
Abstract
The obstetrician/gynecologist frequently serves as the primary care physician for women. Specialty-specific guidelines vary in screening recommendations for lipid disorders; women's health practitioners often follow recommendations to screen at age 45 in the absence of other risk factors. However, 2013 American College of Cardiology/American Heart Association cholesterol guidelines recommend screening at age 21 to capture those at risk of cardiovascular disease and allow for early intervention with lifestyle and, in the most severe cases, evidence-based statins. We discuss the care of women who primarily benefit from screening: those with familial hypercholesterolemia (FH), those with the metabolic syndrome (MetS) or polycystic ovary syndrome, and those with hypertriglyceridemia. Those with FH have elevated low-density lipoprotein cholesterol from birth and a propensity for premature coronary heart disease. Early recognition of FH can allow risk-reducing interventions, as well as identification of additional affected relatives. Early detection of metabolic variables, such as in the MetS and hypertriglyceridemia, can lead to an enhanced focus on physical activity and heart-healthy diet. Finally, we discuss a practical approach to lipid management and review concerns regarding drug safety. Our objective is to provide a current overview of cardiovascular risk factor optimization that women's health practitioners can use in identifying and/or treating patients at risk for cardiovascular disease and diabetes.
Introduction
C
Attention to lipid disorders is also important because women seek primary care from ob-gyns. Between 2007 and 2010, surveys found that approximately 44% of preventive care visits for nonpregnant women 18 years or older were to their ob-gyn. 8 Ob-gyns are more likely to take an adequate and complete obstetrical history than internal medicine physicians. 9 Several pregnancy-related diseases are significant ASCVD risk factors, on par with smoking. 10,11 Pregnancy-induced hypertension is found to increase the risk of hypertension (odds ratio [OR] 1.7) and dyslipidemia (OR 1.55). 12 Preeclampsia is associated with more than two- to ninefold increase risk for ASCVD death (with vs. without severe features), 13,14 while gestational diabetes increases the risk for myocardial infarction (MI) (OR 2.07) and hypertension (OR 2.92). 15 If provided an adverse obstetrical history, internal medicine physicians are much more likely to implement appropriate lipid and glucose screening and management than ob-gyns. 9 This highlights the need for further education for all who provide primary care.
Teaching and clinical recommendations for ASCVD risk reduction have been gender skewed. There is underrepresentation of women in cardiovascular clinical trials. 16 More recent efforts to include women in ASCVD prevention studies have been associated with a reduction of the gender gap in ASCVD preventive care. 17 In turn, the new lipid guidelines provide specific risk calculations and clinical guidance. For example, the ACC/AHA risk estimator is beneficial for women by including stroke in its determination of ASCVD risk, as more women die annually from stroke than MI. 18,19 The risk calculator includes for the first time a separate equation for African American individuals, which is significant because, at similar ages, African American women have higher rates than non-Hispanic white women of stroke and heart attack.
The ACC/AHA cholesterol, risk assessment, and lifestyle guidelines 20 place a strong emphasis on lifestyle as the foundation for preventive efforts. These include recommendations to engage in aerobic activity three to four times a week for 40 minutes, to consume a diet rich in vegetables, fruits, and whole grains, and, for those with hypertension, to reduce sodium intake. 21 This is especially encouraged for those younger than 40 years of age with elevated lifetime risk. The guidelines further endorse statin-benefit groups based on evidence from high quality, randomized controlled trials (RCTs) and meta-analyses of these RCTs. Statin use is recommended for individuals with clinical atherosclerotic heart disease (including stroke and peripheral vascular disease as well as obstructive coronary disease), those who have diabetes between 40 and 75 years of age with low-density lipoprotein cholesterol (LDL-C) 70–189 mg/dL, and those with primary elevations of LDL-C ≥190 mg/dL. This latter group includes women with familial hypercholesterolemia (FH). The ACC/AHA 10-year risk estimator, a web-based risk calculator, is recommended for women 40–75 years of age who do not have one of the above high-risk indications to determine whether statin therapy is appropriate. The guidelines found evidence for net benefit of statin use when the 10-year ASCVD risk is estimated to be 7.5% or more. 22 In women 20–39 years of age, a separate lifetime risk estimator is available to guide prevention discussions on a healthy lifestyle to address issues such as abnormal lipids, diabetes, obesity, and hypertension. It is not used to prescribe statins. Those with FH do not require risk estimation due to their high lifetime exposure to LDL-C ≥190 mg/dL.
Current ACOG guidelines recommend screening for lipid disorders in patients with risk factors and routinely in women over age 45. 3 This is the same strategy recommended by the USPSTF and the VA/Department of Defense guideline statements. 1,2 We are concerned that a delayed screening strategy fails to address those with genetic lipid disorders, the metabolic syndrome (MetS), and other women who would particularly benefit from early diagnosis and therapy. As discussed below, there is strong evidence that women with primary elevations of LDL-C ≥190 mg/dL, usually due to FH, derive cardiovascular benefit from early initiation of statin therapy to lower the strikingly elevated levels of LDL-C. Furthermore, those with metabolic risk factors, often with underlying insulin resistance, benefit from understanding the ability of lifestyle change to reduce all five components of the MetS, a precursor to early diabetes and CHD. Using the ACC/AHA approach, which addresses screening for women from age 21, we endorse management guidelines for all women's health clinicians, including the ob-gyn, beginning at this age (Figs. 1 and 2). These algorithms are age based. For women aged 21–39 years, Figure 1 provides guidance for primary prevention, secondary prevention, and those with elevated LDL, including indicated use of the lifetime ASCVD calculator. Figure 2 details management for women 40–75 years old. This population includes high-risk women, defined as those with prior ASCVD events, LDL >190 mg/dL, and diabetes. Lower risk women are those with LDL <190 mg/dL and without diabetes or previous cardiovascular events who may still benefit from primary prevention. Guidance is provided to calculate women's 10-year ASCVD risk and additional factors that may facilitate the decision to pursue statin therapy. Bidirectional arrows highlight the importance of integrating the patient's personal care heuristics and preferences. This informs choice because the immediate absolute risk reduction with medication is small, and there are side effect and cost considerations.
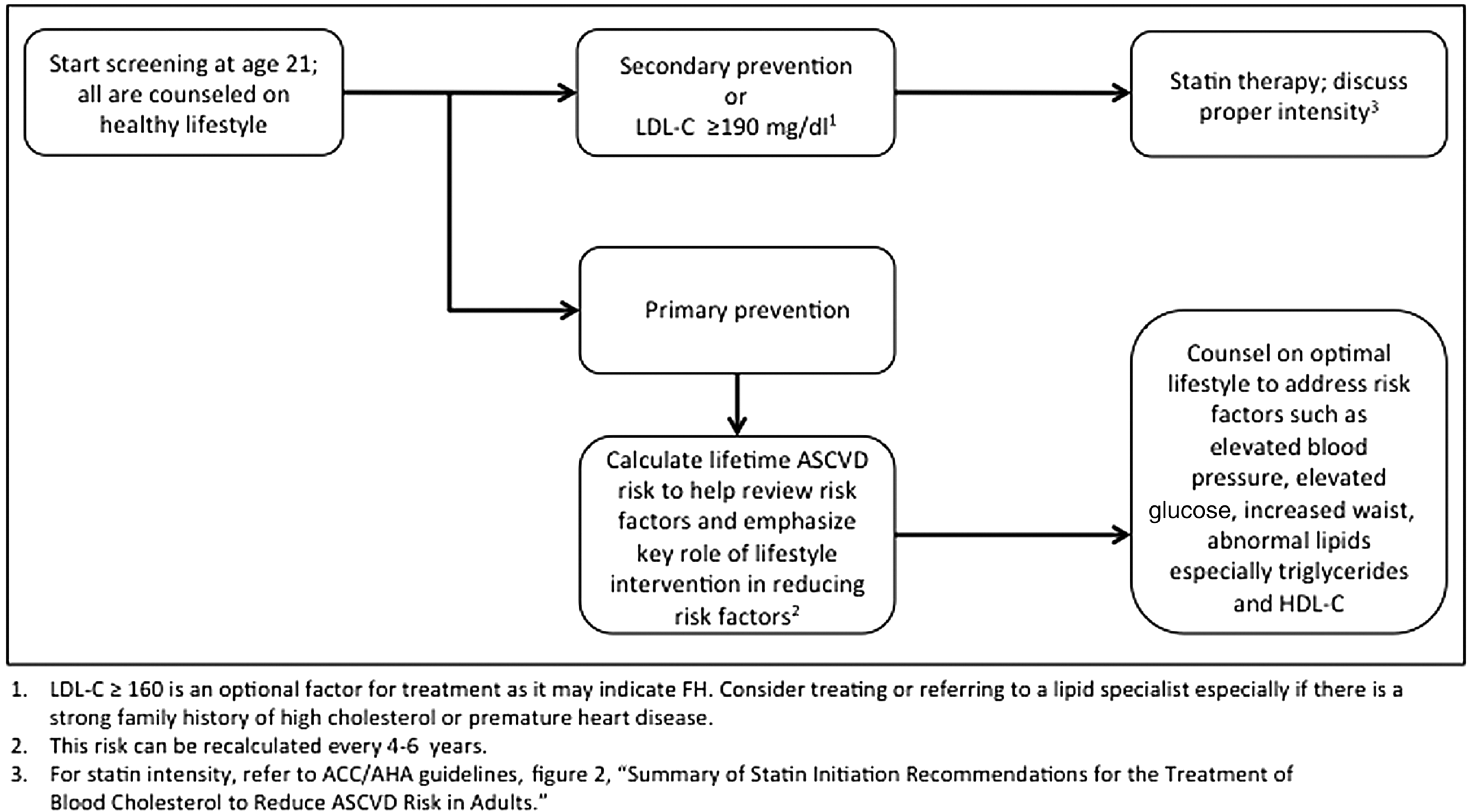
Approach to ASCVD risk assessment among women 21–39 years old. ASCVD, atherosclerotic cardiovascular disease.

Approach to ASCVD risk assessment among women 40–75 years old.
Special Populations
Familial hypercholesterolemia
FH is a common genetic disorder that results in severe elevations in LDL-C with a greatly increased risk for premature coronary disease. Patients with FH may have no risk factors other than a markedly elevated total cholesterol and LDL-C. Young women often transition their care to an ob-gyn by age 20. Many, in the absence of major medical problems, see their ob-gyn exclusively for screening and primary care, especially during their reproductive years. FH can be easily detected in this population by ordering a simple and inexpensive standard lipid panel implicit in screening all women.
FH is one of the most common genetic diseases. It is often underdiagnosed and undertreated. 23 Heterozygous FH (HeFH) affects more than 10 million persons worldwide. 24 It occurs in more than one of every 250 adults in the United States (US). 25 When a first-degree relative of a woman with FH is screened, the likelihood of identifying a similarly affected individual is as high as one in two. This enhanced ability to find other affected family members with this treatable disorder is a strong supportive reason for screening at age 21. Clinicians who provide medical care to young women should be aware of the main features of FH.
FH results in severely elevated serum cholesterol due to inadequate LDL-C clearance. FH can occur due to many different mechanistic defects in the low-density lipoprotein receptor (LDLR) gene function. 26 It is transmitted in an autosomal dominant or codominant pattern. The vast majority of patients with elevated LDL cholesterol have inherited one defective gene (HeFH). Although mutations in LDLR are responsible for ∼85% to 90% of clinical cases, the FH phenotype is also seen with defects in the apolipoprotein (Apo) B and proprotein convertase subtilisin/kexin type 9 (PCSK9) genes. 24 Multiple gene defects, some yet to be discovered, are responsible for producing the FH phenotype.
FH should be suspected when LDL-C is >190 mg/dL in adults (those older than 20 years of age) and >160 mg/dL in children or adolescents. A strong family history of premature ASCVD (men <55 years or women <65 years of age) and/or presence of characteristic physical findings such as tendon xanthomas in a young adult are suggestive findings. While detection of a causative mutation is informative, it is not necessary for diagnosis. A negative genetic test does not exclude FH. Cascade screening, a process for identifying people carrying a genetic condition, is the most cost-effective strategy to diagnose new cases of FH. In cascade screening, all first-degree relatives of affected patients undergo screening for FH with a lipid panel. 27 First-degree relatives of all individuals identified through this process should subsequently be screened.
When untreated, patients with FH typically have LDL-C levels between 190 to 400 mg/dL. The lifelong burden of high LDL-C levels results in a greater than 20-fold increased lifetime risk for premature cardiovascular disease. 28 Untreated women have a 30% risk of a coronary event by the age of 60 years. 29
For women with FH, 10-year ASCVD risk estimation is unnecessary. Aggressive treatment with LDL-C lowering medication is indicated. 30 The guidelines recommended high-intensity statin therapy defined as achieving at least a 50% reduction in LDL-C as first-line therapy. 31 All patients should also be counseled on diet and lifestyle modifications to reduce ASCVD risk. Despite treatment with maximally tolerated statin therapy, many patients with FH do not achieve an adequate response. 32 In these cases, additive therapy, with ezetimibe and/or a PCSK9 inhibitor may be considered for optimal management. 33 Those with clinical lipid expertise may be especially useful in the management of these complex medication regimens.
Overall, patients with FH experience a risk reduction of 76% with statin therapy. 34 When treated with potent statin-based regimens, the risk of MI is not different from the general population risk. Unfortunately, and most importantly, only 20% of patients with FH are diagnosed, and even if diagnosed, very few receive appropriate treatment. 26 Early identification of women of reproductive age has unique benefits. Pregnancy and lactation holidays are less detrimental with timely initiation of statin therapy in these women's lives, ideally years before childbearing. 35 Women with a known diagnosis of FH are able to receive preconception counseling and appropriate recognition of their pregnancies as high risk. If occult or previously identified ASCVD is present, they are able to seek antepartum guidance from a cardiologist who specializes in the care of pregnant women. FH without significant existing cardiovascular disease is not a contraindication to pregnancy, but requires surveillance afforded by capturing this cohort clinically.
Metabolic syndrome
Women fare much worse than their male counterparts when they have multiple metabolic risk factors (RR 5.90 vs. 2.39). 7 Some have called these clustered metabolic factors the MetS. A number of diagnostic criteria have been proposed by several professional groups. The World Heart Federation and the International Association for the Study of Obesity proposed a consensus definition with the following features: elevated blood pressure, high fasting glucose, increased waistline, low high-density lipoprotein cholesterol, and high triglyceride levels. 36 The diagnosis is made when three of these five elements are present.
MetS is increasing worldwide in parallel with the obesity epidemic. In the United States, the prevalence of the MetS from 2003 to 2012 was reported as 33%. 37 Childhood and adolescent obesity has increased (13.9% 1999–2000, 17.2% 2013–2014), which parallels the prevalence of the MetS. 38 Among U.S. children aged 12–19 years, the estimated prevalence of MetS was 1 in 10; among overweight/obese children, prevalence was 1 in 3. 39 Metabolic derangements and their consequences affect U.S. populations early in life, underscoring the significance of early identification.
MetS is associated with weight gain and insulin resistance. It is also highly associated with polycystic ovary syndrome. Deleterious lifestyle factors play a strong role in development of MetS. Factors associated with MetS include older age, female gender, heavy alcohol intake, and decreased physical activity. Weight gain (>5%) is more associated with MetS in normal weight subjects at baseline. 40,41 In particular, an elevated waist-to-hip ratio and insulin resistance contribute to development of the MetS, thought to be via elevated free fatty acids and circulating adipokines. 42 –44 These metabolic disturbances lead to vascular damage and greater risk for a cardiovascular event.
One benefit of MetS as a clinical construct is in its easy recognition. Blood pressure is routinely measured. Elevated waistline can be measured during any clinical encounter at the level of the iliac crest parallel to the ground. The remaining three criteria can be measured by widely available blood testing.
MetS doubles the risk of coronary artery disease and increases the risk of diabetes fivefold. 45 At any level of LDL-C, MetS greatly increases the risk of a coronary event. Individuals with clustered features of MetS are at higher risk for major coronary events and benefit from statin use more than those with isolated lipid derangements (RR of major event with statin use 0.48 vs. 0.86). 46 In the JUPITER primary prevention trial, metabolic factors increased the risk that statin use would hasten new onset diabetes by 5.4 months. 47 However, the reduction in vascular events or deaths avoided by statin use is substantial and exceeds the new cases of diabetes.
All the MetS variables improve with increased physical activity, a healthier diet with avoidance of sugar sweetened foods and drinks, and weight loss. A small amount of weight loss can make a large difference in metabolic variables and the risk of subsequent ASCVD. 48 Replacing red meat with white meat, fish, legumes, or eggs is associated with lower risk of incident MetS. 49
By emphasizing improved nutrition, regular physical activity and avoidance of weight gain, the ob-gyn is in a prime position to influence risk of MetS and its ASCVD sequelae. Patients also may be motivated by the impact on the long-term health of their children. Abnormal maternal nutritional states, both under- and overnutrition in pregnancy, contribute to a greater risk of obesity in offspring through epigenetic modifications that affect metabolic processes that may carry through to adulthood. 50
Hypertriglyceridemia
Although isolated, severe hypertriglyceridemia with fasting triglycerides above 500 mg/dL is rare, it is noteworthy because of the adverse effects of estrogen and pregnancy if not recognized. Hyperlipidemic pancreatitis with triglyceride levels that exceed 2000 mg/dL can occur when a woman with an underlying genetic cause for hypertriglyceridemia is given an estrogen-containing contraceptive or becomes pregnant. The clue is a fasting triglycerides level ≥500 mg/dL. Indeed, for those with severe elevations, nonfasting lipids can alert the clinician as well. An international statement presented good evidence that fasting is not routinely required for determining lipid panels. 51 This may greatly benefit patients who have afternoon appointments and for whom fasting would present a hardship. Current guidance is that if a nonfasting triglyceride level is above 200 mg/dL, then the lipid panel should be repeated fasting after 8–10 hours of water and pills, but no food. 52
Mild hypertriglyceridemia is treated with lifestyle improvements, but severe hypertriglyceridemia needs to be evaluated for dietary causes (excess dietary sugar or alcohol), drugs (estrogens, steroids, retinoic acid), diseases (diabetes, hypothyroidism, liver or kidney disease), or metabolic states such as pregnancy. If severe hypertriglyceridemia is found, removing secondary causes, initiating appropriate dietary therapy, and considering drug therapy (fibrates, omega 3) may be necessary to prevent hyperlipidemic pancreatitis.
Proposed Approach
Early identification of the at-risk patient allows early intervention. However, only 5.4% of patients older than 45 years who presented to their ob-gyn for preventive care between 2007 and 2010 received recommended lipid screening. 8 In recognition of pregnancy as a cardiovascular stress test, closer monitoring with annual assessment of lipids is recommended by ACOG for women with a history of preeclampsia who gave birth preterm (<37 weeks gestation) or who developed recurrent preeclampsia. 53 When this history is elicited, appropriate screening does not invariably follow. 9 Even so, these screening methods do not capture women younger than the age of 45 years with elevated serum glucose or lipids who may not have had previous pregnancies or pregnancy complications. 54
Four groups of women may be prescribed statin therapy: women with LDL-C >190 mg/dL, women 40–75 years old with diabetes and LDL >70 mg/dL, women with previous heart attack or stroke, and women 40–75 years old with an estimated ASCVD 10-year risk >7.5%. Four large-scale, primary prevention RCTs support the use of statins in at-risk postmenopausal women: AFCAPS/TexCAPs, MEGA, JUPITER, and HOPE-3 (Table 1). 55 –58 The ob-gyn office is in a critical position for identifying these women who can benefit from primary prevention and engage them in a risk discussion to foster shared decision-making. Because there is strong evidence for benefit in women with LDL-C >190 mg/dL or those with ASCVD, the use of the 10-year ASCVD risk estimator is not indicated in these women.
ARR, absolute relative risk; CV, cardiovascular; CI, confidence interval; HDL-C, high-density lipoprotein cholesterol; hsCRP, high sensitivity c reactive protein; LDL-C, low-density lipoprotein cholesterol; TC, total cholesterol.
Lipid-Lowering Agents and Lifestyle Modification in Pregnancy
Women considering pregnancy, those at risk of getting pregnant, and women who are pregnant should be aware that cholesterol and triglyceride levels rise after the first trimester. In those women of reproductive age for whom treatment with statins is warranted, reliable contraception should always be used. Formerly, statins were classified as category X and ezetimibe was a category C medication for use in pregnancy. The FDA has abolished this classification system for all medications in favor of a risk discussion and clinician judgment with an informed patient, such that medications are no longer discussed in terms of pregnancy category. 59 The context for the indicated discussion and clinical judgment for the use of statins, and other lipid-lowering drugs, in pregnancy is informed by limited data.
Water-soluble statins, such as pravastatin have not shown specific teratogenicity. 60,61 Thus, pravastatin is currently under study to reduce the adverse obstetrical outcome of preeclampsia, including recent publication of a pilot RCT. 62 Results of such future studies of water-soluble statins may change practice in select pregnant women. At this time, standard guidance indicates statins should not be used in pregnancy or during breastfeeding. Therefore, when pregnancy is desired, current guidance, based on expert opinion, remains to discontinue the use of any statin for at least 1 month before attempting conception and resume lipid drug therapy after pregnancy and breastfeeding are completed. All women should be encouraged to join ongoing registries if they take or have taken lipid-lowering medication during pregnancy.
As noted above, pregnancy in women with an elevated triglyceride level prepregnancy, may develop increasingly higher levels of triglyceride in the second or third trimester of pregnancy that can greatly enhance the risk of hyperlipidemic pancreatitis. 63 These severe elevations of triglyceride with pregnancy are most likely to develop in women with a genetic triglyceride abnormality who respond to higher levels of estrogenic hormones with striking elevations of triglycerides that peak in the third trimester. 52 Triglyceride elevation in the first trimester of pregnancy is also a risk factor for preeclampsia and gestational diabetes. 64,65 The ob-gyn should counsel women with abnormal lipids to implement lifestyle interventions before they undertake pregnancy. If a nonfasting triglyceride is >200 mg/dL, a fasting lipid panel can identify those women with triglycerides 500 mg/dL or higher. They should be counseled to reduce sugar sweetened foods and drinks, white flour carbohydrates and alcohol, while increasing physical activity. Triglyceride levels >1000 mg/dL require more intensive efforts, including dietary fat restriction. 66 Many clinicians are not aware of the striking beneficial effect of daily physical activity to lower triglycerides and other MetS abnormalities. This should be strongly emphasized to facilitate decline in triglyceride levels. Monitoring weight, steps, and dietary components is now possible with free applications for smartphones that enhance lifestyle management. Since hypertriglyceridemic pancreatitis leads to serious morbidity and possible mortality, in those with fasting triglycerides 800 mg/dL or more early in pregnancy, counseling from a physician with lipid expertise should be considered to avoid markedly higher values in subsequent trimesters. 67 Medication may be necessary to treat and/or prevent acute hyperlipidemic pancreatitis, which can be a lethal obstetrical condition. 63
Safety Considerations with Lipid-Lowering Agents
An important issue for women given statins is an increased risk for new onset diabetes. This is especially true with high-intensity statins such as atorvastatin 40 and 80 mg or rosuvastatin 20 or 40 mg daily. Patients who start high-intensity statins should be counseled to avoid weight gain. This is important because a new diagnosis of diabetes occurs primarily in those who already have risk factors for developing diabetes. The factors include weight and blood sugar abnormalities such as a BMI over 30, fasting blood glucose ≥100, hemoglobin A1c ≥6%, or MetS. Those with one or more of these factors are more likely to progress to diabetes. This occurred almost 6 weeks earlier in the statin group than in the placebo group. 47 A large secondary prevention trial showed no increased incidence of new onset diabetes for those with zero to one of these diabetes risk factors as contrasted with a 24% increased incidence in those with two to four risk factors. 68 New onset diabetes in the setting of statin use is an important part of the risk discussion before initiating therapy, although the indications for statin use remain the same.
Musculoskeletal complaints are also concerning in those women given statins. Although many RCTs, including some of the trials in Table 1, have not shown differences in creatine kinase (CK) elevations, myopathy, or rhabdomyolysis with statin use, other data have shown increased rates in muscular symptoms. 69 Risk factors for statin-associated myopathies include advanced age, lean body habitus, vitamin D deficiency, Asian ancestry, alcohol consumption, trauma, high-intensity exercising, especially for long distances, hypothyroidism, and a personal or family history of muscle disorders. Some of these factors are correctable; they should be considered in any woman presenting with muscular symptoms with statin use. If unexplained, severe muscle symptoms or fatigue develop, the statin should be stopped immediately and the possibility of rhabdomyolysis should be addressed. This can be confirmed with a CK value. Also, progressive weakness should prompt cessation of a statin until the cause can be determined. Usually, if the weakness is due to the statin, recovery occurs within a 2 to 3 week drug holiday. If mild to moderate muscle symptoms develop during therapy and persist, even if CK values are normal range, the statin should be discontinued until symptoms can be evaluated and other causes determined. Reinitiation with either a reduced dose or with another statin may be useful once muscle symptoms resolve. Muscle symptoms with one statin may not occur with another, so a low dose of a different statin may be trialed. The ACC/AHA guidelines provide an algorithm for management of those with statin-associated muscle symptoms. 20
The safety profile of nonstatins, ezetimibe, and PCSK9 inhibitor drugs have been examined in RCTs. 70 –73 Ezetemibe is now generic and more extensively studied. There is the possibility of transaminitis with use of ezetimibe. The ACC/AHA cholesterol guidelines recommend baseline transaminases before initiation. 20 If given with a statin, monitoring of liver function tests every 3 to 12 months may be considered. Ezetimibe should be discontinued if liver function tests are greater than three times the upper limit of normal. As of early 2018, the use of the newly FDA approved PCSK9 inhibitors has not been studied in specific circumstances such as pregnancy and lactation. In women outside these unique health statuses, there are two large-scale clinical trials supporting PCSK9 inhibitor use. They were shown to be beneficial when added to maximally tolerated statins in high-risk women who have had a MI and additional high-risk features. 73,74 Since, at this time, both cost and limited availability are important barriers to use, consultation with a lipid expert to help review the potential for net benefit may be helpful if PCSK9 inhibitors are considered.
Conclusions
More than ever, ob-gyns and other women's health practitioners have an increased incentive to identify women in their reproductive years who are at risk for premature ASCVD. Current ACOG screening guidelines may not routinely detect patients with HeFH, MetS, hypertriglyceridemia, or other at-risk women. Patients benefit greatly from early diagnosis and appropriate interventions before age 45. Providers should inquire about a family history of high cholesterol and/or premature CHD that could identify those with FH as benefits of early screening accrue to both high-risk individuals identified and close relatives with a similar genetic condition. Furthermore, recognition of those with elevated triglycerides, such as those with MetS abnormalities, may not only identify those rare individuals at special risk with estrogen therapy and pregnancy that could lead to hyperlipidemic pancreatitis but also allow a focus on lifestyle change that can improve risk factor burden over the life cycle. Lifestyle interventions remain the foundation of ASCVD risk reduction; however, as this commentary demonstrates, women's health practitioners should also have a good working knowledge of statin intervention. In the setting of discordant guidelines, diverse practices, and gaps between pediatric care and later reproductive years, the authors endorse initial lipid screening as recommended by the 2013 ACC-AHA cholesterol guidelines for any woman equal to or older than the age 21 years who has not already undergone screening with a pediatrician or previous physician.
Key Points
ASCVD causes significant morbidity and mortality among women but may be underrecognized and undertreated, particularly among reproductive-aged women.
Obstetrician gynecologists often serve as the primary care providers for women and should initiate lipid screening at age 21.
Women's risk assessment is achieved with a thorough history, including attention to obstetrical and family history, and use of ACC/AHA calculators.
Lifestyle remains the foundation of risk reduction.
Statins are indicated in high-risk women with clinical ASCVD, women with LDL-C greater than 190 mg/dL, women 40–75 years old with diabetes, and LDL-C between 70 and 190 mg/dL. Statins are also indicated among women 40–75 years old with an estimated 10-year ASCVD of 7.5% or greater after a risk discussion to consider the potential for benefits and adverse effects.
Nonstatins, such as ezetimibe and PCKS9 inhibitors, may be used by lipid specialists for very high-risk patients with an inadequate response to maximally tolerated.
FH is a common genetic disorder associated with markedly increased risk for premature ASCVD that can be easily detected and effectively treated.
MetS is characterized by elevated blood pressure, high fasting glucose, increased waistline, low high-density lipoprotein cholesterol, and high triglyceride levels, all of which respond to lifestyle changes.
Hypertriglyceridemia is important to identify, especially among women, because of the associated adverse effects of estrogen and pregnancy that can contribute to the risk of pancreatitis.
Statins and LDL-C lowering nonstatins are generally well tolerated, but current guidance does not recommend their use during pregnancy or breastfeeding at this time.
Footnotes
Author Disclosure Statement
No competing financial interests exist.