
Abstract
Background:
Experiencing mental health difficulties during pregnancy predicts a variety of quality-of-life (QoL) outcomes for Black women. However, one area of prenatal mental health remains underresearched: attention-deficit/hyperactivity disorder (ADHD). Given the impairments reported by adults with significant symptoms of ADHD and the linkages between depression and ADHD in nonpregnant samples, the current study aimed to examine the relationships among ADHD symptoms, depression, and QoL in Black pregnant women.
Materials and Methods:
Participants for this study were 116 pregnant Black women aged 18–43 years (mean age = 27.14, standard deviation = 5.67) presenting to an urban women's health clinic. We investigated associations among maternal ADHD symptoms, risk of maternal depression, and different aspects of QoL, including relationships, life outlook, and life productivity.
Results:
Linear hierarchical regressions were performed to investigate the ability of maternal depression risk to mediate the relationship between maternal ADHD symptoms and QoL. Moderate to large negative correlations were found between maternal ADHD symptoms, depression risk, and quality of life (p's ≤ 0.001). Furthermore, maternal depression risk either partially or fully explained the relationship between ADHD symptoms and the different QoL variables.
Conclusions:
This study illustrates that symptoms of both ADHD and depression are important clinical considerations for Black women during pregnancy. As significant ADHD symptoms can lead to the development of depression, future research should investigate the temporal relationship between depression and QoL in pregnant women diagnosed with ADHD, as well as study whether ADHD treatment results in improvements in depressive symptoms.
Relationships Between Maternal Psychopathology and Quality of Life in Black Pregnant Women
A
While the relationship between certain areas of psychopathology (e.g., depression and anxiety) and QoL during pregnancy is well established, other mental health conditions have received far less attention in the prenatal literature. One such condition is attention-deficit/hyperactivity disorder (ADHD) with core symptom domains of inattention (e.g., forgetfulness, trouble sustaining attention) and hyperactivity/impulsivity. 8 ADHD is a neurobiological condition typically identified in childhood, with a median age of onset (11 years old) that is earlier than the median age of onset for mood disorders (30 years old 9 ). The majority of children diagnosed with ADHD in childhood continue to meet criteria in adulthood (∼65% 10 ). In adulthood, ADHD symptoms are associated with significant impairments in multiple domains of daily life, such as lower job performance, 11,12 more problems in interpersonal relationships, 13 and lower levels of martial satisfaction. 14 In light of these struggles in daily life, it is unsurprising that adults with ADHD report significantly lower QoL. 15
Notably, there is strong evidence that maternal psychopathology is associated with behavioral difficulties in children 16 ; this relationship seems to be at least partially attributed to the impact of psychopathology on parenting behavior. 17 Both maternal depression and maternal ADHD symptoms, in particular, have been linked to parenting difficulties such as less use of positive parenting strategies such as praise and lower levels of involvement. 17,18 Furthermore, maternal depression is a strong early predictor of conduct problems in children with ADHD specifically. 19 In sum, it is clear that maternal psychopathology, including symptoms of ADHD and depression, are associated with more difficulties in parenting and more negative child outcomes. 17 –19 Early identification of maternal psychopathology is therefore an important goal not only for the well-being of mothers but also for promoting positive parenting and better outcomes for children.
In addition, rates of depression are higher among adults with high levels of ADHD symptoms. 20 Given that the age of onset for ADHD is earlier than the median age of onset for depression, 21 it is most likely that the presence of ADHD increases risk for later depression, as opposed to the presence of depression contributing to increases in ADHD. There is evidence that ADHD may lead to depressive symptoms 22 through multiple frustrations and failure experiences, which negatively impact an individual's sense of self-worth and competency. 23,24 Furthermore, some of the symptoms of ADHD do overlap with symptoms of depression. For example, trouble concentrating, forgetfulness, and executive functioning difficulties are associated with both depression 25 and ADHD in adulthood. 26,27 Hence, it may be that ADHD impacts QoL in pregnant women both directly, through its negative impact on functioning in multiple life domains, 11 –13 and indirectly, by increasing risk for depressive symptomology, 20,22 which in turn negatively impacts QoL. In addition, investigations of this relationship should take into account the potential for overlap between ADHD and depression.
To date, only one study has investigated the associations between ADHD symptoms and QoL in pregnant women. 23 In this study, higher levels of ADHD symptoms negatively predicted functioning in multiple areas, including professional life, relationships, and daily life activities. 23 However, this study did not investigate the role of possible depression in the association between ADHD symptoms and impairment. As noted above, the impact of ADHD on QoL may operate indirectly through symptoms of depression in addition to a direct impact. No additional studies have investigated QoL as it relates to symptoms of ADHD in pregnant women. Given the struggles observed in nonpregnant adults with significant symptoms of ADHD, it is important to investigate the relationship between ADHD symptoms and QoL in this vulnerable population. Furthermore, given the strong links between depression and QoL, it may be that depression acts as a mediator of the relationship between ADHD and QoL in pregnant women.
Black women are one group particularly vulnerable to both adverse mental health outcomes and poor QoL during pregnancy. Compared to nonBlack pregnant women, Black pregnant women report more negative life events, 28 increased psychosocial stress 29 and increased depressive symptoms. 30 These mental health disparities may also be responsible for racial disparities in QoL during pregnancy. 31 Investigating factors which may predict QoL in pregnant Black women is an important step in aiding the identification and prevention of depression and improving QoL overall in this population.
Currently, there is no research examining the impact of ADHD on Black women, either during pregnancy or in adult Black women in general. In fact, there is a notable paucity of research on Black adults with ADHD. Conducting a PsycINFO database search with the terms “ADHD,” “Black or African American” and “Adult” returns only 14 studies. None of these articles presents empirical research on how symptoms of ADHD impact the lives of Black adults; at best, these articles review barriers to treatment and the need for culturally informed assessment and treatment of Black adults with ADHD. Clearly, this represents an important gap in the literature on adults with ADHD. Moreover, given the disparities in other mental health-related outcomes reported in pregnant Black women, it is likely that disparities associated with symptoms of ADHD also exist. Identifying disparities will aid in identifying targets for prevention and intervention to promote better QoL in Black pregnant women.
The primary aim of the present study was to investigate the relationships among ADHD symptoms, depression, and QoL in pregnant Black women. Consistent with past research, we hypothesized that both ADHD symptoms and depression risk would be negatively correlated with different aspects of QoL, including relationships, life outlook, and life productivity. Furthermore, given the strong relationships found in the literature between ADHD and depression as well as depression and QoL, we also hypothesized that ADHD would have an indirect effect on QoL via symptoms of depression risk.
Materials and Methods
Participants
One hundred sixteen Black pregnant women participated in the current study, as part of a larger parent study of prenatal behaviors, maternal psychopathology, and QoL. In the current study, women ranged from 18 to 43 years of age (M = 27.14, standard deviation [SD] = 5.67). All participants identified their racial group as “Black,” and the vast majority (99%) identified their ethnic group as “Non-Hispanic.” Participants' reports of estimated gestational age ranged from 5 to 40 weeks (M = 26.17, SD = 9.36). Approximately 81% of the women reported being single, and over half of the sample was unemployed. See Table 1 for demographic details.
Three participants did not provide income information.
GED, General Education Diploma.
Measures
Conners Adult ADHD Rating Scales-Self-Report: Short Version
The Conners Adult ADHD Rating Scales-Self-Report: Short Version (CAARS-S:S) quantitatively measures the presence and severity of ADHD symptoms in adults using 26 items that assess symptoms across clinically significant domains. Each statement is rated on a four-point Likert scale, from “not at all” to “very much/very frequently.” The scale includes a 12-item ADHD Index, 32 which is used as a screen for those at risk for ADHD. Scores were calculated for each participant using age-based norms for women. This measure was developed and normed using a large multisite sample of nonclinical adults. Cronbach's α for the current sample was good (ADHD Index α = 0.82). We used the ADHD Index as a dimensional measure of ADHD symptoms (and continuous predictor) in our adult sample. A cutoff score of T = 70 was used to determine the percentage of participants scoring in the clinically significant range, as suggested by Conners and colleagues. 32
Adult ADHD QoL Questionnaire
The Adult ADHD QoL Questionnaire (AAQoL) was designed to assess how symptoms of ADHD impact QoL. The AAQoL is a reliable and valid measure of QoL in adults. 33,34 Given that diagnostic status was not assessed in this study, this measure was adapted to ask generally about the participant's QoL in different areas (not specific to ADHD). This measure has 29 total items and 4 subscales. The Life Productivity subscale consists of 11 items that assess an individual's ability to manage everyday tasks and avoid other problems related to procrastination, task initiation and completion, and disorganization. The Life Outlook subscale has seven items framed as positive assertions and self-perceptions (e.g., “your energy is well spent”). The Relationships subscale contains five items that describe an individual's social relationships across contexts (e.g., tensions in relationships). The individual items have five-point Likert scale responses ranging from “not at all/never” to “extremely/very often.” Finally, the Psychological Health subscale broadly evaluates mental health symptoms (e.g., anxiety, depression, over reactivity), but given the overlap in this subscale and the depression risk measure, this subscale was not used in the current study. Cronbach's α's for the current sample were good (Life Productivity α = 0.94, Life Outlook α = 0.82, Relationships α = 0.80).
Patient Health Questionnaire-2
The Patient Health Questionnaire-2 (PHQ-2) is a 2-item version of the Patient Health Questionnaire, which assesses the frequency of a patient's depressed mood and anhedonia over the past 2 weeks. The two items were “little interest or pleasure in doing things” and “feeling down, depressed, or hopeless,” with a four-point Likert ranging from “not at all” to “nearly every day.” The PHQ-2 has good sensitivity and specificity for identifying major depression in adults. 35,36 Its brief nature makes it an appropriate screen for depression in a medical setting, 37 as it measures for the presence of two symptoms of depression. For the purposes of this article, scores on this screen will hereafter be referred to as “depression risk.” Furthermore, the symptoms of depression assessed by the PHQ-2 do not overlap with symptoms of ADHD in adulthood, thereby reducing the likelihood that the relationship between ADHD symptoms and depressive symptoms can be attributed to symptom overlap.
Demographics
A demographic questionnaire assessed for number of weeks' gestation and participants' age, marital status, race, ethnicity, income level, highest level of education, and employment status. Participants also reported on their number of weeks pregnant.
Procedure
Participants were recruited at a women's health clinic at a large southeastern urban university hospital. As the women checked in for their appointments, they were informed of their potential eligibility for the current research study. If the woman was interested in learning more about the research study, a clinic staff member directed her to the study staff, stationed at the back of the waiting room. Study staff reviewed eligibility criteria and the consent form with interested participants. Consented participants completed the survey questions in the clinic waiting room, as they waited for their medical appointment. Study staff were available to answer any questions during the survey administration. Participants were compensated with $25 for their time. The university's institutional review board approved this study.
Statistical analyses
All analyses were conducted using IBM SPSS Statistics (Version 22). Mediation analyses were conducted using the PROCESS macro, 38 which allows for the testing of mediation models, including both direct and indirect effects. PROCESS generates bias-corrected bootstrapped estimates of the confidence intervals (CIs) for indirect effects. For this study, 95% CIs are considered significant if they do not include zero, and 5,000 replications (bootstrapping tests) were used. Means, ranges, and the percent of participants scoring above the clinical cutoff on study measures are presented in Table 2.
ADHD, attention-deficit/hyperactivity disorder; CAARS, Conners Adult ADHD Rating Scale; PHQ-2, Patient Health Questionnaire-2; QoL, Adult ADHD Quality of Life Questionnaire.
Bivariate correlations using Pearson's correlation coefficient and Spearman's rank-order correlation coefficient were first conducted between all study variables, as well as between study variables and three possible confounding variables (i.e., maternal age, gestational age, and income). Based on the results and findings from past literature, income was chosen to be included as a covariate in all following analyses. Three separate mediation analyses were then conducted. In each model, ADHD symptoms were entered as the independent variable and depressive symptoms as the mediating variable. Each model contained one of the three QoL subscales as the outcome variable. Missing data in the study were minimal; no variable contained more than 8% missing data. As such, pairwise deletion was used to handle missing data.
Results
Bivariate correlations
Bivariate correlations are presented in Table 3. As expected, ADHD and depression risk were strongly positively correlated (r = 0.54, p < 0.001). ADHD symptoms were also negatively correlated with all three AAQoL subscales (r ranging from −0.34 to −0.67, p ranging from 0.001 to <0.001), such that higher levels of ADHD symptoms were associated with lower levels of QoL. In addition, depression risk was negatively correlated with the three AAQoL subscales (r ranging from −0.32 to −0.57, p ranging from 0.001 to <0.001), with increased depression risk relating to decreased QoL. These moderate to large correlations between the variables of interest indicated that mediation analyses were appropriate to perform.
All correlations presented are Pearson correlation coefficients, with the exception of correlations with Income, which are Spearman's rank order correlation coefficients.
p < 0.001; * p < 0.05.
We also examined the correlation of the study variables with potential confounding variables, including income, maternal age, and gestational age. Pearson correlation coefficients were used for maternal and gestational age, whereas Spearman's rank-order correlation coefficients were used for income, which was an ordinal variable. None of these variables was significantly correlated with any of the study variables. As such, maternal age and gestational age were not included as covariates in the main analyses.
Mediational analyses
Given the well-established link between socioeconomic status (SES) and depression as well as the literature suggesting income to be the SES indicator most strongly associated with depression in Black females, 39 all mediation analyses included income as an ordinal covariate.
In the first model (Fig. 1), there was no significant indirect effect of depression risk on the relationship between ADHD symptoms and life productivity when controlling for income, b = −0.13, SE = 0.15, and 95% CI = −0.47 to 0.12. There was a significant direct negative relationship between ADHD symptoms and life productivity, when accounting for the effect of depression risk, b = −1.49, SE = 0.23, t = −6.35, and p < 0.001, indicating that higher levels of ADHD symptoms were associated with lower levels of life productivity.
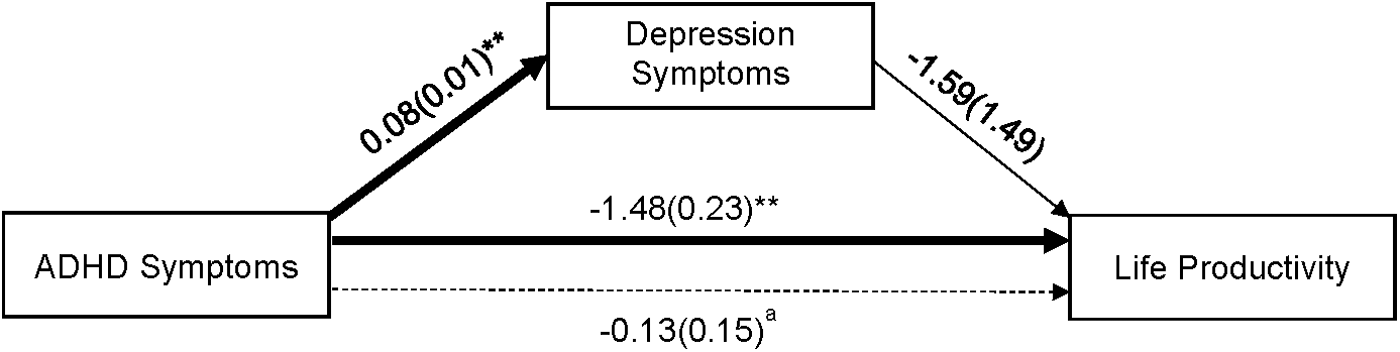
Mediation model of the associations between ADHD and Life Productivity through symptoms of depression. Unstandardized coefficients are reported outside of parentheses, standard errors reported inside parentheses. Solid lines represent direct pathways; dashed line represents indirect (ab) pathway. Model includes income as ordinal covariate. **p < 0.001; aindirect pathway is not significant. ADHD, attention-deficit/hyperactivity disorder.
In the second model (Fig. 2), there was a significant indirect effect of depression risk on the relationship between ADHD and life outlook, b = −0.30, SE = 0.12, 95% CI = −0.57 to −0.07. Greater levels of ADHD symptoms predicted higher amounts of depression risk, b = 0.09, SE = 0.01, t = 6.71, and p < 0.001, which in turn predicted less positive life outlook, b = −3.34, SE = 1.46, t = −2.29, and p = 0.02. There was no significant direct effect of ADHD symptoms on life outlook when accounting for the effect of depression risk, b = −0.46, SE = 0.23, t = −1.97, and p > 0.05, indicating that depression risk fully mediated this relationship.

Mediation model of the associations between ADHD and Life Outlook through symptoms of depression. Unstandardized coefficients are reported outside of parentheses, standard errors reported inside parentheses. Solid lines represent direct pathways; dashed line represents indirect (ab) pathway. Model includes income as ordinal covariate. **p < 0.001; *p < 0.05; bindirect pathway is not significant.
In the third model (Fig. 3), there was a significant indirect effect of depression risk on the association between ADHD and relationships, b = −0.24, SE = 0.12, and 95% CI = −0.51 to −0.02. Higher levels of ADHD symptoms predicted greater levels of depression risk, b = 0.08, SE = 0.01, t = 6.60, and p < 0.001, which in turn significantly predicted poorer QoL as related to relationships, b = −2.91, SE = 1.43, t = −2.03, and p = 0.04. There was a significant direct negative effect of ADHD symptoms on relationships when accounting for levels of depression risk, b = −1.12, SE = 0.21, t = −5.29, and p < 0.001, indicating that depression risk partially mediated this relationship.

Mediation model of the associations between ADHD and Relationships through symptoms of depression. Unstandardized coefficients are reported outside of parentheses, standard errors reported inside parentheses. Solid lines represent direct pathways; dashed line represents indirect (ab) pathway. Model includes income as ordinal covariate. **p < 0.001; *p < 0.05; bindirect pathway is not significant.
Discussion
In this study, we investigated the relationship among ADHD symptoms, depression risk, and QoL in Black pregnant women. We found that ADHD symptoms and depression risk were positively related, and both forms of psychopathology were negatively related to QoL. Further, depression risk at least partially explained the relationship between ADHD symptoms and two areas of QoL, thus providing support for the importance of screening for depression and ADHD as risk factors for poor QoL in pregnant women.
Our finding that ADHD symptoms correlated with depression risk and QoL was consistent with prior research in nonpregnant populations. 20 For Black women specifically, a higher than expected prevalence rate of depression has been found in cross-sectional studies of depressive symptoms in primary care settings. 40 This finding is particularly notable in low-income samples, such as the one described herein, given the health disparities that exist for low-income, racial minority pregnant women. Also, as noted earlier, although not yet studied in Black women specifically, a number of studies have found that ADHD may confer risk for depression in both children and adults. 22,41 Furthermore, poorer QoL has been found to be predictive of significant symptoms of ADHD 15 or depression, 42 given that both disorders are associated with functional impairment in different domains, such as social relationships. Finally, pregnancy itself is associated with a number of significant stressors (e.g., physical and hormonal changes to the woman's body, decreased work productivity in the third trimester) that put women at risk for depression. 43 Thus, the bivariate associations found in our sample of Black pregnant women were in the expected direction.
Depression risk emerged as a full mediator of the relationship between ADHD symptoms and life outlook, suggesting that the link between ADHD symptoms and life outlook, or how one views the future, in Black pregnant women is fully explained through risk for depression. Thus, even though adults with ADHD have a more negative life outlook than those without ADHD 33 for pregnant women, it is actually depression risk that may best elucidate this relationship. Given that one of the diagnostic criteria for a major depressive episode is hopelessness or feeling as though one's future is not positive, and this finding is unsurprising. Hopeless feelings in Black pregnant women may lead them to disengage from behaviors that would allow them to feel positively about their future (e.g., avoidance of social activities, declining productivity at work). This is particularly concerning as hopelessness in pregnant women is associated with postpartum depression and suicide risk. 44 Therefore, while ADHD may be important to consider for pregnant women with regard to impairment across different areas of their lives, 23 assessing for depression among pregnant women remains vital to clinical practice.
Depression risk partially explained the relationship between ADHD symptoms and relationships for Black pregnant women, indicating that it helps to explain why women with increased ADHD symptoms may report poorer satisfaction with the relationships in their lives. For instance, an example item on this subscale is “tension in relationships.” Women with ADHD report significant relationship problems, reporting more conflict and few relationships. 45,46 Our findings suggest that depression risk also plays an important role in QoL for pregnant women. Researchers have documented the role of social support in determining how Black pregnant women perceive stress, particularly for those who live in lower quality neighborhoods. 47 For instance, Giurgescu et al. found that, for Black pregnant women, living in poor-quality neighborhood was associated with increased stress, but social support fully mediated that relationship. Thus, for Black pregnant women, having positive relationships and feeling supported during pregnancy is vital. Interventions that result in increased social support and improved relationship quality, such as interpersonal therapy for depression or cognitive behavioral therapy, for Black women at risk for depression and ADHD may be warranted.
Finally, depression risk did not account for the relationship between ADHD symptoms and life productivity. In our mediation model, we did find that ADHD predicted poorer life productivity, which is consistent with previous research indicating that adults with ADHD report significantly less life productivity than those without the disorder. 33 According to the literature, adults with ADHD are more likely to miss days from work and produce work of lower quality, 48 related to the executive function deficits in time management and self-motivation that are noted in people with the disorder. 26 As depression risk did not explain this linkage in our sample, for pregnant women, there may be other explanatory variables, such as executive functioning deficits (which are linked to ADHD), that should be measured in subsequent studies.
Study limitations
The current study has important implications for the QoL in pregnant women; however, a few limitations must be noted. First, the use of a cross-sectional design limits the ability to draw firm conclusions about the direction of the relationships among ADHD symptoms, depression risk, and QoL. For instance, it may be that lowered QoL leads to increased depression risk in this population or that ADHD is the mediator of the relationship between depression risk and QoL. While we believe that there is empirical and theoretical justification for the directions of the relationships we chose to measure, cross-sectional data do not allow us to definitely confirm these hypotheses. Second, only self-report measures were utilized, while the best practice for assessment of ADHD typically includes reports from other individuals such as spouses or parents. 49 However, there is evidence that adults can provide fairly accurate reports of their current symptoms, and indeed, the utilization of self-report measures to measure psychopathology is a typical practice by physicians. 50,51 However, we also did not conduct semistructured interviews, which are often used by mental health professionals to diagnose ADHD or depression. A small but significant subset of our sample (19.1%) reported clinically significant symptoms of ADHD, which represented a higher prevalence than is found in the general population (8%–9% lifetime prevalence rate 21 ). A more comprehensive assessment for ADHD would better describe who actually met diagnostic criteria for the disorder. Thus, the use of both multiple raters and multimethod assessment would help to further explain the relationships found among ADHD, depression risk, and QoL.
Conclusions
This study represents an important first step toward examining relationships among ADHD, depression, and QoL during pregnancy among low-income Black women, a group at high risk for adverse mental health outcomes and life stressors. Future studies should investigate the trajectories of these symptoms and their relationship to one another before, during, and after pregnancy. Longitudinal studies will allow researchers to track the course of ADHD symptoms and depression throughout pregnancy. Furthermore, a recent cross-sectional study found that ADHD symptoms during pregnancy relate to significant difficulties engaging in prenatal health behaviors, such as eating healthy foods and avoiding strenuous activities. 52 Therefore, future research should endeavor to better elucidate the course of ADHD symptoms during and immediately following pregnancy. In addition, there is little data about how (or if) women with ADHD engage in treatment during a pregnancy. Studying such phenomena will inform efforts to identify women who are most at risk for lowered QoL during pregnancy and to provide evidence-based intervention and treatment for women in need of care.
Healthcare professionals working with pregnant Black women should consider routine screenings for both ADHD and depression, especially among women who report significant problems in their QoL or daily functioning. There are multiple brief screening measures designed to assess symptoms of depression, including the Patient Health Questionnaire 53 and the Edinburgh Postnatal Depression Scale. 54 Brief measures of ADHD symptoms are also available, such as the Barkley Adult ADHD Rating Scale-Quick Screen (8 items) 55 and the Adult ADHD Self Report Scale (for which a 6-item screener is available). 9 Healthcare professionals who work with pregnant women with depression or ADHD should provide information to patients about the potential impact of these conditions on QoL during pregnancy. Furthermore, healthcare providers can collaborate with patients to discuss strategies to manage symptoms, including brief interventions or referrals to mental healthcare providers for such evidence-based treatments as cognitive behavioral therapy for ADHD or for depression.
This study provided an investigation of the relationships between ADHD symptoms and QoL in pregnant women. There is a clear need to assess the efficacy of existing mental health treatments for pregnant women and to consider whether adaptations or new protocols are needed. Pregnancy is a time of transition, and this study provides evidence that the relationships among ADHD symptoms, depression risk, and QoL in this population deserve further investigation.
Footnotes
Acknowledgments
This research was funded by a small internal grant awarded to the first author. The authors thank the patients and staff at the participating women's clinic for their contribution and interest in this area of study. The authors also acknowledge the work of all study staff in participant recruitment and data collection.
Author Disclosure Statement
No competing financial interests exist.