
Abstract
Background:
Women are disproportionately affected by both obesity and food insecurity. Food insecurity occurs when there is limited ability to acquire adequate foods. It is unknown whether social support can reduce the effect of food insecurity on increased obesity. This study seeks to determine whether social support modifies the relationship between food insecurity and obesity.
Methods:
We conducted a cross-sectional study in a nationally representative sample of 4672 women aged ≥40 years using National Health and Nutrition Examination Survey (2003–2008). Individual food insecurity was assessed based on the U.S. Department of Agriculture 18-item validated household food security scale. Women were categorized as fully food secure (0 affirmative responses) or food insecure (1–10 affirmative responses). Obesity was defined as body mass index ≥30 kg/m2. Outcomes were analyzed by multivariable logistic regression.
Results:
Fourteen percent were food insecure. Women with food insecurity had 1.4 the odds of obesity as those who were fully food secure, adjusting for race/ethnicity and health status (95% confidence interval [CI] 1.22–1.62). Food-insecure women were 80% less likely to report strong social support than women who were fully food secure (95% CI 0.11–0.36). Social support as measured in this study did not modify the association between food insecurity and obesity.
Conclusions:
Women reporting food insecurity reported lower levels of social support and were more likely to experience obesity. Interventions to reduce obesity in women who are food insecure must consider the limited resources available to these women.
Introduction
O
The prevalence of household food insecurity is 14% in the United States. 3 Food insecurity occurs when there is limited or uncertain availability of foods that are both safe and nutritiously adequate, or when there is an uncertain ability to acquire such foods in socially acceptable ways. 3,4 Food insecurity disproportionately affects special populations. For single-women-led households with children, the prevalence is 38%. Twenty-six percent of non-Hispanic black-led households and 22% of Hispanic-led households experience food insecurity. 3 Food insecurity is associated with many negative health outcomes such as insulin resistance, diabetes, and physical and mental health. 5 –12 As with food insecurity, obesity also disproportionately affects women, non-Hispanic black, and Hispanic women in the United States. 1
Food insecurity has been shown to be associated with higher body mass index (BMI) in adults. 13 –17 Although results for men have been mixed, the relationship between overweight and obesity and food insecurity in women is consistent. 17,18 Obesity is a diet-related disease that is attributed not only to excess energy intake but also to poor quality food patterns that include highly processed foods. 19 These processed, nutrient-poor foods may be easier to access and more affordable than high-quality foods. 19,20 Theory-based weight loss interventions commonly include components to increase social support. 21
It is unknown whether social support modifies the association of food insecurity on obesity. Strong social support may represent a range and depth of resources needed to maintain multiple health behaviors to prevent obesity. Having little emotional or material support may discourage someone from taking the time to shop for healthier, more affordable options, which requires preparation and some skill. Having a strong social support system may provide a “safety net” that includes someone to turn to for financial support, which could help women have greater access to healthier foods. Social support has been positively correlated with obesity and diabetes. 22 Longitudinal data also suggest that strong social support can have a protective effect on BMI in offspring of parents with high BMI. 23
In diabetes research, social support has been shown to influence health behaviors and to increase the likelihood of patients being aware of having a diabetes diagnosis in low-income adults, potentially allowing for better care of patients. 24 Social support has also been linked to improved diabetes self-care behaviors. 25 Obesity is also a risk factor for cardiovascular disease and low social support is associated with increased risk of negative outcomes for cardiovascular disease. 26 Although a promising idea, whether the untoward effects of food insecurity on obesity can be diminished by social support has yet to be explored.
The goal of this study is to determine to what extent social support modifies the association between food insecurity and obesity in women. We focus on women for two reasons. First, women are disproportionality affected by food insecurity and obesity. Second, the relationship between food insecurity and obesity has been consistently observed in women. 17,18 We hypothesize that food insecurity will have a weaker association with obesity in women with high social support than in women with low social support.
Materials and Methods
An analysis was performed on participants of the National Health and Nutrition Examination Survey (NHANES) waves 2003–2004, 2005–2006, and 2007–2008. This is a nationally representative survey of a community-dwelling population of the United States. NHANES is administered annually through a household interview in conjunction with a physical examination from a Mobile Exam Center (MEC). 27 All participants provided written informed consent. 28 The University of Massachusetts Medical School Institutional Review Board determined that this study did not require their oversight because analyses included only publically available deidentified data.
Analytic sample
Women were included if they were ≥40 years of age because the social support questionnaire was administered to these women for the NHANES cycles examined. 29 We included women with BMI available in the data set (n = 4879). Underweight women (<18.5 kg/m2) (n = 71) were excluded because there were not enough participants to maintain a separate underweight category in the analysis. Women were excluded if there were missing data on adult household food security (n = 89), marital status (n = 1), number of friends (n = 19), education level (n = 7), smoking status (n = 2), and general health (n = 5), or they did not report scores for emotional support or financial support (n = 7). Women who were pregnant at time of interview were not included (n = 6). This resulted in an analytic sample of 4672 participants (weighted n = 64,804,362).
Outcome measurement
We selected obesity as the primary outcome of interest because we were intrigued by the food insecurity–obesity paradox. Height and weight were directly measured according to standardized protocols at the MEC. We classified women according to their BMI as normal weight (18.5–24.99 kg/m2), overweight (25–29.9 kg/m2), and obese (≥30 kg/m2). 2 We created a dichotomous variable using the cutoff for obesity (≥30 kg/m2) for three reasons. First, the guidelines for management of obesity recommend weight loss for BMI ≥30 kg/m2. 2 Second, we did so to allow for comparisons with previous literature on this topic. 30 Lastly, collapsing BMI in this way maintained the minimum observations needed per NHANES analytic guidelines. 27
Determinant: food insecurity
The NHANES adult food security measure is based on the validated 18-point household level scale developed by the U.S. Department of Agriculture. 3 The adult food security scale is an ordinal scale based on affirmative answers to 10 questions addressing anxiety about, access to, and quality and quantity of food. Participants were administered the food security module during the MEC phase of the study. Preliminary analyses included three categories of food insecurity as fully food secure (0 responses), marginal food security (1–2 responses), and low/very low food security (3–10). Based on these analyses, we determined that food-insecure categories should be collapsed further to maintain the minimum counts per cells recommended by NHANES. 27 We categorized women as fully food secure (0 responses) and food insecure (1–10 affirmative responses).
Effect measure modifier: social support
Social support was measured as an index based on four domains: (1) emotional support, (2) material support, (3) marital status, and (4) size of network. Emotional support was measured by asking respondents “Can you count on anyone to provide you with emotional support such as talking over problems or helping you make a difficult decision?” (Yes/No). For material support, respondents were asked “If you need some extra help financially, could you count on anyone to help you; for example, by paying any bills, housing costs, hospital visits, or providing you with food or clothes?” (Yes/No). Marital status was categorized as “yes” for self-report of currently married or living with a partner and “no” for widowed, divorced, or single. 31 Network size was measured by the number of close friends and was dichotomized using a median split (≥5 friends and <5 friends).
Each of the previous four components was assigned a point if answered “yes.” The four components were then summed to create the social support index, consistent with prior research. 25 The social support index was categorized as 0–2 as low support, 3 as moderate support, and 4 as strong social support. To maintain cell size for analysis, the social support category was collapsed to low support (0–2) and high/moderate social support (3–4).
Confounders
Potential confounders were chosen based on their known associations with food insecurity and obesity and not social support per methods described for studies evaluating effect measure modification. 32 Age, race/ethnicity, education, health status, access to routine care, household size, 33 and smoking status were considered to be potential confounders. Age was divided into three categories (40–54, 55–64, and ≥65 years). Race/ethnicity was defined as non-Hispanic white, non-Hispanic black, and other (includes Mexican Americans, other Hispanic origin, and multiracial); non-Mexican Hispanics and Mexican Americans were not analyzed separately due to differences in sampling methods across NHANES waves analyzed. 34 Education was defined by four categories: less than high school, general education diploma or high school diploma, associate's degree or some college, and bachelor's degree or more. Poverty-to-income ratio was defined as <1.35, 1.35–1.85, or >1.85 to line up with eligibility for relief programs. Participants were asked to describe their general health, which was dichotomized to 1 if excellent/very good/good or to 0 if fair/poor. Participants were asked whether they had a routine place to go for healthcare. Routine access to care was categorized as 1 if they responded yes to at least one place or 0 if they had no routine place to access care. Household size ranged from 1 to 7 (7 represented ≥7 household members). Household size was categorized as lives alone, lives with one other person, or lives with two or more people. Participants smoking status was categorized as current smoker if they have smoked at least 100 cigarettes in their life and reported currently smoking cigarettes every day or some days. They were defined as former smokers if they smoked at least 100 cigarettes in their life but did not currently report smoking, or responded do not know or refused. Participants were categorized as never smokers if they responded “no” to ever smoking 100 cigarettes.
Statistical analysis
Sample weights for the examination phase of the survey were used according to NHANES analytic guidelines and analyses were weighted to represent middle-aged and older U.S. women. 35 The percentage of participant characteristics was reported by food security level. Frequency of individual social support components was reported by food insecurity level.
For the main effects of food insecurity on obesity, a logistic model was developed to adjust for confounders. The logistic model included the main outcome, obesity, with food insecurity as the main determinant. We forced race/ethnicity and current health status into the model, but other covariates were evaluated using the change in estimate method to determine which characteristics changed the crude estimate by 10% or more. 36 The following characteristics were evaluated for change in estimate: age, education level, household size, access to routine place of care, and smoking status. Adjusted odds ratios (aOR) and 95% confidence intervals (CIs) were reported. We conducted a formal analysis for effect measure modification of social support by evaluating departures from additivity. 32 We used this approach (e.g., testing for departures from additivity) because it can be useful for identifying subpopulations for intervention targeting. Stratified logistic regression was also performed to evaluate the association between food insecurity and obesity within each strata of social support, adjusted for health status. A separate logistic regression model was developed to estimate the association between food insecurity and social support, adjusting for race/ethnicity, education, and age. We also explored the components of the social support index individually.
Results
Among women, 14% were food insecure. The average age of food-insecure women was 54.6 years and the average age of food-secure women was 58.0 years. Among food-insecure women, 51.9% reported their race/ethnicity as non-Hispanic white; among food-secure women, 79.4% were non-Hispanic white. Of the women experiencing food insecurity, 7.6% reported having at least a bachelor's degree, whereas 26.6% of women reporting food security attained at least a bachelor's degree. Forty-four percent of women experiencing food insecurity and 18.3% of food-secure women reported their current health status as poor or fair. The majority of women reporting some level of food insecurity had low social support, whereas the majority of fully food-secure women reported mid to high social support (Table 1).
All values are weighted to represent nonpregnant women of ages ≥40. Data are from NHANES 2003–2004, 2005–2006, and 2007–2008.
Percentages may not total 100% due to rounding.
There were 408 participants missing poverty income ratio.
NHANES, National Health and Nutrition Examination Survey.
Women with any reported level of food insecurity were 80% less likely to have a social support index ≥3 than their food-secure counterparts (OR 0.20; 95% CI 0.11–0.36). Individual components of the social support index did not achieve statistical significance. The odds of obesity were 1.70 (95% CI 1.50–2.01) times higher in women with food insecurity than in food-secure women (Table 2). Adjusting for race/ethnicity and health status, the estimate was attenuated (aOR 1.41; 95% CI 1.22–1.62).
All values are weighted to represent nonpregnant women of ages ≥40. Data are from NHANES 2003–2004, 2005–2006, and 2007–2008.
Adjusted for race/ethnicity and health status, women who were food insecure had 1.41 times the odds of obesity relative to women who were food secure.
Figure 1 shows the unadjusted prevalence of obesity in food-secure and food-insecure women stratified by social support. The prevalence of obesity was higher among food-insecure women than among those who were food secure, and this relationship was similar by level of social support. Stratified analysis of social support levels showed similar associations between food insecurity and obesity for both women with moderate/high social support and women reporting low social support, adjusting for health status (Table 3). Among women reporting high or moderate social support, 8% reported food insecurity. Within moderate/high social support, food-insecure women were 1.60 (95% CI 1.25–1.99) times as likely to be obese compared with food-secure women, adjusting for perceived health status. Among women reporting low social support, 29% reported food insecurity. Within the strata of women with low social support, the prevalence of obesity was higher among food-insecure women relative to food-secure women (aOR 1.50; 95% CI 1.21–1.91). The formal analysis for effect measure modification of food insecurity and social support failed to reveal departures from additivity.
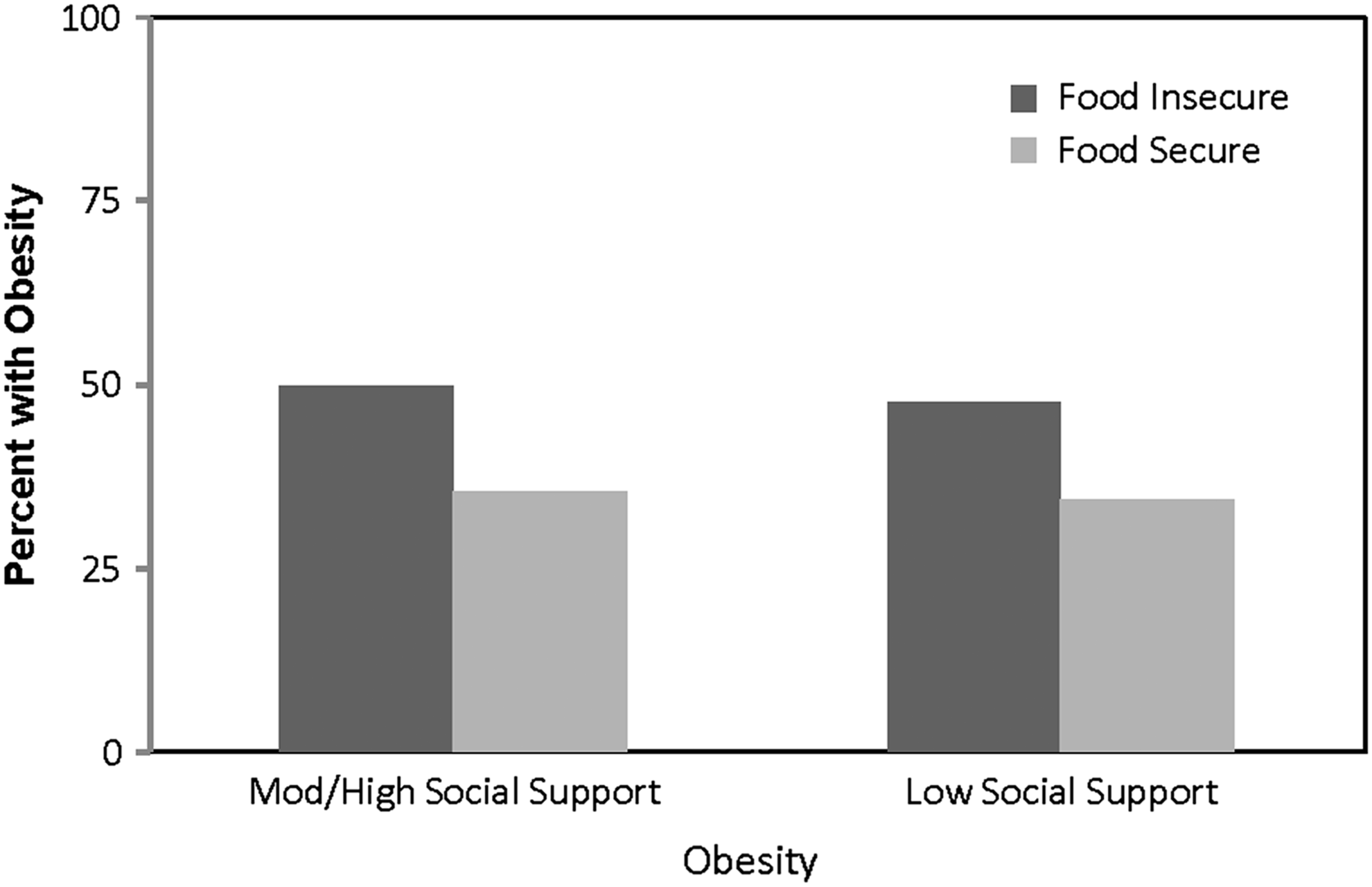
Prevalence of obesity in women aged ≥40 years by food security status and social support. Dark gray represents obesity among food insecure; light gray represents obesity among food secure. Obesity = BMI ≥30 kg/m2. All values are weighted to represent nonpregnant women of ages ≥40. Data are from NHANES 2003–2004, 2005–2006, and 2007–2008. Prevalence represents unadjusted estimates. BMI, body mass index.
All values are weighted to represent nonpregnant women of ages ≥40. Data are from NHANES 2003–2004, 2005–2006, and 2007–2008.
Adjusted for health status, food-insecure women with high social support were 1.58 times as likely to be obese than food-secure women. For women with low social support, the adjusted odds ratio was 1.52.
Discussion
We found that food insecurity occurred in 14% of U.S. women at least 40 years of age. Women experiencing food insecurity were disproportionately poor, racial/ethnic minority, less educated, and of fair or poor health relative to food-secure women. Women experiencing food insecurity were less likely to have strong social support relative to food-secure women. The prevalence of obesity was greater in food-insecure women relative to food-secure women. We hypothesized that social support would diminish the adverse effect of food insecurity on obesity. Contrary to our hypothesis, the level of social support as defined by the instrument used in this study did not modify the association between food security status and obesity prevalence.
Our findings regarding the prevalence of food insecurity and which women experience food insecurity are consistent with the literature. Overall in the United States, the prevalence of household food insecurity is 14% 3 and this matches our estimate in women at least 40 years of age. Furthermore, the characteristics among food-insecure women in our study are similar to what has been reported in other nationally representative studies with regard to age, education, and race/ethnicity and income and obesity. 5,30,37
This study adds to the literature by describing the level and type of social support available to women experiencing food insecurity. We found that women experiencing food insecurity were much less likely to experience strong social support of all four indicators, availability of emotional and financial support, marriage or living with a partner, and a large network of friends. Food insecurity in adulthood has been linked to adverse childhood experiences 38 and depression, 39 both of which can impact adult social support. Our data, however, are cross-sectional in nature and as such we could not differentiate whether poor social support was an antecedent or a consequence of food insecurity. However, recent qualitative research on household food insecurity revealed that food insecurity often occurs across the lifespan and may cross generations. 40 We also found that food insecurity was associated with increased prevalence of obesity, which adds to the consistent literature on this association in women. 17,18
In general, social support has been found to be positively associated with health behaviors. 25,41 –43 In older Americans, unmarried adults were less likely to engage in moderate physical activity relative to those who were married, whereas those having ≥5 friends or emotional support was associated with being more likely to engage in moderate physical activity. 42 Results on the role of social support are mixed with regard to BMI. 22,23,44,45 In a population of African American women in the rural South, participants reported limited social support from family and friends for eating and physical activity behaviors that was not associated with obesity, 44 although the choice of obesity cut points used in the study may have diluted the effect. 44 In a cross-sectional study, there was no association between strength of social support and obesity, although obese participants were more likely to report food insecurity. 45
In a longitudinal analysis of middle-aged adults, social support was found to be protective of overweight. 23 Detection of a protective role of social support may be due to the longitudinal study design and the use of a detailed perceived social support scale that captured the quality of relationships. 46 This study focused on BMI as the primary end point. Although our data did not support the role of social support as a modifier of the association between food insecurity and BMI, social support may modify the association between food insecurity and the more proximal measures of dietary intake and physical activity, which are associated with BMI. A recent review suggested that social networks may interact to influence weight behaviors in three ways: (1) people can be influenced by the networks that they are already integrated into, (2) their weight may influence how they choose their network, and (3) a sense of support and belonging to a network influences behavior. 47 The data available for this study did not permit a more in-depth understanding of the role of social support and obesity.
Although we expected to see a higher prevalence of obesity among those experiencing food insecurity and low levels of social support, obesity was common across all levels of social support measured. Social support did not modify obesity prevalence in our study. This suggests that the cumulative resources of having emotional and financial support, being married or living with a partner, and having a large network of friends were not protective for either food-secure or food-insecure women at the time of this study. In a study on hypertension, similar indicators of emotional support, financial support and marriage, and social support were found to moderate the impact of race on hypertension. 41 That we did not show an association could be due to obesity representing cumulative effects of negative behaviors, whereas the social support and food insecurity questions are more reflective of participants' current situation. For example, in the hypertension study, the outcome was measured either by participants having an antihypertension prescription or current blood pressure reading, thus strengthening the interaction of social support and race on an immediate rather than cumulative outcome. 41 We were also unable to determine the positive or negative nature of current social support. 48 This may have diluted the impact of social support on the relationship between food insecurity and obesity prevalence.
The implications of our study findings for weight loss interventions are noteworthy. First, integrating screening for food insecurity is important as food insecurity has been shown to be associated with increases in BMI over time. 49 Given that food insecurity may be a marker of prolonged (and potentially intergenerational) disadvantage, 40 interventions with women experiencing food insecurity should emphasize the need to access information beyond regular sources to begin to break behavioral patterns that may lead to obesity. The paradox of obesity and food insecurity may be due to consuming calorie-dense, nutrient-poor foods, 50 or lack of physical activity. Future research should consider diet and physical activity to further our understanding of the impact of food insecurity and social support.
Second, understanding more about how to address the needs of this vulnerable population is essential. The importance of social networks in the spread of the obesity epidemic has been demonstrated, 51 and reinforces the role of social networks and social support in addressing this public health issue. Despite the importance of social support and social ties in weight loss, a recent systematic review 52 concluded that the role of social ties appeared to be “conceptually ancillary” to most weight loss interventions. That persons experiencing food insecurity lack social support must be considered in the design of weight loss interventions in this vulnerable population. Furthermore, in a mixed-method study that sought to understand how participants maintained healthy weight in the face of food insecurity challenges using a positive deviance approach, participants suggested that skill-building interventions targeting the individual should focus on budgeting, cooking techniques, and portion control. 49 Third, innovative research and programs are needed that address the needs of food insecurity in their community. A recent pilot intervention focused on delivering diabetes-appropriate foods, screenings, and primary care physician referrals through local food banks. 53 Community level programs that may reduce economic barriers to health food choices show promise. 54 Furthermore, tailored community-based interventions using social–ecological approaches have been successful. 55
Strengths and limitations
Our study offers many strengths. First, this study was conducted in a nationally representative sample allowing for generalizability to U.S. women ≥40 years of age. We replicated expected prevalence of food insecurity and obesity, thus strengthened the validity of the findings. Second, the study used actual measured height and weight, which offers advantages to other studies that relied on self-reported data. Furthermore, the outcome measurement cutoff of BMI ≥30 kg/m2 is associated with established increased risks of cardiovascular disease and mortality and has lower rates of misclassification than overweight. 56 Lastly, NHANES included measures of individual food insecurity. Typically, food insecurity is measured at the household level and may not coincide with current individual measures of health. The concurrent measurement of individual food insecurity and actual BMI provides important contextual information on experiences of women with obesity who may benefit from weight management counseling.
Some limitations must be considered when considering the study findings. The data are cross-sectional and as such prevent the determination of causal relationships. We also recognize that BMI is one component of health and does not capture overall metabolic profiles. Women may have metabolically unhealthy profiles but normal BMI and vice versa. BMI was selected rather than dietary intake because we were interested in focusing on a measure closer to conditions and diseases further along the causal pathway (e.g., cardiovascular disease and osteoarthrtitis). Although social support did not modify the association between food insecurity and BMI, we recognize that lack of social support may increase difficulty in making optimal diet choices. As such, future research should explore the extent to which food insecurity is associated with diet and whether social support modifies any observed association. We caution against generalizing the findings observed in women to men. We excluded men from this study because the evaluation of three-way moderation is unwieldy and not easily interpretable. We believe a separate study focusing on this issue in men would be worthwhile. Because women <40 years were not asked key questions regarding social support, they were excluded from the analysis. As such, the findings must not be extrapolated to women of younger ages. It may well be that social support does modify the association between food insecurity and obesity, but the particular measure used in this study does not adequately capture the concept of social support. The social support index could be strengthened in future studies by incorporating frequency of social contact with friends, community organizations, and church attendance. Frequency of church attendance is protective of chronic diseases and this relationship is especially strong in women. 57 More importantly, future research should include measures of social support specifically associated with the behavior change under study, rather than generic social support measures available in this study.
Conclusion
In the United States, obesity is highly prevalent among women ≥40 years of age, and among women reporting food insecurity, a population that reports low social support, the prevalence of obesity is nearly 50%. It is important to take into account the limited resources of food-insecure women who would benefit from weight loss intervention.
Footnotes
Author Disclosure Statement
No competing financial interests exist.