
Abstract
Background:
The authors analyzed data from the Hungarian Myocardial Infarction Registry (HUMIR) to examine the potential impact of gender on the treatment and 30-day and 1-year mortality of patients with myocardial infarction (MI).
Materials and Methods:
The National Registry of Myocardial Infarction included 42,953 patients between January 1, 2013 and December 31, 2016; 19,875 of whom were diagnosed with ST-elevation myocardial infarction (STEMI) and 23,078 with non-ST-elevation myocardial infarction (NSTEMI). The proportion of women was 39% and 41.9% in the two groups, respectively. Logistic regression analysis was performed adjusting for age, the year and month of hospital admission, smoking, as well as for five concomitant diseases and anamnestic data. We found that the odds ratio (OR) of performing percutaneous coronary intervention (PCI) was influenced by age, the year of treatment, prior stroke, and peripheral artery disease (PAD) in both patient groups.
Results:
Gender had an impact on treatment in both cases; women had significantly fewer PCIs (OR = 0.86 confidence interval [95% CI: 0.77–0.95] in the STEMI group, OR = 0.75 [95% CI: 0.70–0.82] in the NSTEMI group). Age and PCI, PAD, and diabetes mellitus proved to be prognostic factors for 30-day and 1-year mortality in both groups. In the STEMI group, hypertension proved to be of prognostic value for both 30-day and 1-year mortality, whereas prior MI, stroke, and smoking only affected 1-year mortality. Similarly, in the NSTEMI group, prior stroke was also of prognostic value for 30-day and 1-year mortality, whereas prior MI, hypertension and smoking were only associated with 1-year mortality.
Conclusions:
The independent prognostic value of gender could not be proven for any of the MI types or follow-up periods. In conclusion, gender influenced the treatment of patients with MI but had no significant impact on prognosis in itself.
Introduction
E
This study aimed to analyze whether treatment, 30-day, and 1-year mortality differed among men and women using data from a large unselected population of patients with MI. Data were provided by the Hungarian Myocardial Infarction Registry (HUMIR), which includes clinical and treatment data as well as data related to clinical course.
Materials and Methods
This retrospective observational study examined the treatment of patients with MI and gender differences using data from the HUMIR. The HUMIR included 42,953 patients with acute myocardial infarction (AMI) during the period between January 1, 2013 and December 31, 2016. Altogether 19,875 of patients were diagnosed with ST-elevation myocardial infarction (STEMI) and 23,078 were diagnosed with non-ST-elevation myocardial infarction (NSTEMI). The registered patients with MI were 72.5% of total reimbursed cases by the insurance fund. Registry data were continuously compared with the National Health Insurance Fund of Hungary reimbursement data base. In 2016, 83% of reimbursed AMI cases were registered in HUMIR. The majority of nonregistered events were a complication of an intervention (e.g., noncardiac surgery). Details on the methodology of HUMIR were summarized in our previous publication. 5
This study investigated whether there were significant differences between genders in the proportion of percutaneous coronary intervention (PCI) performed at the time of the index event among patients with STEMI or NSTEMI, and aimed to identify potential factors associated with the observed differences using multivariate analysis. We also aimed to examine 30-day and 1-year all-cause mortality, and to explore factors affecting survival, including gender. Cutoff date for the survival was March 30, 2017; thus, a 30-day follow-up was available for all patients, whereas 1-year follow-up was available only for patients admitted to hospital before March 30, 2016. Analysis of 1 year mortality will be therefore restricted to patients admitted before March 30, 2016.
Descriptive information on distribution was provided as (median) ± interquartile range [Min–Max] for continuous variables, and as frequency (proportion) for categorical variables. The Wilcoxon and Kruskal–Wallis tests were used for comparing continuous variables, and the Fisher's exact and chi square tests for comparing categorical variables between the two groups. The number of valid cases (with complete data) are indicated everywhere.
Multivariate modeling was performed using logistic regression (all outcomes considered were binary), adjusted for five concomitant diseases and anamnestic data: diabetes mellitus (DM), peripheral artery disease (PAD), hypertension, prior stroke, and MI, as well as smoking, date of hospital admission (month and year), and gender. Coronary arteriography was evaluated during the acute phase. Normal coronary arteriography was defined by the operator. We applied spline regression to allow for the detection of a potential nonlinear effect of age. Outcomes are provided as odds ratio (OR) with a confidence interval (CI) of 95%.
Mortality data were obtained from the database of the Hungarian National Health Insurance Fund.
Results
Patient demographics and concomitant diseases
The distribution of patient groups by age, gender, diagnosis (STEMI or NSTEMI), coronary angiography, and PCI are presented in Table 1. The mean age of patients with NSTEMI was higher than that of patients with STEMI (both for men and women). The number of men in case of both types of MI was higher than that of women, and women were older in both patient groups. Coronary angiography and PCI were more frequently performed among men in both MI groups, with more substantial difference in the NSTEMI group.
Major Characteristics of Patient Groups
Continuous variables are presented as mean (median) ± interquartile range [Min–Max], categorical variables are presented as frequency (proportion). There were no missing data for age, coronary angiography and PCI; for the remaining variables, the number of cases is indicated.
NSTEMI, non-ST-elevation myocardial infarction; PCI, percutaneous coronary intervention; STEMI, ST-elevation myocardial infarction.
Coronary artery disease in the STEMI and NSTEMI groups
The extent of coronary artery disease (CAD) is summarized in Table 2. In the STEMI group, the extent of CAD (one-vessel or two-vessel artery disease) was similar between the two genders; however, normal angiography was significantly more common among women compared with men (3.1% vs. 4.8%). In the NSTEMI patient group, the prevalence of CAD was similar between men and women, with a higher prevalence of severe CAD among men, and a higher prevalence of normal coronarography among women. Coronary angiography was normal in one out of six female patients.
Coronary Angiography Findings in the ST-Elevation Myocardial Infarction and Non-ST-Elevation Myocardial Infarction Groups by Genders
We also examined the preferred route for coronary angiography. The prevalence of radial access was lower among women, in the case of both MI types, than among men: STEMI 86.9% versus 91.3%, NSTEMI 88.6% versus 92.4%. Complications related to PCI were of similar frequency in both genders with slightly higher percentage seen for women in both MI groups—STEMI: men 1.86%, women 2.29%; NSTEMI: men 2.03%, women 2.49%.
Prevalence of PCI and factors associated with PCI
In general, PCI was more often performed in the STEMI patient group than in the NSTEMI group (78.9% vs. 53.4%, p < 0.001). Multivariate analysis revealed that the year of therapy had a significant impact on the prevalence of PCI in the STEMI patient group (the OR for the intervention increased by 20%–30% annually). PCI was less likely to be performed in patients with prior MI, PAD, and stroke, whereas it was more frequent among patients with hypertension. The impact of age had an inverted U-shaped graph, with a peak at ages 55–60. Multivariate analysis also found that PCI was performed significantly less often among women (OR = 0.86 95% CI: 0.77–0.95, p = 0.005). The complete model is shown in Figure 1, and major ORs are given numerically in Table 3.
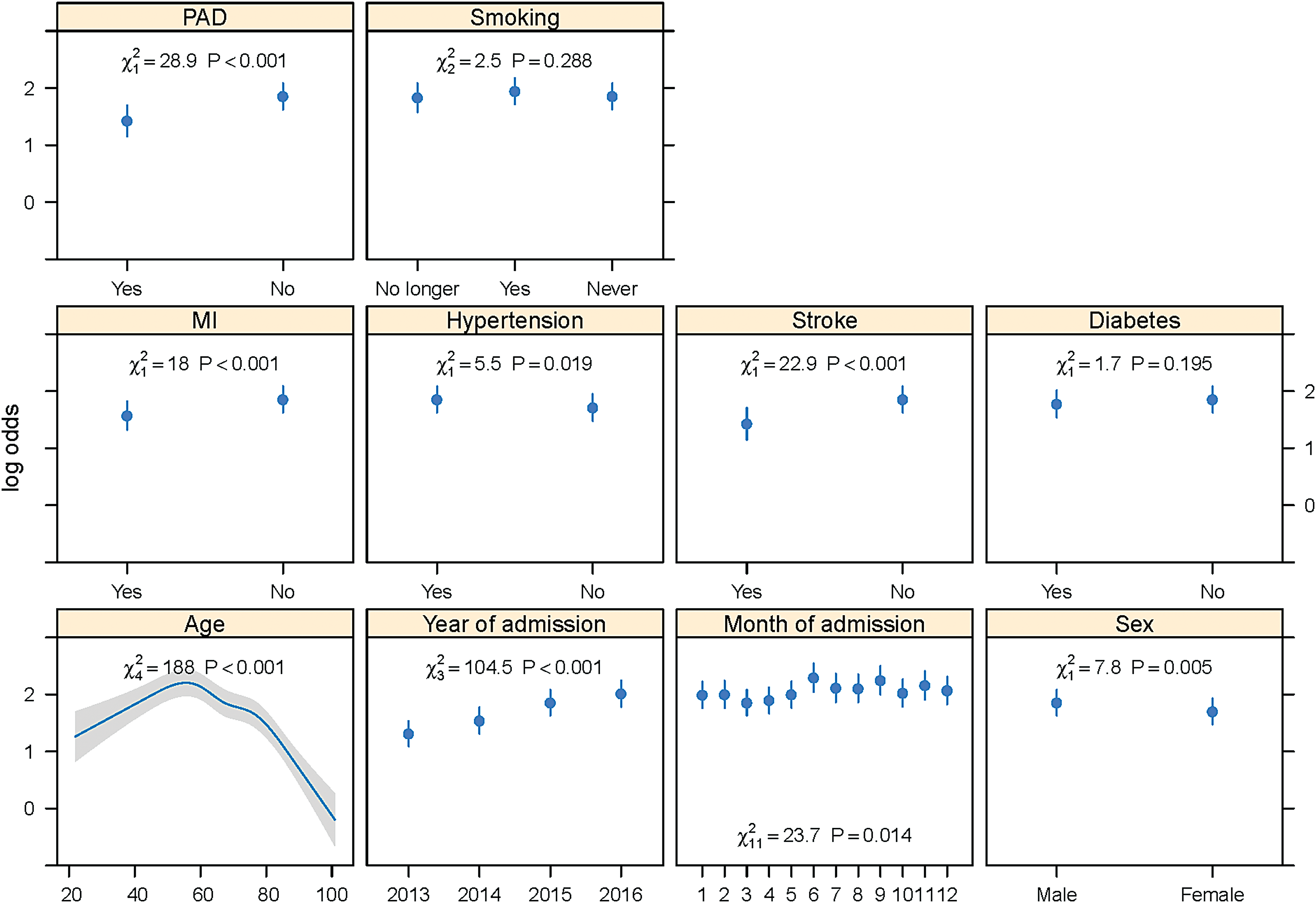
Effect of different variables on whether PCI is performed in STEMI patients in a multivariate logistic regression model. Each panel of the figure represents the effect of a variable by depicting the odds ratio for all possible values of the given variable (on a logarithmic scale), with 95% confidence interval, whereas the other factors are fixed at mean values (the continuous variables at their median and the categorical ones at the mode). PCI, percutaneous coronary intervention; STEMI, ST-elevation myocardial infarction. Color images available online at
Factors Associated with the Prevalence of Percutaneous Coronary Intervention in the ST-Elevation Myocardial Infarction Patient Group Using Multivariate Logistic Regression
CI, confidence interval; OD, odds ratio.
In the NSTEMI patient group, multivariate analysis showed that similar to STEMI patients, the year of therapy significantly affected the prevalence of PCI (however, the prevalence reached a plateau in 2015 in this group). Prior PAD and stroke also decreased the OR for the intervention, but hypertension and prior MI increased it. Age had an impact similar to that seen in STEMI. The impact of gender was also significant among NSTEMI patients, with a similar tendency: PCI was performed less frequently among women than in men (OR = 0.75 [95% CI: 0.70–0.82], p < 0.001). The impact of female gender on PCI was more pronounced among NSTEMI group. The complete model is shown in Figure 2, and major ORs are provided in Table 4.
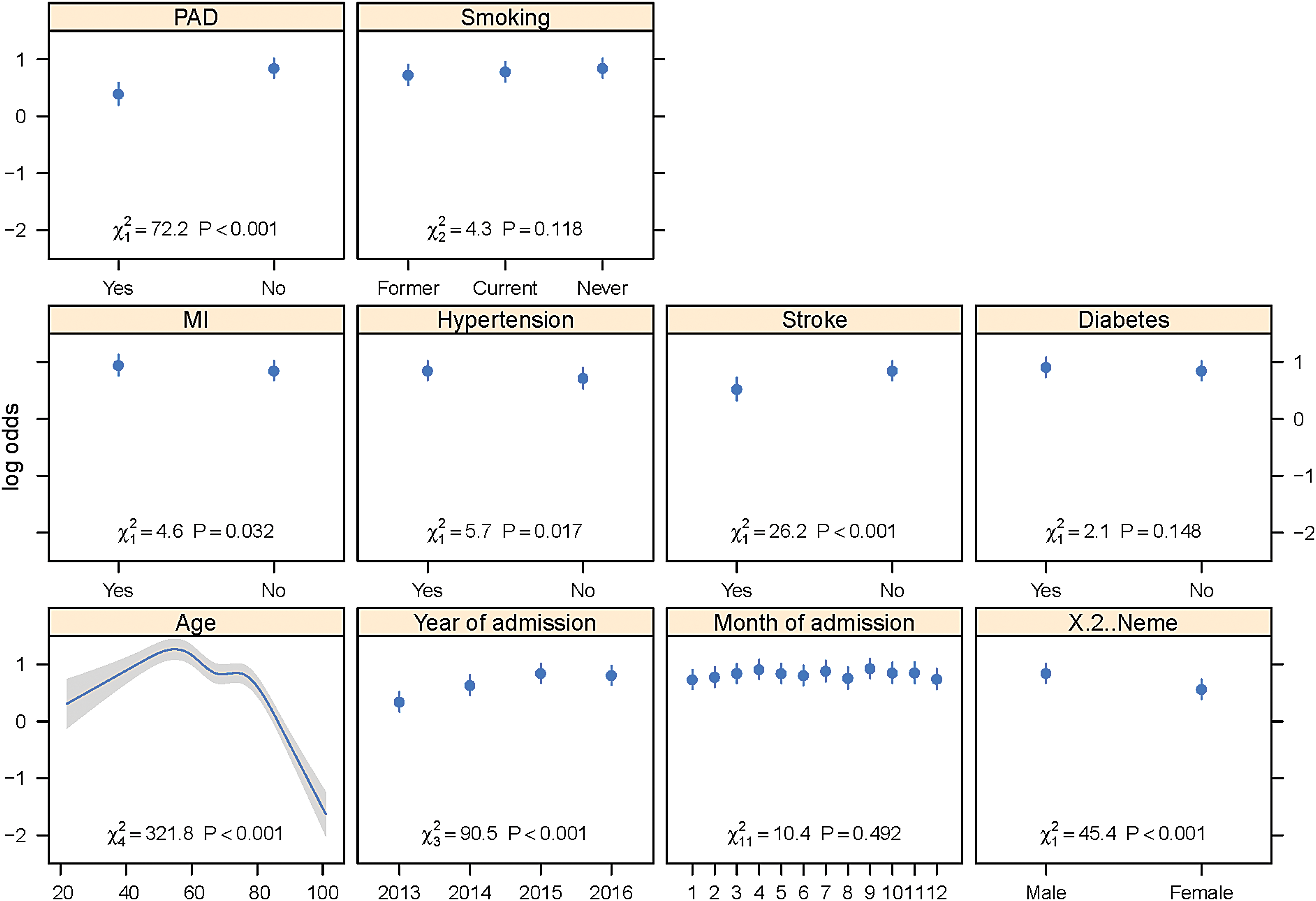
Effect of different variables on whether PCI is performed in NSTEMI patients in a multivariate logistic regression model. Each panel of the figure represents the effect of a variable by depicting the odds ratio for all possible values of the given variable (on a logarithmic scale), with 95% confidence interval, whereas the other factors are fixed at mean values (the continuous variables at their median and the categorical ones at the mode). NSTEMI, non-ST-elevation myocardial infarction. Color images available online at
Factors Associated with the Prevalence of Percutaneous Coronary Intervention in the Non-ST-Elevation Myocardial Infarction Patient Group Using Multivariate Logistic Regression
Of note, the difference in the effect of gender between STEMI and NSTEMI groups was nonsignificant (p = 0.0698) in a model that included interaction between STEMI/NSTEMI and all other predictor variables.
Medical therapy recommended at discharge
As for secondary prevention, a difference was seen in the STEMI group; the studied drugs were prescribed 4%–5.6% less frequently to women than to men. A similar tendency was not observed in the NSTEMI group (Table 5).
Frequency of Prescription of Certain Medications (as the Proportion of Discharged Patients with Prescription)
Mortality among men and women
The mortality of male patients was substantially lower than that of female patients both during the 30-day (STEMI: 9.9% vs. 16.2%, NSTEMI: 9.5% vs. 12.3%) and 1-year intervals (STEMI: 16.4% vs. 25.8%, NSTEMI: 20.6% vs. 26.2%). Among patients undergoing PCI, mortality rates were considerably lower than in the absence of PCI. Men undergoing PCI had lower 30-day mortality (STEMI: 7.3% vs. 11.3%, NSTEMI: 5.1% vs. 5.6%) and 1-year mortality (STEMI: 12.5% vs. 18.8%, NSTEMI: 12.7% vs. 14.4%) than women.
Multivariate analysis was performed to examine whether the differences in mortality are in fact gender-related or are only due to confounding.
In the STEMI patient group, 30-day mortality was significantly influenced by age, PCI, PAD, hypertension, and DM. Gender had no significant impact (p = 0.848) on 30-day mortality after controlling for all factors. One-year mortality was significantly influenced by the same as 30-day mortality and prior MI, prior stroke, and smoking in addition. Gender however did not have a significant impact during this follow-up period either (p = 0.768). Major ORs are presented in Table 6.
Factors Affecting Mortality in the ST-Elevation Myocardial Infarction Patient Group Using Multivariate Logistic Regression
In the NSTEMI patient group, 30-day mortality was significantly influenced by age, PCI, PAD, stroke, and DM. Gender (p = 0.185) had no prognostic value after controlling for all factors. One-year mortality was significantly influenced by the same as 30-day mortality and prior MI, hypertension, and smoking in addition. Gender did not have prognostic value in this case either (p = 0.1). Major ORs are presented in Table 7.
Factors Affecting Mortality in the Non-ST-Elevation Myocardial Infarction Patient Group Using Multivariate Logistic Regression
Discussion
Cardiovascular disease was traditionally considered to be men's disease for a long time. Epidemiological data, however, clearly show that this group of diseases is also the most frequent cause of death among women. 6 Data from the United Kingdom showed that 1 out of 10 deaths among women was attributable to CAD in 2010. 7 Ischemic heart disease in female patients has several characteristics both in terms of diagnosis and clinical manifestation, which require a special approach. The American Heart Association summarized the information available on the AMI of women in a separate scientific statement. 6 Some studies on the treatment of patients with MI found that among women, coronary angiography was performed less frequently, and the rate of revascularization was also lower among women. 8 –15 This study showed similar results: female patients were treated less often with PCI in both study group, and impact of female gender was more pronounced among NSTEMI group. Our data show that the proportion of patients with normal coronary angiography was higher among women than among men both in the case of STEMI and NSTEMI. This may be one cause of lower frequency of PCI among women. An analysis of the French National Cardiac Catheterisation Registry by Isorni et al. 15 reported similar observations. As for secondary prevention, we found that a few percentage lower proportion of women received optimal medical therapy than men; however, the clinical significance of this small difference is questionable. Hvelplund et al. 13 reported similar tendencies among postinfarction patients. When examining the prognosis of men and women, we found that both 30-day and 1-year mortality were higher among women compared with men. Nevertheless, multivariate analysis adjusting for other factors affecting prognosis (e.g., age, concomitant diseases, the form of therapy) showed no differences in 30-day or 1-year mortality between the two genders. Several authors reported similar findings. 4,11,12,16 –18
Bucholz et al. 3 summarized relevant studies in a meta-analysis and concluded that the differences in prognosis were due to the higher mean age of female patients and the larger number of concomitant diseases, whereas gender had no prognostic value on its own. In the SWEDEHEART Registry, 19 the prognosis of female STEMI patients below the age of 60 was worse than that of men. In a meta-analysis of 48 studies conducted by Bavishi et al., 20 the short-term prognosis of women was worse than that of men even after the correction of raw mortality data, but gender differences in mortality disappeared by the end of the 1-year follow-up period. As opposed to the mentioned findings, de Boer et al. 21 reported that both 1-year and 4-year mortality were higher among female STEMI patients than among men; however, they found no difference in mortality in the NSTEMI patient group.
The strength of our study is the extremely large sample size (a 3-year comprehensive study of a country with a population of 10 million and 42,953 MIs), which allowed for precise estimations and provided unselected real-world data. The most important limitation is the observational nature of the study, which always gives rise to the problem of whether all necessary confounders were controlled for, and thus whether the causal effects were correctly identified. Further limitation that we have no information related to some other important comorbidities (chronic obstructive pulmonary disease, cancer, atrial fibrillation, etc.) and to socioeconomic status, such as income or educational level of patients.
Conclusions
In summary, currently available data are inconsistent regarding the prognostic value of gender among patients with MI. Our data do not support the prognostic value of gender in itself among patients with STEMI or NSTEMI.
Footnotes
Acknowledgment
T.F. is supported by the ÚNKP-17-4-I-OE-779/71 New National Excellence Program of the Ministry of Human Capacities.
Author Disclosure Statement
No competing financial interests exist.