
Abstract
Background:
In Los Angeles County, the rates of sexually transmitted infections and diseases among African Americans represent a significant public health disparity. Older African American women are at particular risk as they are more likely to engage in high-risk sexual behaviors and report social isolation and loneliness than their younger counterparts. However, the literature on the relationship between sexual health and mental health in this group is limited. The purpose of this study was to use a community-based participatory research (CBPR) approach to better understand sexual health behaviors and mental health among African American women over 50 years of age who reside in South Los Angeles.
Materials and Methods:
This project was divided into two phases. Phase I (January–March 2017) of the project consisted of four dialog/focus groups (N = 45) (ages: 50–80; M age = 67). The purpose of Phase II (April 2017) was to present study results from Phase I to the community via a community-based conference, as well as gather feedback and generate discussion about the next steps for community prevention/intervention.
Results:
Women reported that they did not feel comfortable discussing sexual practices with their physician, partners, and friends. Most women identified depression, loneliness, and self-esteem issues as reasons for engaging in high-risk sexual behaviors. During Phase II, potential intervention avenues emerged to address issues such as lack of physician–patient communication, lack of community support, and dialogs about sex.
Conclusions:
The use of CBPR greatly enhanced our knowledge of the core issues surrounding sexual health and mental health among older African American women.
Introduction
D
Results from a survey study of individuals 50+ years of age, and who were at risk for STIs, revealed that 64.4% of men and 68.9% of older women had not received an STI test within the past year. 6 In contrast to popular belief, many older women remain significantly sexually active as they age, as well as engage in high-risk sexual behavior (e.g., lack of condom usage, increased sexual activity due to the advent of sildenafil [Viagra]). 7 –9 Women who no longer worry about becoming pregnant may be less likely to use a condom and to practice safer sex. 10,11
STD/STIs among older African American women
In the United States, African Americans are disproportionately affected by STDs/STIs relative to their population numbers as compared with Whites. 12,13 Epidemiological data have shown that STD/STI contraction is one of the highest rated health disparities among African Americans. 14 For example, in 2016, the CDC reported that the rates of chlamydia were highest among Blacks, with 5.6 times the rate among Whites (1125.9 and 199.8 cases per 100,000 population, respectively). The rate of reported gonorrhea cases among Blacks was 8.6 times the rate among Whites, and the rate of primary and secondary (P&S) syphilis among Blacks was 4.7 times the rate among Whites. Furthermore, the disparity for P&S syphilis was higher for Black women (7.0 times the rate among White women) than for Black men (4.6 times the rate among White men). Among people 50 years of age and older, newly acquired HIV infection rates were 15% among heterosexual men, and 23% among heterosexual women. 1
Few studies involve adults over 50 15 and even fewer include women. 16 This is particularly concerning for African American women, as older African American women are more likely to engage in high-risk sexual behaviors than their younger counterparts. 11,17 Furthermore, older women are also less likely to have ever had the topic of sexual health raised during healthcare visits. 18 In addition to these factors, women's ethnic/racial background and cultural upbringing may critically influence their interest in, participation, and expectations about sexual activity. 19,20 For example, studies of older African American women have found that factors contributing to high-risk sexual practices include trust in partner's fidelity, 21 lack of power in the relationship, or fear of violence. 22,23
Mental health well-being and sexual health behaviors
Mental health well-being is an important factor in one's overall sexual health, 24 but very few studies have looked at mental health well-being and sexual health in older adults. Studies have consistently demonstrated a relationship between risky sexual behavior, STI/STD prevalence, and mental health factors. 25 –31 It is estimated that 20% of people 55 years of age or older experience some type of mental health concern, 32 with depression being most prevalent. In a study conducted with African American women, psychological distress (i.e., recent depressive symptoms) negatively predicted self-efficacy to refuse sex in high-risk situations. 33 Depressive symptoms likely inhibit the ability to communicate skillfully, which is relevant in sexual communication situations, especially if such negotiations lead to conflict about condom use. 34
Los Angeles County: A community at risk
In Los Angeles County, African American women have five times the rate of chlamydia, nine times the rate of gonorrhea, and six times the rate of syphilis compared with Whites according to a 2015 report. 35 Among women over the age of 45, the rate of chlamydia incidence for African American women was 37.3% in comparison to 9.5% for Whites. 36 For gonorrhea, the incidence rate for African American women 45 years of age and older was 19.7% compared with 6.9% of Whites. As such, there is a need for more focused studies of this particular demographic as there may be regional specific differences. Studies of this cohort have been ignored due to low levels of participation, lack of opportunity, and trust barriers in medical and academic research. 37 –39
One method for addressing engaging the community in sexual health issues is through community partnerships. 40,41 Community-Based Participatory Research (CBPR) is a method that has been shown to be effective at capturing the underlying issues in the community that are important for community members and stakeholders. 42 –47 Utilizing CBPR provides this cohort an opportunity for engagement and equal representation in the research process. 48,49
The purpose of this two-phase project was severalfold. First, it aimed to identify factors that may contribute to the increase of STIs among African American women over 50 who reside in Los Angeles. As such, the goals of Phase I of this project were as follows: (1) Describe the impact of aging on sexuality and mental health well-being among African American women over 50; (2) Identify potential barriers to engaging in safe sexual health practices; (3) Identify gaps in service delivery in relationship to sexuality and sexual practices among older adults; and (4) Determine the existing resources available to promote sexual health and prevent STIs/STDs for older women in South Los Angeles. Second, we determined whether or not responses from our groups were consistent with those reported in previous literature, as well as identify any new themes that have not been previously reported. Third, and perhaps most unique to this study, is that we reported research study findings to the community (Phase II) to receive feedback before submitting for publication. Finally, the purpose of hosting the academic-community-partnered conference was to discuss next steps for what is needed that is specific to the Los Angeles community to prevent this disparity.
Materials and Methods
All research procedures were conducted in accordance with the Declaration of Helsinki and were reviewed and approved by UCLA Institutional Review Board. The planning group team was formed based upon the Circles of Influence Model developed by Jones et al. 50 (Fig. 1). The planning group consisted of the Principal Investigator, UCLA faculty members (n = 2), members from the Healthy African American Families Association (HAAF; n = 4), Pacific Region Oasis Clinic (n = 2), Los Angeles Women's Coalition on HIV/AIDS (n = 1), Bivens Consulting Group (n = 1), Fox Hills Ladera Healthy Families Association (n = 1), as well as members of the South Los Angeles community (n = 2). The planning committee met weekly to plan for Phase I of the project, biweekly during data collection, and then weekly for Phase II conference planning. The committee used a logic model approach to guide planning (Fig. 2). The logic model structure sets the parameters and expectations of the research program.

Circle of influence model. This model was adapted from Jones et al. 50
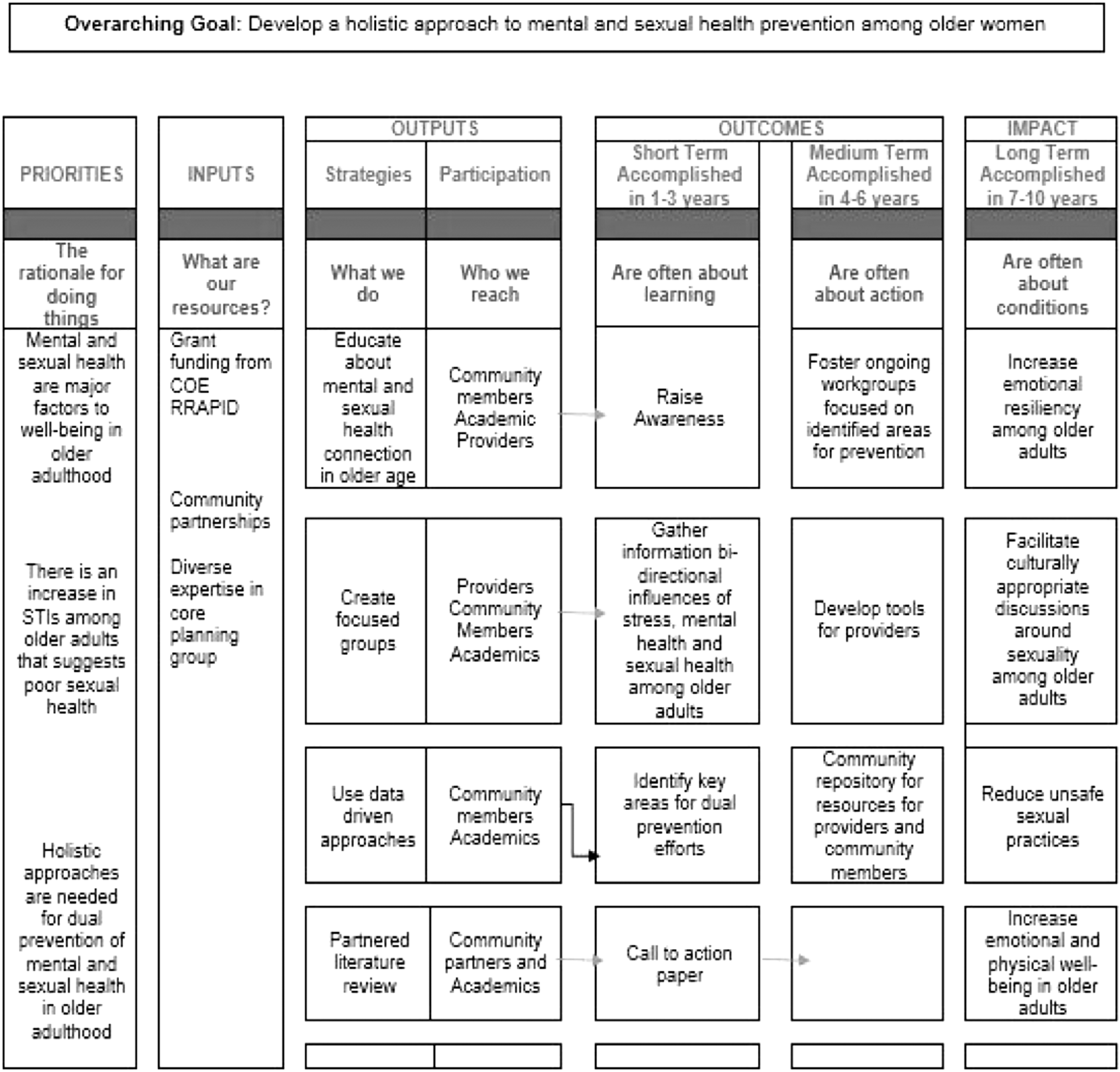
Project logic model. 51 Community-academic partnerships to promote sexual health through mental health and wellness among women over 50. COE, Centers for Excellence; RRAPID, Rapid Research Advances for Progress in Disparities.
Phase I: Dialog groups
Phase I of the project consisted of four dialog/focus groups, with 10–12 participants per group (age range: 50–80; M age = 67). Forty-five (N) women participated in total. Participants were recruited from HAAF as well as other community partners. The purpose of Phase I was to stimulate conversation about the relationship between mental health well-being and sexuality. Before the dialog group, participants were provided informed consent and allowed to ask questions about their participation. Next, the moderator and assistant moderator explained the dialog group rules (e.g., “Turn off cell phones,” “Do not interrupt a group member while speaking”). Each dialog group had a moderator, assistant moderator, and two designated notetakers. Each session was audio recorded for transcribing later. To ensure anonymity of study participants, each participant was given a pseudonym (i.e., flower name). Participants were compensated $25 at the conclusion of the dialog group. Figure 2 shows the logic model that was used to guide the group's planning.
Dialog group questions
Participants were instructed to refrain from self-reference in their response to questions and to instead think of women in their communities and circles. All dialog group questions began with the introduction “Do women who you know, or women like you……” Below were the six questions:
Feel comfortable about discussing sexual practices with their physician?
Have a conversation about use of protection with their partners?
Have conversations about sex (friends, family, partners)?
Think that physical changes that occur with age (e.g., menopause) impact sexuality?”
Think that mood might influence sexual behaviors?
Have access to STI/STD prevention and support services?
Data analysis
Trained research staff (n = 2; not part of the dialog groups) transcribed tapes. Transcribed tapes were examined with handwritten notes from the dialog group sessions to determine consistency across notetakers. The PI and the trained research staff independently coded themes across notes. Data were examined for intercoder reliability. We began with one full-length interview transcript and compared themes. At the end, each rater coded all four transcripts and if there were discrepancies we refined our coding themes until we were satisfied with the level of intercoder reliability (or agreement). This method has been suggested in other studies. 52 For themes that differed across staff, a collective decision was made on the final coding. Cohen's kappa was used to determine reliability of coding themes. Overall, there was substantial reliability of coding across raters (k = 0.85). 53
Results
Results for each question are presented in Figure 3. In general, most of the women reported discomfort about discussing sexual practices with their physician. The majority of responses centered around lack of rapport with the physician and believing that the physician did not think that it was necessary to address sexual health practices because of their age. Other responses included that talking about sex went against cultural norms and that they were afraid to broach the conversation. Examples of these responses included the following: Rose: “Cultures are set in their ways. They don't talk about anything.” “If it's not killing them then there is nothing wrong.” Dandelion: “Sometimes doctors aren't comfortable asking women about sexual practices. Doctor told me before that it is not necessary to test me for STDs. They might not feel comfortable in talking about things so were not comfortable.” Freesia: “I would never ever use a male doctor. If it's a female, I feel like I can express myself. Write everything down and bring it to the doctor because they don't care.”

Study results.
Regarding conversations about the use of protection with partners, there was a bimodal distribution of responses such that 38% of the responses indicated regular conversations about the use of protection, whereas 41% of the responses indicated that the conversation about protection with partners did not occur, with a majority reporting that their partners complain about the use of condoms. Examples of responses were as follows: Freesia: “My friends are not married and act like none of that exist. All the men that she has been with this year don't wear a condom. A lot of them lie. A guy took her to a motel room and he couldn't put one on. Some of us enforce condoms and some of us don't.” Sunflower: “They claim they don't feel anything with the condom.”
Seventy-two percent of responses indicated that women were not having conversations about sex with friends, families, or partners, but about one-third felt that menopause was an acceptable topic. When asked about physical changes that occur with sexuality, a majority of responses (i.e., 55%) reported that age-related physical changes were associated with depressed and/or irritable mood as well as losing sex drive. A critical question pertained to the relationship between mood and sexual decision making. Seventy-two percent of the responses reported that women engaged in unsafe sex because of low self-esteem and depression. Thirty-five percent of the responses stated that women had sex because they felt lonely and wanted someone to make them feel desired. Violet: “It goes back to self-esteem. We feel needy if we don't love ourselves. We're not self-appreciating—causes a lot of what people do—filling void inside.” Iris: “I think emotion is everything. We need to incorporate mental and sexual health on questionnaires.” Lily: “I have a friend who is lonely and depressed and is attracting bad men. She's making these hasty decisions. Mentally if she had been healthy she would have seen him coming from around the corner.” Sunflower: “Women need to feel loved. Vibrators don't come with arms.”
The final question pertained to access to STI/STD prevention and support services for women their age who are entering sexual relationships. While most women were able to identify services in the community once someone receives an STI/STD diagnosis, they were not able to identify support groups for women who are entering relationships with new sexual partners. The women expressed a desire to have “sister circles” and workshops for topics such as “How to use a female condom” and “What STD tests should you ask for?.” The women also expressed interest in having this integrated as part of their faith-based communities, since their churches and networks within the church were an integral part of their circle.
Phase II: Community conference
The purpose of the community conference was to present the study results from the dialog groups to the larger community as well as receive feedback and determine the next steps for community prevention/intervention. The conference was held at a well-known community location for a half day and advertised through word of mouth and flyers. Approximately 95 conference attendees were present. The community conference was structured such that it would include presenting the research results, presentations from a panel of experts on the topic, and dialog with the audience about what they would like to see as “next steps” in the community. The planning committee collectively decided on panel experts who would address the key issues that were found through the results. The conference moderator is a pastor in the community. An expert in mental health discussed self-esteem in women over 50 as it pertains to body changes and sexual decisions. A retired registered nurse, Chair of the HIV/AIDS/STIs ministry for the local community church discussed the uses of protection and STD testing. The final expert has worked in the HIV-positive community for the past 30 years. Below are specific recommendations that stemmed from discussions between the audience and panel: To address lack of physician–patient communication: Clinics should include a checklist to be given to women before their doctor's visit that include questions about sexual activity and mental health. This would prompt the physician to bring up the topic and create a dialog about sexual health and mental health. To address the lack of community support: Many of the audience respondents felt that “Sistah circles” devoted to this topic would be helpful as a means of support within the community. These circles would decrease feelings of social isolation. These circles could be made available through the church or community centers that are frequented by community members. To address dialog about sex: Including men into the conversation was highlighted as being key to beginning the dialog. Creating spaces for men and women to dialog about sex was thought to be critical to being able to have the conversation with potential partners about the use of protection and STD history.
Audience members were administered a survey providing valuable insight into the impact of the community engagement approach in sexual and mental health well-being. When answering questions regarding comprehension of research results, 96.1% of respondents agreed or strongly agreed that they learned from the research results and 94.1% agreed and strongly agreed to sharing results with community and networks. In questions relating to the panel discussion, 96.2% of respondents agreed or strongly agreed that panel members had knowledge and expertise and 90.3% agreed or strongly agreed that the panel was successful in discussing next steps in prevention of STI/STD transmission. In assessing the overall conference presentation, 91.3% agreed and strongly agreed that the conference was organized and 93.7% agreed and strongly agreed to attend future presentations. However, only 73.8% respondents were clear of future directions of research, indicating a need for intervention.
Discussion
The purpose of this study was to understand contributors to the increase of STIs/STDs among African American women 50+ years of age who reside in South Los Angeles. While our results were generally consistent with previous studies that have studied older women and sexuality, 54 –56 there were a few unique findings that emerged. Consistent with previous reports, 7,57 a majority of the women reported that their physician overlooked asking questions about their sexual health. Indeed, more than 65% of the responses indicated that physicians made explicit statements that it was not necessary to address sexual health practices because of their age. This concerning statistical observation is important since empirical studies have shown that women of all ages are especially vulnerable in the acquisition of STDs/STIs. 58 –60
Also consistent with previous reports, 11,61 a majority of the women had not discussed STIs with their healthcare provider, but would be comfortable doing so if there was good rapport. Other women discussed cultural norms with respect to being African American and the era of their upbringing, which they believed contributed to a lack of conversation. Many of the women felt that the physical changes that occur with aging (e.g., menopause) also contributed to a lack of desire for sex. With regard to mental health, some of the women felt that engaging in risky sexual practices stem from feelings of loneliness and wanting to feel desired by the opposite sex. Although there were no specific questions about partner infidelity, the women raised partner infidelity as a significant issue in their community. It was generally agreed upon that marital status or being in a committed relationship did not protect them against STDs/STIs.
One of the noteworthy strengths of the current study include bidirectional relationships that were formed between academic and community partners. Each member of the planning committee brought together knowledge and expertise that shaped the design of the overall study and dialog groups. Furthermore, we used logic models to help guide our planning and evaluation. Findings from Phase II provided ideas for intervention design and implementation. One potential intervention to increase the physician–patient dialog about sexuality is to include a checklist before the medical visit that includes questions about sexual activity and mental health. This is a relatively simple intervention that may be feasible in high-demand clinic settings. Support networks, particularly those that pertain to issues of sexuality, were also identified as lacking in the community. As demonstrated in this study, creating “Sistah circles” devoted to this topic was identified as a way to increase a network of support within the community. Including men into the conversation about sexuality was identified as a critical piece to the overall dialog. Similar to “Sistah Circles,” this could be achieved by having dialog groups with both sexes. Finally, interventions related to sexual health practices for older African American women should include mental health screening that have demonstrated validity for use in this population. Among older African American women symptoms of depression may go unnoticed in part by symptom severity, cultural descriptions, and manifestations of symptoms. 62 Future research should include testing these interventions in the community to determine feasibility and effectiveness.
There are limitations to the current investigation worth noting. First, women who volunteered to participate in the dialog groups may have been more comfortable with discussing the topic of sex compared with those who elected not to participate. Another limitation that might be important is the educational background of some of the women who participated and the absence of assessing for general knowledge of STDs/STIs (e.g., differences between STI and STD, how diseases are transmitted, and condom use). There were instances throughout the discussion when the moderators had to explain particular STDs/STIs. Finally, we did not break down sexual health issues according to age (e.g., 50–60 vs. 70–80). Future qualitative studies should examine specific disparities by age groups, rather than using global statements about “older women” or “women over 50.” These limitations aside, we believe that this study provides critical information with respect to disparities that occur in sexual health among older African American women. Healthcare providers do not always assess dating and sexual health in the older adult population. First-line healthcare professionals are in a position to assess the dating relationships of older patients and can ask targeted questions to determine if patients are engaging in potentially risky sexual practices.
Earlier studies have suggested that disparities in this community exist as a result of an array of social and structural determinants. 63 –66 Our results suggest that disparities in STI/STD acquisition largely stem from social determinants, such as those highlighted in this study, which include social support, social norms and attitudes, and lack of information about how to discuss these issues.
Conclusion
In sum, the incidence of STDs in the elderly population is significant for both newly acquired disease and for residual complications from preceding infections. 67 Considering that African American women are at high risk for these new infections, addressing sexual health and mental health in this cohort is important in preserving overall health in the older adult population, although studies of this nature rarely investigate issues surrounding sexuality and STDss in older adults. 67
Footnotes
Acknowledgments
This work was supported by the UCLA Behavioral Health Centers of Excellence RRAPID Awards funded through the California Mental Health Services Act (MHSA). The authors would also like to acknowledge the support of Drs. Kenneth Wells and Jeanne Miranda and the Center for Health Services and Society, Department of Psychiatry and Biobehavioral Sciences at the University of California Los Angeles.
Author Disclosure Statement
No competing financial interests exist.