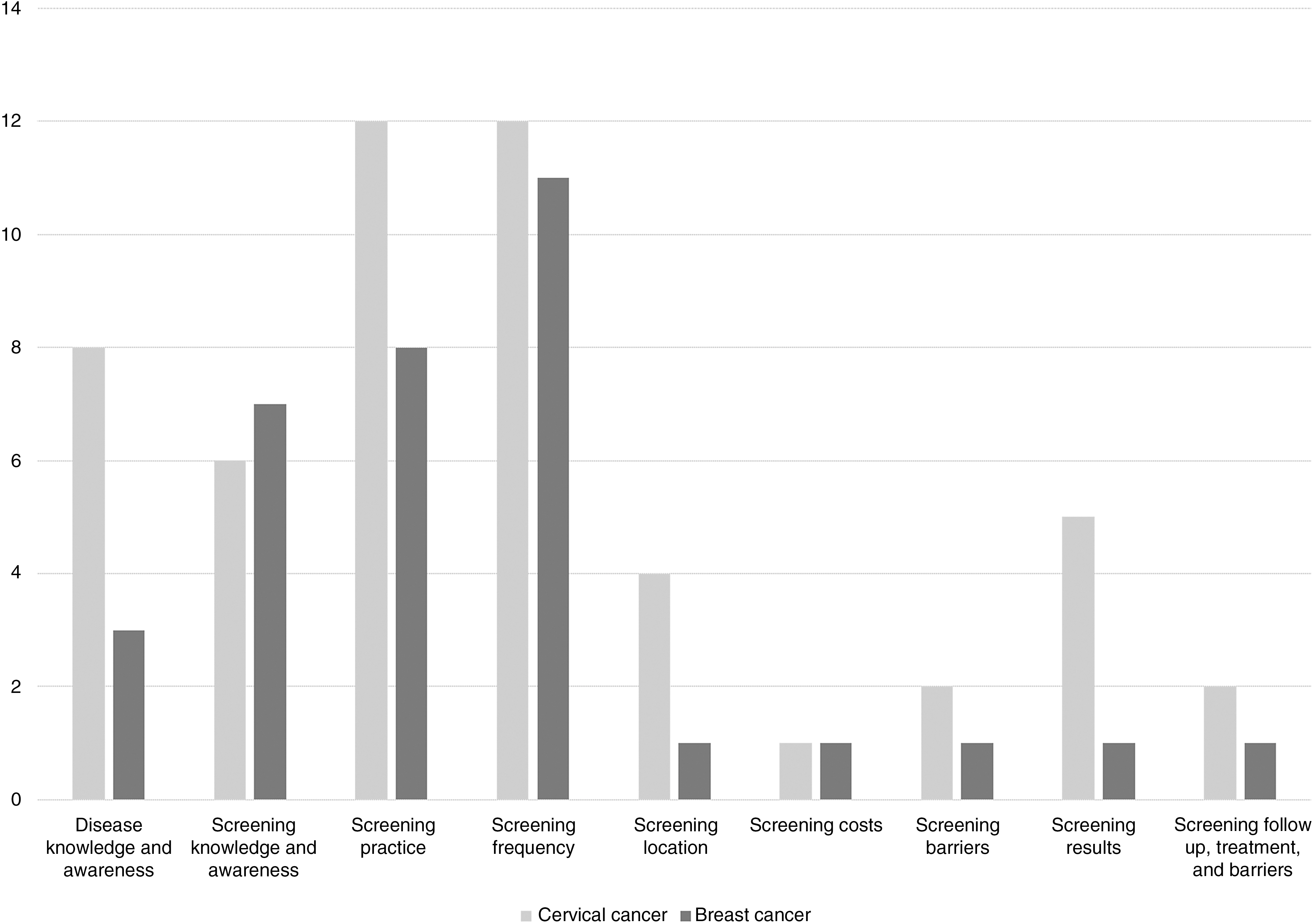
Number of countries that include breast and cervical cancer screening questions in their Demographic and Health Surveys by theme.
A history of screening for cervical cancer by using any modality, including general questions as well as those that specified Pap, cytology, or visual inspection methods, was asked in 12 of 18 countries (66.7%). The timing and frequency of this testing were assessed in 12 countries (66.7%). Four countries (22.2%) asked about cervical cancer screening location (i.e., clinic, hospital, private doctor), one country (5.6%) asked about cost, and two countries (11.1%) asked about barriers to screening. Eight countries (50.0%) assessed a history of screening for breast cancer, including mammography, clinical, and self-breast examination, and 11 countries (68.8%) asked questions about the timing of this screening. One country (6.3%) asked about location, cost, and barriers to screening. Five countries (27.8%) asked about receipt of results, and two of those countries (Bolivia and Colombia, 11.1%) assessed follow-up examinations, treatment, and barriers to treatment following cervical cancer screening. One country (Colombia, 6.3%) asked about receipt of results, follow-up examinations, barriers to follow-up, treatment, and barriers to treatment after breast cancer screening.
Cervical and breast cancer questions have been incorporated into relatively few DHS surveys, but their absolute inclusion has increased since 1984 (Fig. 4). Countries asked a wide range of questions to capture information about disease and screening knowledge, practices, or outcomes. The most frequently assessed topics were whether the respondent had been screened for breast or cervical cancer and the timing or frequency of this screening. Relatively few countries asked specific questions about knowledge of disease and screening, and fewer assessed receipt of screening results, follow-up, and barriers.

Breast and cervical cancer screening questions in the Demographic and Health Surveys, survey count by year.
Discussion
To guide national efforts to reduce the effects of cancers, surveys need to provide specific and measurable information about both the quantity and the quality of cancer screenings. More than half of the countries that asked cancer screening questions did include the core information to enable countries to document the prevalence of breast and cervical cancer screening. However, questions about follow-up and treatment of screened women were rare and missing a component of the screening process that is necessary to achieve reductions in cancer incidence and mortality. Very few surveys have incorporated these essential questions, which will enable countries to evaluate the effectiveness of their cancer screening practices beyond estimates of the proportion of eligible women screened.
On the basis of WHO global screening recommendations, countries that have determined their national cancer prevention and control priorities need specific information to evaluate the success of their interventions. Several DHS questionnaires in their current form provide information to assess the existence of breast or cervical cancer screening. Expansion of these questions by using the more comprehensive questionnaires as a model to include relevant knowledge, barriers, and follow-up could guide efforts to reduce the global burden of breast and cervical cancers.
A recent evaluation of the measurement of NCDs, including cancer, concluded that the DHS Program does collect useful information about NCDs. 12 This year, DHS has made available to countries an optional NCD module with questions about overall cancer diagnoses as well as questions specific to cervical cancer screening. In addition, the WHO STEPS surveys currently include one question asking participants if they have ever been screened for cervical cancer. 10 However, a prerequisite to the expansion of cancer screening data collection is careful evaluation of the relative utility of the data in terms of the increased costs. Collection of NCD data by the DHS may be more relevant among middle-income countries when compared with low-income countries. 12 Of the 22 countries that asked questions about breast and cervical cancer screening in the DHS Program, most (19 of 22) are in the 2017 fiscal year World Bank middle-income categories. 13 Middle-income countries may have more resources compared with low-income countries for implementing and monitoring screening programs. This disparity may explain the increased interest in cancer screening information and more comprehensive questionnaires in some of these middle-income countries, which could also provide guidance for standardized survey questions for the developing world. However, many low-income countries with high HIV prevalence also have initiated cervical cancer screening pilots, so this may be of interest to low-income countries as well.
The ability to assess the existence of cancer screening aligns with the most relevant WHO monitoring framework indicator—the proportion of eligible women screened for cervical cancer. The WHO framework does not include indicators for breast cancer screening. The DHS surveys included in this review did not address the other WHO framework cancer indicators of availability of oncology medicines, treatment, palliation, incidence, and mortality. Cancer incidence and mortality may require the use of vital statistics systems, cancer registries, or other surveillance systems that monitor clinical care. There is a standard way to conduct vaccine coverage surveys, which several low- and middle-income countries are launching as part of their national immunization programs. 14 HPV vaccine coverage is an essential piece of the cervical cancer prevention and control continuum, and countries that have implemented HPV vaccination can track this information at the country level.
The three common themes identified in this analysis (knowledge, practice, and outcomes) could guide the creation of a standard survey tool to be incorporated into future population-based surveys. Such guidance would augment dissemination and comparability of population-level information about cervical and breast cancer screening, which would favor public health research at the global level and enable the monitoring and evaluation of national cancer control policies and programs, with the ultimate goal of reducing the burden of these cancers among low- and middle-income countries.
In response to the need for standardized cervical cancer survey questions, the CDC Foundation, in partnership with CDC, the George W. Bush Institute, and WHO, developed globally endorsed, population-based survey modules as part of the Improving Data for Decision Making in Global Cervical Cancer Programs (IDCCP) Toolkit, scheduled for global dissemination in 2017. 15 The IDCCP Toolkit seeks to improve and accelerate the availability of data for cervical cancer program planning, monitoring, and evaluation. The population-based survey component of the Toolkit includes a core set of questions measuring cervical cancer screening coverage, screening interval, and follow-up and treatment of precancer, as well as an expanded module measuring knowledge and awareness, barriers and facilitators, screening location, single-visit approach, and HPV vaccination. To our knowledge, a similar initiative to create a tool kit to guide breast cancer screening has not yet been undertaken. Given the high burden of breast and cervical cancers among low- and middle-income countries, these initiatives are timely and critical.
Footnotes
Acknowledgment
The authors would like to thank Fred Arnold, PhD, of The Demographic and Health Surveys Program.
Novelty and Impact
In the context of a strong global commitment to reducing the high burden of cervical and breast cancers among low- and middle-income countries, strategies to improve screening are critical. This study identified gaps in the collection of screening data from population-based surveys of breast and cervical cancer and identified themes that need to be included in a standardized survey tool to guide cancer control efforts in a comparable and effective manner.
Disclaimer
The findings and conclusions in this report are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention.
Author Disclosure Statement
No competing financial interests exist.