
Abstract
Purpose:
Cervical cancer screening reduces the incidence and specific mortality rate of cervical neoplasms. In most cases screening by means of Pap smears is performed in France by gynecologists. The primary objective of this study was to confirm whether the participation rate is increased when general practitioners (GPs) carry out the smears themselves. The secondary objective was to evaluate other independent characteristics of GPs predicting participation rates in women.
Methods:
The population of 347 GPs, including their relevant characteristics and their 90,094 female patients eligible for screening over 2 years (2013–2014), was derived from the SIAM claim database of the Flanders Healthcare Insurance Fund (CPAM). A telephone survey among all GPs was carried out to know whether they were performing smears in their surgeries.
Results:
A total of 343 GPs were included for analysis (98.8% participation rate). The mean cervical cancer screening participation rate over 2 years among all the women in the recommended age group (25–65 years) was 43.3% (±6.9). Bivariate analysis showed that participation rate was higher when the GP performed smears (adjusted difference of mean: 2.06 [95% CI: 0.67–3.45], p = 0.037) and whether the GP was female (2.08 [0.42–3.74], p = 0.0144). After multivariate analysis the only significant characteristic of the GP was the performance of smears (1.71 [0.27–3.16], p = 0.0204).
Conclusions:
Cervical smears performed by GPs led to increased screening participation rates within the recommended age group of women. However, the size of this increase is insufficient to reach the expected participation rates.
Introduction
C
To screen for cervical cancer, the French National Authority for Health (Haute autorité de santé, HAS) guidance recommends to perform cervical smears for Pap tests among all women from 25 to 65 years of age. The test is performed every 3 years, after two initial negative tests. 6 However, the implementation of cervical cancer screening in France does not match the HAS guidance. 4,7 GPs and midwives can carry out Pap smears, but in most cases these are performed by gynecologists, varying from 70% to 90% according to regions. 8,9 As the number of gynecologists is drastically decreasing in France and as most of deprived women are not managed by a gynecologist, French authorities encourage GPs and midwives to perform cervical smears for Pap tests. Indeed, depending on different sources (insurance claim databases, national census), about 80%–90% of unscreened female patients meet their GP yearly, for themselves or for a relative.
The literature describes many factors influencing participation in cervical cancer screening. Factors with a positive influence are: female doctor 10 –12 and medical monitoring by a gynecologist. 13 In addition, information provided on cervical cancer screening, and an incentive to cervical cancer screening carried out by GPs improves participation. 8,9,14 –16 A nationwide population-based program betters the participation rates, mainly in women with a low educational level, 6,17 –20 but in France, screening for cervical cancer remains opportunistic. The organization of the screening in 13 counties (départments) between 2010 and 2014, led to an increase of the participation rate by 12%. 21 Factors with a negative influence are: barriers to access to GPs and gynecologists and the nonutilization of their services, 22 geographical distance, and cultural or organizational factors. 15,16,23,24 The screening rate is also lower among socially deprived and less educated women. 9,15,16,25
The socioeconomic level of the geographical area of a GP surgery can be defined by the European Deprivation Index (EDI). The EDI is a validated composite indicator combining 10 weighted variables retrieved from the census. 26 In France, the mean EDI is 0 ± 1.8. In the health insurance district encompassing our study, the mean EDI is 2.1, corresponding to a socioeconomically slightly deprived area. Another preliminary study performed by our study group found that the EDI of the GP surgery setting was strongly correlated with patient screening participation rates independently of GP characteristics. [publication under submission]
The primary objective of this study was to confirm whether the cervical cancer screening participation rate is increased when general practitioners (GPs) perform cervical smears by comparison with the rate among GPs who do not perform these smears themselves, regardless of the management by a gynecologist or a midwife. The secondary objective was to evaluate other independent characteristics of GPs predicting cervical screening participation rates in their female patients.
Materials and Methods
Design
We conducted a retrospective analysis of a database extracted from the SIAM ERASME claim database of the Healthcare Insurance Fund (CPAM) of French Flanders, coupled with a cross-sectional survey. Excepting specific follow-up, the SIAM database keeps data on patients' level for 2 years.
Target population
The target population consisted of all GPs practicing in primary care settings, registered at the Flanders Healthcare Insurance Fund from January 1st, 2013 to December 31, 2014. Exclusion criteria were: retired GPs and GPs with less than 100 listed female patients (to eliminate recently settled GPs and GPs with peculiar practices, such as echography, acupuncture, homeopathy or angiology).
Data acquisition
The SIAM claim database of the Flanders Healthcare Insurance Fund (CPAM) provided for each GP data characterizing their medical practice between January 1st, 2013 and December 31, 2014. In the French fee for service payment system, the cytological analysis of cervical samples is rated by the cytologist on the health insurance invoice using specific codes depending on the analysis technique (classical smear or liquid-based cytology). The outcome was the number of female patients between 25 and 65 years of age (range of age framed for cervical screenings) with a cervical cytology code over the 2 years.
All GPs in the area were called by telephone from January 1st, 2015 to February 6, 2015. They were asked whether they were performing Pap smears in their surgeries themselves or not. The main explicative variable was the performance of cervical smears by the GP.
Secondary explicative variables collected from the SIAM claim database were the gender of the GP and the burden of activity estimated by the number of all listed patients and female listed patients.
The dataset was completed by the search of the EDI of each GP surgery's geographical setting.
Statistical analyses
Quantitative variables are expressed as mean ± standard deviation, median, and interquartile and the categorical variables are expressed as numbers (percentage). In this study, there were two levels for data: the individual level (GP's characteristics and the outcome “the cervical cancer screening participation rate”) that were nested in the geographical level (EDI). All analyses were performed by using a hierarchical mixed model. This statistical model takes into account the hierarchical structure of data. The association between each individual characteristic of GP's and the screening participation rate was first analyzed separately with an adjustment on EDI. The GP's level variables having a p-value less than 0.2 were introduced in a multivariate analysis (adjusted for EDI) to identify the subset of variables linked to the outcome (the cervical cancer screening participation rate). The significant level for the tests was 0.05. Data were analyzed using SAS software (version 9.3; SAS Institute, Inc., Cary, NC).
Results
A total of 402 GPs were registered at the CPAM of Flanders between January 1st, 2013 and December 31, 2014. Fifty GPs were excluded due to a number of listed female patients lower than one hundred. Five GPs were excluded due to retirement. Of the 347 eligible GPs, totalizing 343 GPs (131,053 female patients) and a total of 90,094 female patients between 25 and 65 years eligible for screening, only 4 GPs refused to participate in the survey (participation rate: 98.8%). In total, 343 GPs were included for analysis (Fig. 1). The median number of patients by GP was 668 (interquartile interval: 491–852). Characteristics of the included GPs are shown in Table 1.
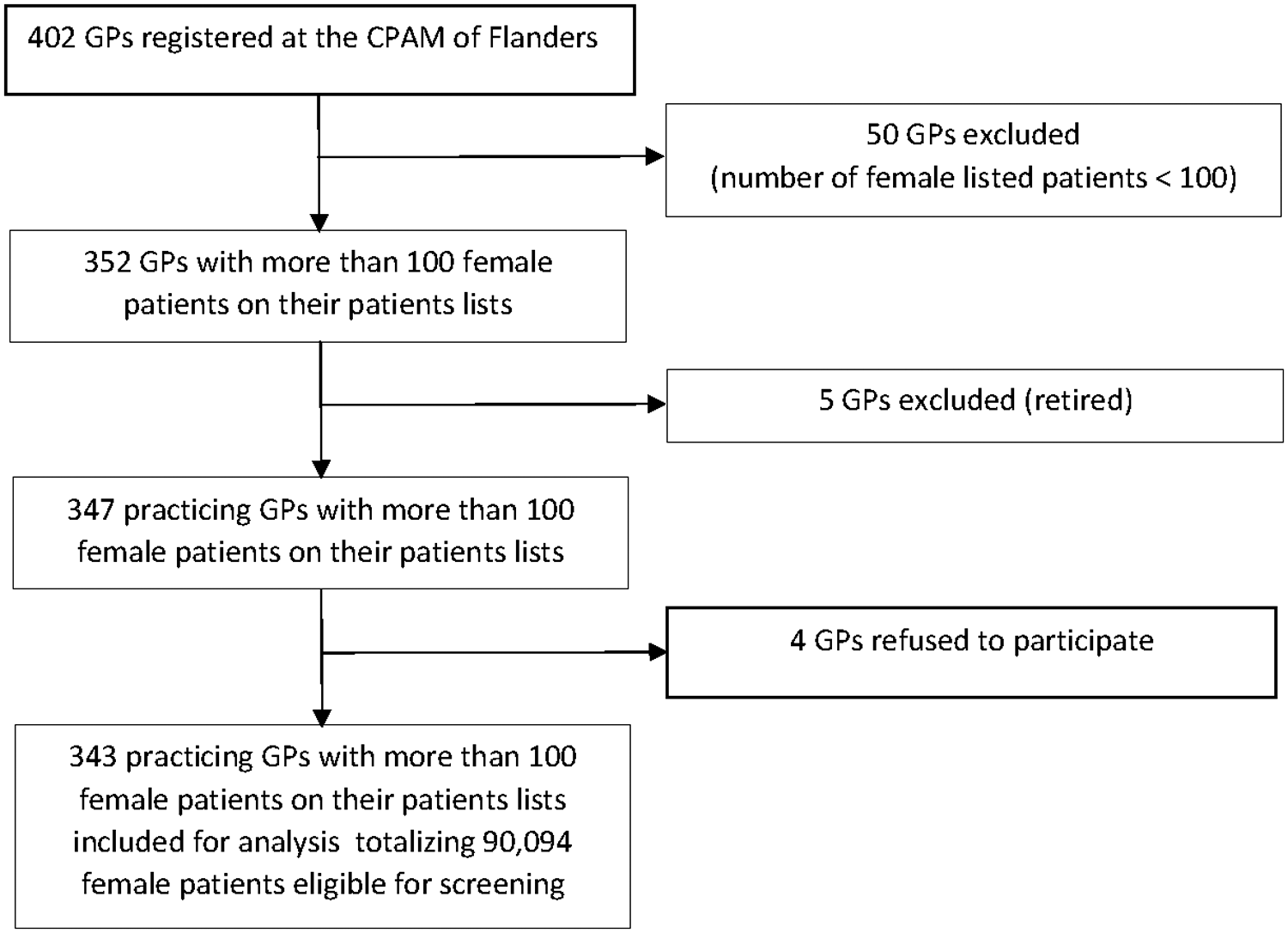
Flow diagram.
N, number; %, percent; SD, standard deviation; Q1, first quartile; Q3, third quartile; EDI, European deprivation index.
Most of GPs were males (78.4%). Out of 343 GPs, 182 (53.1%) reported performing cervical smears themselves, 79.7% (n = 59/74) in female GPs versus 45.7% (n = 123/269) in males. The mean screening participation rate among all the women was 43.3% (SD: ±6.9%).
Bivariate analyses were performed to analyze the association between the screening participation rate and different characteristics after adjustment for the EDI of the geographical area of the GPs' surgeries. The adjusted mean of the screening rates for the group of women who saw GPs who perform smears versus the group who saw GPs who do not were 44.41 (±0.15) versus 42.35 (±0.54), respectively (adjusted difference of mean: 2.06 [95% CI: 0.67–3.45], p = 0.037). The gender of the GP also significantly influenced screening participation percentages, the mean rate in female GPs being greater than for males (adjusted difference of means: 2.08 [95% CI: 0.42–3.74], p = 0.0144) (Table 2).
Coefficient of mixed model adjusted for EDI.
Coefficient represents the mean difference in participation rate (vs. reference), adjusted for EDI (IC95%).
Adjusted means (standard deviation).
Coefficient represents the mean variation in participation rate for an increase of one patient listed, adjusted for EDI (IC95%).
The bold p values represent the difference between groups. Values in bold are the adjusted mean values of cancer screening participation rates (SD) in both groups.
95% CI, 95% confidence interval; GP, general practitioner.
Regarding activity burden indicators, the total number of listed patients (p = 0.77) and the total number of female patients (p = 0.26), had no influence on the screening participation percentage.
In multivariate analysis (Table 3), the only remaining independent factor is the performance of cervical smears by GPs (adjusted difference of means: 1.71, p = 0.0204).
Coefficient represents the mean difference in participation rate between GPs performing Pap smears versus not, adjusted for gender and EDI (IC95%).
Coefficient represents the mean difference in participation rate between GPs female versus GPs male, adjusted for the variable “GPs performing Pap smears” and EDI (IC95%).
The bold p value represents the difference between groups.
Discussion
This is the first robust French study linking cervical cancer screening participation rates to GPs' characteristics. These data could not be found with sufficient evidence in the literature and were a necessary preliminary for the stratification of randomization in the ongoing PaCUDAHL-Gé screening trial. Cervical cancer screening participation rates over 2 years in the target population were independently increased if GPs declared to perform themselves cervical smears in their practice. However, the size of this effect is small and not sufficient to reach a necessary threshold of participation to lower the incidence of cervical cancer. Moreover, in multivariate analysis, the effect of the gender of the GP, generally described in the literature, was not found significantly associated to the percentage of participation to cervical cancer screening. We will carry out a new study with a 3-year follow-up to confirm this finding.
We found that 53% of GPs declared performing cervical smears themselves. This rate is comparable close to the national rate of 50%, 20 which geographically varies from 46% in the region of Paris to 83.6% in the county (département) of Saone-et-Loire. 9
The cervical cancer screening participation rate was higher when women receive care from GPs who perform cervical smears, rather than depending on a gynecologist for screening. This outcome demonstrates that primary care physicians can play a statistically significant role in screening programs based on Pap tests, but clinically irrelevant when screening is not organized on a national level. Gynecologists are performing the great majority of smears in France, but their numbers are drastically decreasing. 27 French health authorities instigate GPs and midwives to take over this health delivery service. For this reason, they encourage GPs to train to perform smears if they are not skilled.
We demonstrated that the motivation of GPs to promote cervical cancer screening participation by performing smears themselves has a significant influence, but we found that the size of this effect is small. At least, it is insufficient to reach the necessary thresholds of participation to influence the decrease of cervical neoplasms.
The organization of mass screening increases participation rates compared with the usual French opportunistic screening. 9,16,18 –20,28 However, almost half of GPs are not performing cervical smears and motivating economically deprived women or those with low education levels appears to be difficult. 24 Moreover, there is still an important number of women who are not willing to undergo a gynecological examination, which is partly related to the barrier of embarrassment regarding sexual issues in the relationship between GPs and their patients. 22,29 The objective of the ongoing PaCUDAHL-Gé cluster randomized screening trial is to compare the proposition by the GP of a usual Pap smear (with the cervical sampling performed by him- or herself or by another health professional) to a self-sampled HPV test in all under- or unscreened female patients.
Limitations
This study is robust and has a high level of evidence, thanks to the comprehensiveness and the accuracy of the SIAM claim database and the extremely high response rate to the telephone survey of the entirety of the GPs in the research area. By eliminating the GPs who had less than 100 listed female patients, we cleaned out from our database those who were not carrying out a primary care practice.
As first limitation, the cervical cancer screening participation rate of 43.3% in this study cannot be considered as representative of French participation rates in general. The dataset encompassed only 2 years. This duration was sufficient to find out independent GP characteristics explaining screening participation rates in their female patients and this was the primary need to define the randomization stratification levels in the PaCUDAHL-Gé study. A 3-year time frame, matching the French guidelines, is necessary to consider cervical screening participation percentages. Regarding the external validity of screening participation percentages, French Flanders is not France, and the setting was chosen for the PaCUDAHL-Gé trial because of an already supposed low rate of participation and an important incidence of cervical neoplasms.
The major risk of bias in this study is due to the survey procedure. GPs were asked by telephone a binary question: “Do you perform cervical smears yourself in your surgery?” yes or no. Rare GPs who had a very scarce activity in carrying out smears answered in accordance to their feelings sometimes yes and sometimes no. Answers were not double checked, by instance verifying in cytology laboratories the list of the GPs who were referring smears for interpretation. We believe that the influence of these GPs on the general trend of the outcomes is not a sufficient bias to modify the main results.
As last limit, the model takes into account individual characteristics of the GPs (gender, performance of smears, number of listed patients, number of female listed patients in the screening population), which reflects individual variance. The hierarchical mixed model operates the GP's individual level and the geographical level. Nonetheless, other geographical characteristics such as the availability of gynecologists or individual characteristics of the GP not taken into account might influence the results. 20
Conclusion
Cervical cancer screening has proven worldwide to be an effective method of reducing the incidence and mortality of cervical cancer. This article demonstrates that the performance of cervical smears by the GP is associated with increased screening participation rates, although insufficiently to reach the necessary participation thresholds. An organized cervical cancer screening program on national level is supposed to be implemented soon in France. In this environment, the effect of the commitment of primary care physicians in to lower the incidence of cervical cancer and its specific mortality still has to be demonstrated.
Footnotes
Acknowledgments
The authors wish to thank Elise GERS and Malek DIB for their patience and their efficacy monitoring the PaCUDAHL-Gé trial. The authors also wish to acknowledge Ghislaine LIEKENS, Laurent DUPLESSY, Eliane VANDERGHOTE, and Thérèse DEVIENNE-ROLLIN, from the CPAM of Flanders, for the extraction of our dataset from the SIAM-ERASME claim database. In addition of course, the 16 GP residents who carried out the telephone survey: Margot BADELON, Pauline BEAUVALLET, Ludovic CEROL, Marianne DELSERT, Axel DESCAMPS, Lynda DONAT, Marie FRANCKE, Anissa HINDI, Perrine KUCZERA, Claire LALOY-DEGRAEVE, Maxime LAMIRAND, Hélène LANGIN, Fanny PIGNOLE-SERMAN, François QUERSIN, Camille SANTANDREU, and Estelle SOUERES.
This study is a preliminary study of the PaCUDAHL-Gé trial. It was granted by the French Ministry of Health (PREPS: LIC-14-14-0615, 12/19/2014) and sponsored by the University Hospital of Lille. It was approved by the French Agency for the Safety of Health Products (ANSM, 2015-A01331-48, 10/06/2015) and by the Ethics Committee North-West III of Caen (2015-23, 02/03/2016). The registration number in
Author Disclosure Statement
No competing financial interests exist.