
Abstract
Background:
A novel formulation of secnidazole is under development in the United States for the treatment of bacterial vaginosis (BV). Efficacy and safety of other formulations of secnidazole have been reported. The objective of this study is to evaluate the safety of a single-dose oral granule formulation of secnidazole in a U.S. population of women with BV.
Methods:
In this open-label study, patients were enrolled based on the following criteria: off-white, thin, homogeneous vaginal discharge; vaginal pH ≥4.7; presence of ≥20% clue cells; and positive potassium hydroxide whiff test. Eligible patients received a single dose of secnidazole 2 g at baseline. Patients were contacted on days 8–10 and were assessed for safety at an end-of-study visit (days 21–30). Additional endpoints included investigator assessment of the need for additional treatment and a post hoc analysis of clinical response to treatment.
Results:
Of 321 patients, 283 (88.2%) completed the study. The mean age was 32 ± 8.5 years; most patients were white (51.4%) or black/African American (46.1%). Most (79.1%) reported ≤3 episodes of BV in the past year. The overall number of treatment-emergent adverse events (TEAEs) was 95 (29.6%), of which 53 (16.5%) were treatment related. Common treatment-related TEAEs were vulvovaginal mycotic infection (5.3%), nausea (4.4%), and dysgeusia (3.1%). The proportion of patients not requiring additional BV treatment, as assessed by investigators, was 72.5%.
Conclusions:
Single-dose secnidazole 2 g was well tolerated, with a low overall number of TEAEs, most of which were mild to moderate.
Introduction
B
BV is associated with an increased risk of serious health complications, including an approximately twofold increased risk of acquiring sexually transmitted infections (STIs), that is, HIV infection, herpes simplex type 2 infection, 4 and a greater than threefold increased risk of transmitting HIV to male partners. 5 Compared with women without BV, those with BV are 4.1 times more likely to test positive for Neisseria gonorrhoeae and 3.4 times more likely to test positive for genital Chlamydia trachomatis. 6,7 In addition, BV has been associated with increased risk of various negative reproductive health outcomes for both mother and child (i.e., preterm deliveries, low birth weights, and clinical chorioamnionitis). 8 For example, BV is associated with a twofold increase in preterm delivery and a sixfold increase in risk of miscarriage. 9 In addition, BV can impact quality of life, with 60% of recurrent sufferers reporting a negative impact on job-related productivity and 95% reporting a severe restriction in intimate partner relations. 10,11
Current first-line therapeutic regimens recommended by the U.S. Centers for Disease Control and Prevention include metronidazole 500 mg orally twice daily for 7 days; metronidazole gel 0.75% intravaginally once daily for 5 days; or clindamycin cream 2% intravaginally at bedtime for 7 days. 4 Based on comparative studies, the efficacy of oral tinidazole is equivalent to oral metronidazole, intravaginal clindamycin cream, and intravaginal metronidazole gel in treating BV. 12 Despite the availability of these regimens, recurrence rates of 30% have been observed at ∼60–90 days posttreatment, and recurrence risk is known to increase over time (50% at 12 months). 13 Poor adherence to anti-infective therapy increases with length of treatment (7 days twice daily for current standard of BV care) 14 ; studies have demonstrated nonadherence in >50% of patients for a 7-day treatment course. 15
Symptoms of BV are often difficult for patients to distinguish; thus, many do not seek treatment. 3,13 Approximately 75% of BV patients report never noticing vaginal odor, and only 42% report abnormal vaginal discharge. Moreover, 25% of symptomatic women with BV only report having symptoms on direct questioning. 16,17
Poor diagnostic practices are common with vulvovaginal symptoms: 54% of women are treated without adequate diagnostic evaluation, and a previously reported study showed that microscopic confirmation did not support the treatment given in 26% of cases. 18 Sixty percent of symptomatic patients are left untreated; therefore, increased disease awareness among patients is necessary, and could ultimately lead to reduced risk of serious consequences associated with BV. 18
Effective treatment of BV remains an unmet medical need, given the prevalence of this infection, combined with the response/recurrence rates associated with currently available multidose therapies. Secnidazole has been used for the treatment of numerous infectious diseases, but was not submitted for U.S. Food and Drug Administration approval, despite its efficacy, due to the presence of other effective marketed antibiotics (e.g., metronidazole). Single-dose secnidazole 2 g (SOLOSEC™ [secnidazole]; Symbiomix Therapeutics, LLC, Newark, NJ) is an oral granule formulation of secnidazole, a 5-nitroimidazole that is being developed to treat BV in the United States. Secnidazole has been shown to have antimicrobial activity against many bacterial species implicated in BV and, like other 5-nitroimidazoles, has limited activity against lactobacilli, the beneficial microbes that are important in establishing vaginal health after treatment. 19,20 Single-dose secnidazole 2 g is rapidly absorbed and has not been shown to have any drug-drug interactions or interactions with alcohol. It has a longer half-life (t 1/2) than metronidazole (∼17–39 hours vs. ∼8 hours), and it can be administered with or without a meal. 21,22
Previously published clinical studies have demonstrated clinical and microbiological activity of single-dose secnidazole 2 g in the treatment of BV. 23,24 In a phase 3, randomized, double-blinded, multicenter, placebo-controlled study, including women and postmenarchal adolescent girls with BV (N = 189), single-dose secnidazole 2 g was superior to placebo in all primary and secondary efficacy measures. 24 More specifically, the clinical outcome responder rate (primary efficacy endpoint) differed significantly between the secnidazole 2 g- and placebo-treated groups (53.3% vs. 19.3%, respectively). A separate randomized clinical study conducted outside the United States compared a single dose of secnidazole 2 g and metronidazole (N = 577), and it demonstrated comparable cure rates at day 28 (60.1% vs. 59.5%, based on resolution of vaginal discharge, positive potassium hydroxide [KOH] whiff test, vaginal pH >4.5, Nugent score >7) and a comparable safety profile. 25
To date, clinical trials of single-dose secnidazole 2 g have focused on efficacy and safety/tolerability. This is the first safety study in BV for single-dose secnidazole in the United States; the objective is to further evaluate and confirm the safety of single-dose secnidazole 2 g for the treatment of women with BV.
Materials and Methods
Study design
This was a phase 3, multicenter, prospective, open-label study evaluating the safety of single-dose secnidazole 2 g in women with BV. Patients with symptomatic BV were recruited from 34 study sites that enrolled at least one patient based on the inclusion criteria. Patients who were determined to be eligible at the baseline visit (day 1) received single-dose secnidazole 2 g in 4 oz of unsweetened applesauce to be self-administered on day 1 (without regard to meals). Patients were contacted by telephone once between days 8 and 10 to inquire about possible adverse events (AEs). A final end-of-study (EOS) visit was conducted on days 21–30 to assess the patient for safety.
Inclusion criteria
Eligible patients were: nonpregnant adult females or postmenarchal adolescent girls ≥12 years of age with a clinical diagnosis of BV, defined as having all of the following criteria: off-white (milky or gray), thin, homogeneous vaginal discharge, vaginal pH ≥4.7, presence of clue cells ≥20% on microscopic examination of vaginal samples, positive 10% KOH whiff test 17 ; in good general health, as confirmed by a medical history and physical examination; and willing and able to give written informed consent or, if aged <18 years, were willing and able to give written informed consent along with a parent or legal guardian. Patients of childbearing potential were required to use a form of birth control, including oral contraception; implantable, injectable, or transdermal hormonal contraception; intrauterine device; double-barrier methods; have a vasectomized partner; or practice abstinence. NuvaRing® (etonogestrel/ethinyl estradiol vaginal ring) or other vaginal ring products were not permitted. Patients agreed to abstain from alcohol for 3 days after study treatment and not to use vaginal douches for the duration of the study.
Exclusion criteria
Patients were excluded if they had any vaginal bleeding at baseline (day 1) or were menopausal, as determined by the investigator; were suspected clinically (or confirmed diagnostically) of having alternative causes of vaginal symptoms, such as candidiasis or other STIs; had a history of an abnormal Pap smear that required cervical biopsy or cervical cauterization within <3 months of the baseline visit; and had active genital lesions. Concomitant systemic antimicrobial therapies, warfarin, systemic corticosteroids, and immunomodulatory therapies were not permitted during the study. Antifungal therapies to treat intercurrent conditions such as vulvovaginal candidiasis were permitted.
Treatments
Patients received a single-dose secnidazole 2 g orally administered with 4 oz of unsweetened applesauce, followed by 8 oz of water. The study medication was mixed and administered by the study patient on day 1, without regard to meals.
Outcomes/assessments
The following safety outcomes were assessed: treatment-emergent adverse events (TEAEs), serious adverse events (SAEs), and treatment-related TEAEs. Investigators were asked to report the severity and duration of the AE. AEs were recorded verbatim and then categorized by System Organ Class and Preferred Term by using the Medical Dictionary for Regulatory Activities. A TEAE was defined as any AE that occurs after administration of the study drug and through the EOS visit. A treatment-related TEAE was defined as a TEAE possibly or probably related to the study drug, as determined by the investigator. TEAEs were defined as severe if they were incapacitating and resulted in an inability to perform normal activities. Vital signs (blood pressure [BP], temperature, pulse), physical and pelvic examinations, and clinical laboratory assessments were also recorded at baseline and the EOS visit. Blood and urine samples were collected for safety laboratory tests (hematology, chemistry, urinalysis [including pH]) from all patients at the baseline and EOS visits as well. At the EOS visit, investigators were also asked to assess whether additional treatment was needed. A pelvic examination was performed at the EOS visit if the patient reported any vulvovaginal signs/symptoms/AEs. In addition, a pelvic examination could be performed at the investigator's discretion in patients with no vulvovaginal signs/symptoms/AEs at the EOS visit and at any time during the study if the patient's clinical response was perceived to be inadequate or as dictated by patient symptoms.
A post hoc analysis was conducted to determine clinical outcome based on available vaginal assessment data collected at the EOS visit (investigators were not required to collect these data). A clinical outcome responder was defined as a patient with normal vaginal discharge or abnormal discharge inconsistent with BV; negative 10% KOH whiff test; and <20% clue cells, as determined by microscopic examination of a wet-mounted vaginal sample.
Data analysis
Safety evaluations were based on the number, intensity, and type of AEs, and changes in the patients' physical examination findings, vital signs, and clinical safety laboratory results. The frequencies of TEAEs were summarized overall and by System Organ Class and Preferred Term by using frequencies and percentages. The sample size of 325 patients was chosen to provide observational safety data only. No formal sample size calculations were made. Statistical analyses were performed by using SAS® Software Version 9.3 or higher.
For laboratory results and vital sign parameters, changes from baseline to the EOS visit were summarized. In addition, shifts in laboratory parameters and physical examinations from baseline to the EOS visit were summarized. Counts and percentages of patients with ≥1 abnormal vital sign results after baseline, investigator's clinical assessment at EOS visit, and post hoc clinical responder analysis were summarized (Supplementary Table S1; Supplementary Data are available online at
Ethical conduct of the study
This study was approved by multiple institutional review boards (Schulman Associates IRB, Cincinnati, OH; Western IRB, Puyallup, WA; Chesapeake IRB, Columbia, MD), and each subject provided informed consent. This study was designed, monitored, and/or performed in accordance with the ethical principles of the Good Clinical Practice guidelines of the International Conference on Harmonisation. 26
Results
Study patients
A total of 325 patients were enrolled at 34 research centers in the United States. The safety population included 321 patients who received study medication; 4 subjects who did not receive study medication were excluded, due to violation of the study entry criteria. Of the 321 patients in the safety population, 283 (88.2%) completed the study (Fig. 1). Among the 38 patients (11.8%) who discontinued the study prematurely, the most common reason was detection of STIs in baseline vaginal samples (17/283; 5.3%) and lost to follow-up (13/283; 4.0%). Two patients discontinued due to a TEAE (mycotic infection for both patients). Per the prespecified protocol, patients were discontinued from the study because of positive baseline STIs. The majority of the study population was either white (164/321; 51.4%) or black/African American (148/321; 46.1%), and median age was 32 ± 8.5 years (range 15–53 years; Table 1). Most patients (79.1%) reported ≤3 episodes of BV in the past 12 months.
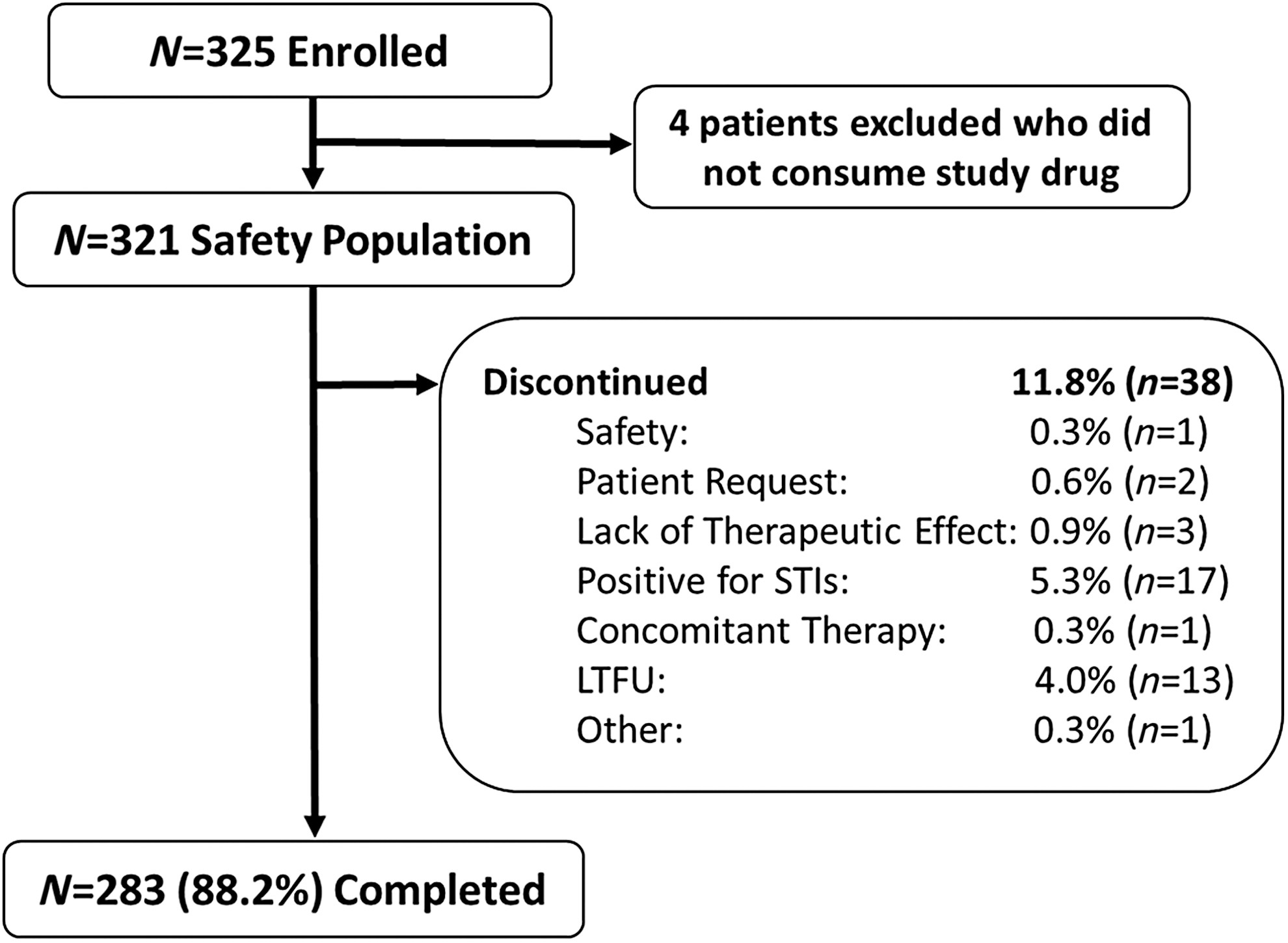
Summary of patient disposition (safety population). LTFU, lost to follow-up; STIs, sexually transmitted infections.
BV, bacterial vaginosis; SD, standard deviation.
Summary of AEs
The majority of TEAEs were mild or moderate. The overall number of TEAEs was 95 (29.6%), and the number of treatment-related TEAEs was 53 (16.5%) (Table 2). The most frequently reported (occurrence ≥2%) were vulvovaginal mycotic infection/candidiasis (17 patients, 17 events, 5.3%), nausea (14 patients, 14 events, 4.4%), and dysgeusia (10 patients, 10 events, 3.1%). Four patients reported eight severe TEAEs, two of which were also considered serious (one unrelated, a wound secondary to a foot burn, and one, loss of consciousness, possibly related to study treatment). There were no deaths reported throughout the study.
Both vulvovaginal mycotic infection and vulvovaginal candidiasis were listed as preferred terms for recording AEs; designation of the term for the AE was at the discretion of the investigator. The terms are listed together in the table as it is likely that all mycotic infections could be attributed to Candida spp.
AE causality was determined by the investigators.
AEs, adverse events; TEAEs, treatment-emergent adverse events.
Vital signs, laboratory findings, and other observations related to safety
Minimal changes from baseline to the EOS visit were observed in all vital sign categories across the treatment group. Three abnormal BP findings were noted after baseline. One patient had an abnormal systolic and diastolic BP (156/110 mmHg) at the EOS visit, and another had an abnormal diastolic BP (96 mmHg). Physical examination at the EOS visit resulted in observation of a total of 10 normal-to-abnormal shifts; 3 in the head, eyes, ears, nose, and throat, 1 in the extremities, and 2 each in the skin, lymph nodes, and musculoskeletal system. Eight of these 10 shifts were determined as “not clinically significant” by the investigator. The remaining two shifts (sebaceous cyst right axilla, mild in severity; swollen adenoids/tonsillitis, moderate in severity) were not related to treatment. There were no notable observations in the mean, median, or minimum/maximum changes from baseline in any laboratory parameter. Chemistry parameters with notably high proportions of subjects with shifts from normal at baseline to abnormal at EOS included: alanine aminotransferase (3.3%), aspartate aminotransferase (6.0%), alkaline phosphatase (3.3%), bilirubin (6.3%), and blood urea nitrogen (6.0%).
Clinical response to treatment
Although the primary objective of this study was to conduct a safety analysis, investigators were asked to determine whether additional treatment was needed. Fifteen out of the 321 patients evaluated had missing data, leaving 306 evaluable patients. Of these, 222 (72.5%) did not need additional treatment at the EOS visit. A post hoc analysis determined that 159 patients in the 275-patient subset with both baseline and EOS vaginal assessment data were clinical responders (57.8%).
Discussion
Secnidazole is a 5-nitroimidazole antibiotic that has been used worldwide for the treatment of various infections, such as trichomoniasis, although it is unavailable for use in women with BV in the United States. 25 Eight studies have investigated the efficacy of secnidazole monotherapy for the treatment of BV and other vaginal infections, including the large, phase 3, randomized, double-blind, double-dummy non-inferiority study comparing secnidazole and metronidazole that was conducted in France, 25 and several smaller open-label studies. 19,21,25,27 –30
Phase 3 studies can be designed to confirm the efficacy or the safety of a new product. This study was designed to evaluate the safety of secnidazole. Such a phase 3 study was designed and conducted because the efficacy of secnidazole could be demonstrated in a relatively small number of subjects (mITT = 164 subjects), 24 whereas the patient population with BV is relatively large and comprises overall healthy women. Extrapolating safety data from our previous phase 3 study (safety population, n = 189) 24 to the larger population generally warrants a phase 3 study to collect more safety data, especially for a patient population that is healthy and consequently, with less risk tolerance when they require treatment.
This is the first safety study undertaken to evaluate a novel single-dose formulation of secnidazole in U.S. patients. Secnidazole 2 g was well tolerated, with the overall number of TEAEs being 95 (29.6%). The overall number of treatment-related TEAEs in this study was low (53 [16.5%]), and it included vulvovaginal mycotic infection/candidiasis (5.3%), nausea (4.4%), and dysgeusia (3.1%). The frequencies and types of treatment-related TEAEs were similar to those occurring in previously reported randomized trials. 25,31 For example, AEs were experienced by 109 (38%) patients treated with metronidazole and by 113 (39%) of those treated with secnidazole in a randomized clinical trial. 25 The percentages of treatment-related TEAEs were 22.7% (n = 65) and 22.4% (n = 65), respectively. In this study, there were no deaths, and two patients reported SAEs: One SAE was possibly related to study treatment (loss of consciousness), and one was unrelated (a wound secondary to a foot burn). Two patients discontinued from the study due to a TEAE (both yeast infections).
The favorable tolerability profile of single-dose secnidazole may be directly related to its pharmacokinetic properties. Single-dose secnidazole 2 g has a longer t 1/2 than metronidazole, has high bioavailability, and its rapid absorption (time to maximum plasma concentration [C max] median 4 hours) provides high C max (mean [%CV] 45.4 μg/mL). 31 In addition, coadministration of single-dose secnidazole 2 g with contraceptives, ethinyl estradiol 2/norethindrone, on the same day or 1 day apart was well tolerated and had no clinically relevant effects on the bioavailability of either hormonal contraceptive. 31 Notably, treatment with single-dose secnidazole requires 3 days of alcohol abstinence compared with metronidazole, which requires 10 days of abstinence (7 days of treatment plus 3 days after treatment). Use of oral metronidazole is also associated with a disulfiram-like reaction to alcohol, including abdominal cramps, nausea, vomiting, headaches, and flushing. 22
Conclusions
Administered as a single dose, secnidazole 2 g has the potential for improved patient adherence, improved real-world efficacy outcomes, and lower numbers of treatment failures due to an incomplete antibiotic course. Secnidazole 2 g ultimately addresses an unmet need for a single oral dose versus the currently used treatment regimens that require dosing for up to 7 days, a treatment course known to impact adherence in more than 50% of patients, as stated earlier. 32 In addition, secnidazole 2 g has low systemic side effects, with minimal effects on vital signs and laboratory values. This open-label study demonstrated a low frequency of AEs, with only 53 (16.5%) deemed treatment related by investigators. Although the primary objective of this study was to collect safety data in a large population of women with BV, investigators also determined that 222 out of 306 patients (72.5%) did not need further treatment by the EOS visit. A single-dose formulation of secnidazole offers a safe and well-tolerated treatment option that has the potential to resolve BV in women with 1 treatment.
Footnotes
Acknowledgments
Editorial and medical writing assistance was provided by Maryn Padula, PhD, of Virtuoso Healthcare Communications, supported by Symbiomix Therapeutics, LLC, Baltimore, MD, the manufacturer of SOLOSEC™ (secnidazole) Oral Granules. The authors were fully responsible for the content, editorial decisions, and opinions expressed in this article. The authors did not receive an honorarium related to the development of this article.
Author Disclosure Statement
Dr. Chavoustie has received personal fees from Symbiomix Therapeutics. Dr. Gersten has nothing to disclose. Dr. Samuel has nothing to disclose. Dr. Schwebke has received grant funding from Symbiomix Therapeutics, BD Diagnostics, Hologic, Curatek Pharmaceuticals, Toltec Pharmaceuticals, Alfa Wasserman, StarPharma, and LabCorp of America. She is also a paid consultant for Symbiomix Therapeutics.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.