
Abstract
Background/Objective:
Persistent instability in insurance coverage before and after pregnancy among low-income mothers in the United States contributes to delayed prenatal care and poor infant outcomes. States that expand Medicaid under the Affordable Care Act (ACA) make public insurance free for many low-income women regardless of parental or pregnancy status. Our objective is to analyze the effects of expanding Medicaid in Ohio on enrollment of pregnant women and receipt of recommended prenatal care. A key objective in the state is to address infant mortality as Ohio ranks above the national average and racial disparities persist.
Materials and Methods:
We used linked enrollment/claims/birth certificate data for women with Medicaid-paid deliveries/births, aged 19–44 years with months of last menstrual period (LMP) in calendar year 2011–2015 (N = 290,091). We used interrupted time-series analysis of enrollment prepregnancy and receipt of guideline-concordant screenings (anemia, asymptomatic bacteriuria, chlamydia, human immunodeficiency virus [HIV], and TORCH) and prenatal vitamins after versus before the expansion. We stratified by parity since first-time mothers would be impacted more.
Results:
We found almost a 12 percentage point increase in enrollment prepregnancy among first-time mothers compared with almost a 6 percentage point increase for parous women. We found significant increases in all screens and vitamins for both groups. TORCH screening increased 8 percentage points and receipt of prenatal vitamins almost 14 percentage points, by the end of 2015 for first-time mothers, compared with 5 and 4 percentage points, respectively, for parous women.
Conclusions:
Early enrollment and prenatal care for low-income women in Ohio could erode if the state's Medicaid expansion is altered.
Introduction
W
Ohio law requires every county to review the deaths of children. According to the 2013 review, >60% of Ohio's infant deaths are attributable to preterm birth and birth defects, 7 pregnancy outcomes that may be preventable through interventions in the prenatal and preconception periods. By some estimates, 6% of all Ohio mothers received late (third trimester) or no prenatal care during their pregnancies in 2013. 8 Although questions persist about the impact of prenatal care on pregnancy outcomes, the adequate and timely receipt of prenatal care has been associated with the reduced risk of low birth weight, stillbirth, early and late neonatal death, and infant death, as well as with maternal health behaviors linked with improved pregnancy outcomes. 9 –13
Although pregnant women are encouraged to schedule their initial prenatal visit during their first trimester, care ideally begins before conception and includes preventive care, counseling, and screenings for risks to maternal and fetal health. 14,15 Nationally, the timing of prenatal care entry varies greatly by race/ethnicity and insurance status, with rates of first trimester prenatal care initiation being highest for non-Hispanic whites and those with private insurance. 16
Lack of health insurance is associated with delaying or forgoing preventive health services and other medical care. 17 Before the Affordable Care Act (ACA), women in the United States faced unique challenges in obtaining or maintaining health insurance for numerous reasons, 18 including historical Medicaid eligibility rules that largely omitted women without dependent children, then qualified lower income women as eligible during pregnancy, but removed them 60 days postpartum. 19 A 2009 study documented that approximately one-third of first-time mothers experienced transitions in insurance coverage, most commonly moving from being uninsured before pregnancy to having Medicaid by the time of delivery. Moreover, these levels and patterns of coverage were largely unchanged since late 1990s. 20,21
Compared with higher income women, low-income mothers are more likely to be uninsured before becoming pregnant and to have three or more chronic diseases and/or related risk factors that could affect birth outcomes if left untreated or not managed appropriately. 22 Recent research on the pre-ACA period documented that 58% of women experience at least one change in insurance status in the 9 months leading up to and including delivery, whereas 55% of women with Medicaid at delivery experienced a coverage gap in the following 6 months; the authors called for analysis of the impact of the ACA in minimizing the adverse effects of such “churning.” 23
In 2014, Ohio expanded Medicaid eligibility under the ACA. Before this, Ohio's Medicaid program covered pregnant women up to 200% of the federal poverty level (FPL); parents were eligible if they were ≤90% FPL, and Ohio Medicaid did not offer coverage to nondisabled childless adults. 24 The expected effect of Ohio's expansion of Medicaid coverage to all adults ≤138% FPL is to increase the proportion of low-income women who deliver on Medicaid who have coverage that begins before pregnancy or early in pregnancy, thereby improving access to prenatal care. As pregnancy and delivery were covered for women up to 200% FPL in Ohio before the ACA, with coverage before pregnancy for some parents (≤90% FPL), we expect women having their first birth in the post-ACA period to be most affected by the Ohio expansion. Before the ACA expansion, these women would not have been categorically eligible for Medicaid before pregnancy.
From an economic perspective, the ACA Medicaid expansion made public insurance free for many childless women who would otherwise have been uninsured, reducing out-of-pocket costs for contraceptives and pregnancy-related expenses. Lower out-of-pocket costs for contraceptives should increase the quantity and/or quality used and, in turn, increase intendedness of pregnancy and reduce births. 25,26 A reduction in the costs of pregnancy-related expenses should lead to higher rates of prenatal and preventive care during pregnancy. 27
Earlier studies of Medicaid expansions suggest expected effects. Analysis of the Oregon Health Insurance Experiment found evidence of increased hospital, outpatient, and medication utilization, as well as increased compliance with recommended preventive care. 28 Studies have found evidence that state Medicaid expansions decreased uninsurance and delays in care seeking due to costs. 29 In addition, the ACA Medicaid expansion increased use of certain forms of preventive care and modestly improved self-rated health. 30 Our study is novel in examining the impact of the ACA Medicaid expansion on the likelihood that women of reproductive age take up Medicaid insurance at an earlier gestational age and receive timely guideline-concordant prenatal screenings and interventions during their pregnancy.
Materials and Methods
Data sources and study sample
The Ohio Department of Medicaid and the Ohio Department of Health granted permission for access to its electronic Medicaid enrollment and encounter records and birth certificate records, respectively. The study was reviewed and approved by Institutional Review Boards of the Ohio State University, Emory University, and the Ohio Department of Health. Personal identifiers were used to perform a well-documented iterative matching process between Medicaid administrative records and yearly Ohio Birth Certificates that involved both deterministic and probabilistic matching. 31,32 The match rate of women with a Medicaid-paid delivery claim to an Ohio Birth Certificate averaged 87.4% across study years. Indicators of health system utilization were generated from procedure, diagnosis, and drug billing codes recorded on inpatient and outpatient encounter claims for deliveries/births with any amount of Medicaid payment.
To capture pre- and postpregnancy information, encounters with a date of service 6 months before the date of last menstrual period (LMP) through 6 months postpartum were included for each birth. The source of LMP was the Ohio Birth Certificate. If LMP date was missing on the woman's record, the infant's gestational age at delivery was used to determine LMP (N = 23,255; 8.5%). If both LMP and gestational age at delivery were missing on birth records, LMP was calculated by subtracting 9 months from the infant's date of birth (<1%). Medicaid enrollment status was obtained from monthly administrative eligibility records. Record matching and data processing were completed in SAS 9.4 (Cary, NC).
From these files, we defined an initial study cohort as those deliveries/births paid by Ohio Medicaid during calendar years 2011 through 2016, aged 19–44 years and with months of LMP in calendar years 2011–2015 (N = 290,091). We then omitted from this cohort those with month of LMP in the last quarter of 2013 to assure that the analysis of women getting prenatal screens included only those whose first trimester occurred fully in the pre- or post-ACA periods. Our final study population equaled 274,541, comprising 155,778 women in the pre-ACA period and 118,763 women in the post-ACA period. Services were considered early in pregnancy if the service date was between LMP date and LMP date plus 16 weeks; we chose 16 weeks to account for services that occurred within the first trimester (within 12 weeks of LMP) and allowed for 4 additional weeks given that enrollment data are by month.
For the analysis of mean months and continuous enrollment during pregnancy, we omitted women with LMP in the last three quarters of 2013 to assure that the analysis considered only women whose pregnancy occurred fully in the post-ACA period, resulting in N = 245,355. We excluded younger teens since their eligibility for Medicaid/Children's Health Inisurance Program (CHIP) was not directly affected by the ACA expansion. Data on Medicaid enrollment for the last quarter of 2010 were used to assess enrollment before LMP of January 2011, and administrative encounter data through the second quarter of 2016 were used to assess early prenatal screens for those with LMP of December 2015.
Dependent variables
The outcomes studied include several measures of enrollment before and during pregnancy, as well as the receipt of early prenatal care. Specifically, we tested for effects on the following as indicators of reduced “churn” for women with Medicaid-paid deliveries: (1) enrollment prepregnancy, (2) enrollment in the first trimester of pregnancy, (3) number of months enrolled during pregnancy, and (4) continuous enrollment throughout pregnancy. In turn, we tested for effects on receipt of the guideline-concordant screenings early in pregnancy (including for anemia, asymptomatic bacteriuria, chlamydia, human immunodeficiency virus [HIV], and TORCH [a blood test that screens for a broad set of maternal infections that can be passed vertically to the infant during pregnancy, including toxoplasmosis, syphilis, measles, rubella, cytomegalovirus, and herpes simplex virus]) and receipt of prenatal vitamins within 12 weeks.
There is wide agreement that the timely receipt of these screens and prenatal vitamins is considered guideline-concordant prenatal care based on recommendations from one or more of the following, as documented in Table 1: (1) Centers for Disease Control and Prevention, (2) Institute of Medicine, (3) American Congress of Obstetricians and Gynecologists, (4) US Preventive Services Task Force (USPSTF), or (5) National Committee for Quality Assurance. 33 –37 We tested for significant differences in these screening outcomes for women in our study cohort with month of LMP in the post-ACA period compared with women with month of LMP in the pre-ACA period.
HIV screening was included in the TORCH screening codes as of January 2016; to some extent this affects the rates seen for women with LMP in the last quarter of 2015.
Source: Authors' summary of publically available information on recommendations and guidelines for prenatal care made by various professional associations and federal organizations.
ACOG, American Congress of Obstetricians and Gynecologists; HEDIS, Healthcare Effectiveness Data and Information Set; HIV, human immunodeficiency virus; LMP, last menstrual period; NCQA, National Committee for Quality Assurance; USPSTF, US Preventive Services Task Force.
Statistical analysis
We began our analyses by describing the observable characteristics of women with a Medicaid-paid delivery across the pre- and post-ACA periods in Ohio to reflect any variation in the enrolled population due to changes in eligibility criteria across the period. As the ACA made more women eligible preconception on the basis of income, rather than on the basis of parental status and income, we stratified our analyses based on parity or the number of times a women has carried a pregnancy to a viable gestational age (parity = 0 vs. parity ≥1).
Next, we used regression models and interrupted time-series to analyze changes in our outcomes of interest. This type of analysis uses data collected at multiple time points (monthly/quarterly) before and after an intervention to detect whether the intervention had a significantly greater effect on the trend than any underlying secular trend. 38 We estimated logistic regressions (or linear regressions as appropriate) and derived marginal effects of changes in the probability of timely screens/vitamin intake and enrollment measures.
In the regressions, we controlled for mother's age, education, race, marital status, parity, poor prior outcome, prior preterm birth, months enrolled during pregnancy, Medicaid category during pregnancy, previous Medicaid birth, obstetricians/gynecologists per 10,000 women (aged 15–44 years), Ohio regional code (Appalachian, rural, metropolitan, suburban, and missing), seasonality (using summer season as reference category), and father's education. Control variables were adjusted for these two subsamples of deliveries, parity = 0 and parity ≥1.
Results
We show our results in both tabular and graphical formats. Descriptive data in Figures 1 and 2 show an increase in all enrollment measures for both study populations. As would be expected with any new policy, it takes time for participation rates to increase and more women to enroll as eligibility expansions start. For example, the percentage of first-time mothers (women with parity = 0) enrolled prepregnancy increased from ∼27% in the last quarter of 2013 to ∼42% by the fourth quarter of 2014 and steadily increased to ∼48% in the fourth quarter of 2015 (Fig. 1). In the first quarter of 2013 (pre-ACA), a large percentage (77.5%) of first-time mothers were enrolled during their first trimester, and by the first quarter of 2015 this equaled 82.3%. The percentage of this group of mothers enrolled during their entire pregnancy increased from ∼29% to 49% over these quarters, but this percentage declined slightly by the end of 2015.
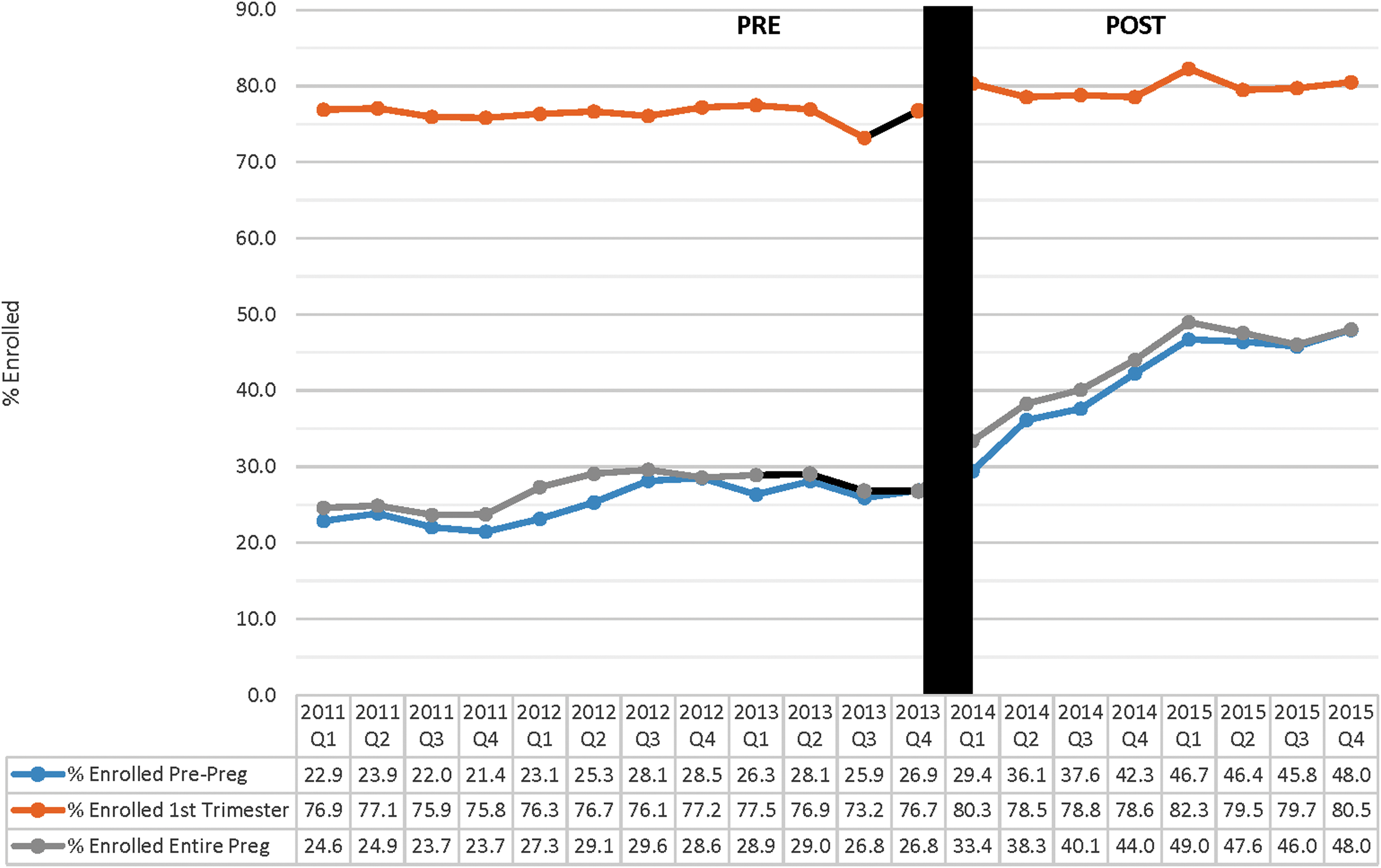
Percentage of women aged 19–44 years with Ohio Medicaid-paid delivery enrolled prepregnancy, first trimester, and continuously through pregnancy, first-time mothers (parity 0), pre- and post-ACA. ACA, Affordable Care Act.
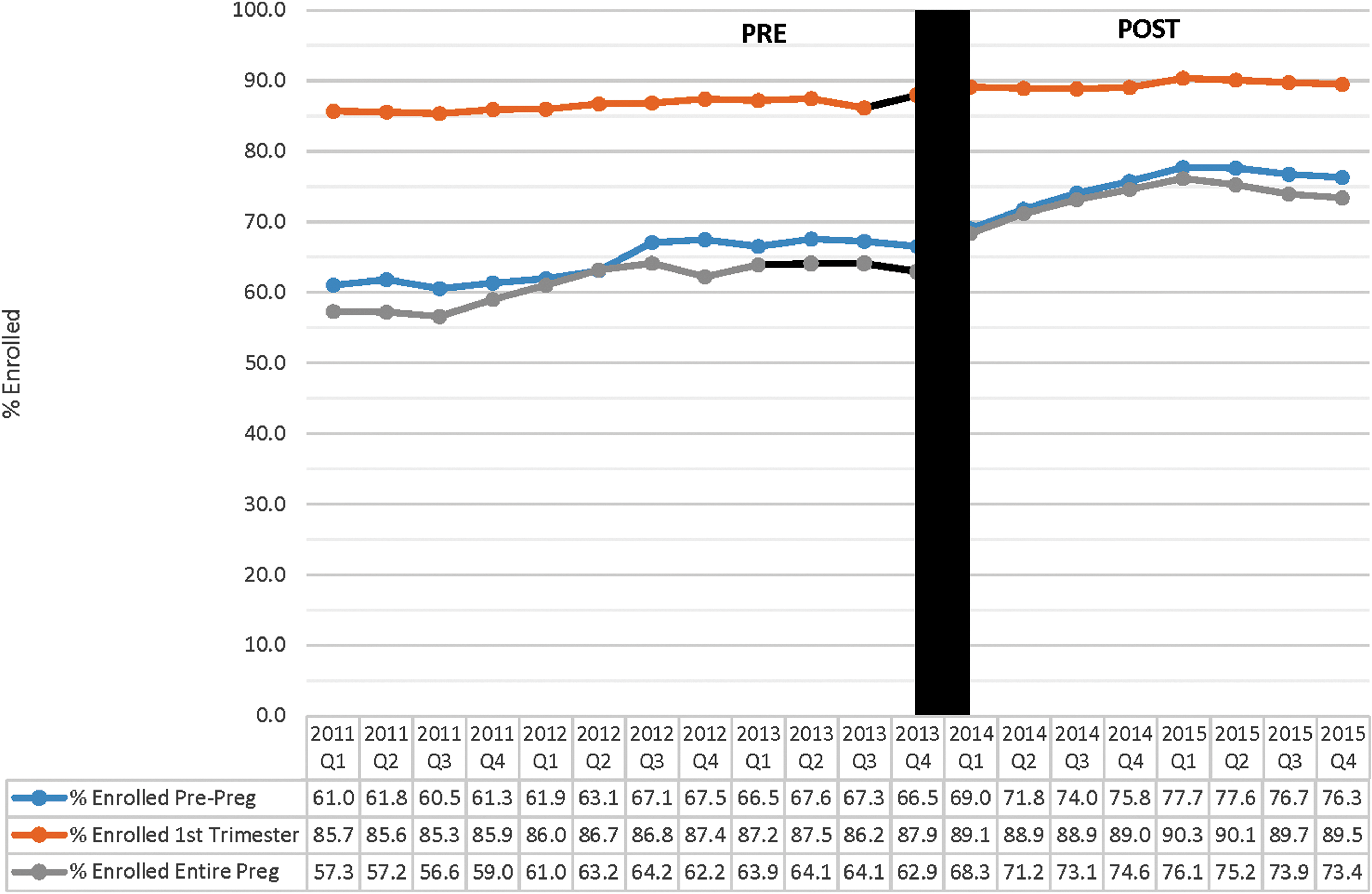
Percentage of women aged 19–44 years with Ohio Medicaid-paid delivery enrolled prepregnancy, first trimester, and continuously through pregnancy, parous women (parity ≥1), pre- and post-ACA.
Similar patterns are seen for parous women (those with parity ≥1) in Figure 2. For parous women, the percentage enrolled prepregnancy was higher at the end of 2013 (66.5% vs. ∼27% already noted) and increased through the first quarter of 2015 (77.7%), but declined slightly after that to 76.3%. Figure 2 indicates that the percentage of parous women who enrolled their entire pregnancy increased from ∼64% in the first quarter of 2013 to ∼76% in the first quarter of 2015. Although both first-time mothers and parous women enjoyed greater prepregnancy and first trimester enrollment, facilitating the provision of best reproductive health practice, there were slight declines in the latter part of 2015. We also noted that 52% of first-time Ohio mothers with Medicaid-paid deliveries were not enrolled in their entire pregnancy, even after the ACA expansion; in comparison, this applied to ∼27% of those having their second or higher birth.
In Figure 3, the descriptive data for timely screens are arrayed by LMP quarter for the full study population. These data indicate a clear upward trend in the post-ACA period in Ohio in the receipt of all screenings as well as vitamins. From the third quarter of 2013 to the fourth quarter of 2015, there were increases of 5.0 percentage points (anemia and chlamydia screening ≤16 weeks) to 5.4 percentage points (TORCH and bacteriuria screening ≤16 weeks). The receipt of prenatal vitamins among the full study population increased 1.9 percentage points over this period. Although the changes in trends for enrollment and receipt of timely screens could reflect the change in policy under the ACA, they could also reflect changes in the composition of women with a Medicaid-paid delivery in Ohio over the pre- and post-ACA period.

Percentage of women aged 19–44 years with Ohio Medicaid-paid delivery receiving guideline-concordant prenatal screens, pre- and post-ACA.
The descriptive data given in Table 2 show total and monthly counts of Medicaid-paid deliveries and the characteristics of these women in the study population. The total monthly sample in the pre-ACA period (N = 4720) was somewhat smaller than in the post-ACA period (N = 4948), consistent with the expanded eligibility criteria. Relatively more of the parous women came into Ohio Medicaid coverage for delivery, as their monthly enrollment increased from 3484 pre-ACA to 3754 post-ACA. Based on the data given in Table 2, the characteristics of the women in the Ohio study population are remarkably similar pre- and post-ACA. Only the age and eligibility categories changed by >2 percentage points. With respect to these changes, after the ACA, Ohio women with Medicaid-paid deliveries (whether it was their first birth or second/higher) were more likely to be >25 years old and, as would be expected, less likely to be eligible due to their pregnancy status.
Parity, number of Medicaid months, and OBGYN ratio used Student's t-test. The other characteristics used Pearson's chi squared test.
<0.01; b<0.05.
ACA, Affordable Care Act; NH, non-Hispanic; OBGYN, obstetricians and gynecologists; SD, standard deviation.
To further disentangle the effects of changes in the composition of the women with a Medicaid-paid delivery versus changes attributable to other policy provisions, we present the results of our multivariate analysis in the following section.
Marginal effects
We show the estimated changes in the probability of dichotomous outcomes and on the mean months enrolled post- versus pre-ACA (Tables 3 and 4) after controlling for the individual and area characteristics as already noted. We also controlled for any underlying monthly time trends independent of the ACA, as shown in the first columns of Tables 3 and 4. We noted that some of the underlying monthly trends for these prenatal care screens were negative. The effects of the ACA are measured by the 2014 and 2015 indicator variables shown in the remaining columns; these indicators equal “0” for any LMP in the pre-ACA period and equal “1” for LMP in 2014 and 2015, respectively. Since women with first births would not have been categorically eligible in the pre-ACA period, but newly eligible if ≤138% FPL in the post-ACA period, the changes seen for them are more likely due to the ACA Medicaid expansion than other policy changes aimed at improving quality of prenatal care. In the following text, we compare the results for first-time mothers to those of parous women.
Logistic regression marginal effects (percentage point changes).
Adjusted for mother's age, mother's education, father's education, race/ethnicity, marital status, months enrolled during pregnancy, Medicaid category during pregnancy, obstetricians/gynecologists per 10,000 women (aged 15–44 years), Ohio regional code, and seasonality.
Observations with LMP in quarter 4 of 2013 excluded.
<0.01.
Adjusted for mother's age, mother's education, father's education, race/ethnicity, marital status, obstetricians/gynecologists per 10,000 women (ages 15–44 years), Ohio regional code, and seasonality.
Observations with LMP in quarters 2, 3, and 4 of 2013 excluded.
Linear regression.
Source: Authors' analysis of 2011–2016 electronic Medicaid enrollment and encounter records and birth certificate records from the Ohio Department of Medicaid and the Ohio Department of Health.
Logistic regression marginal effects (percentage point changes).
Adjusted for mother's age, mother's education, father's education, race/ethnicity, marital status, poor prior outcome, prior preterm birth, months enrolled during pregnancy, Medicaid category during pregnancy, obstetricians/gynecologists per 10,000 women (aged 15–44 years), Ohio regional code, and seasonality.
Observations with LMP in quarter 4 of 2013 excluded.
<0.01.
<0.05.
Adjusted for mother's age, mother's education, father's education, race/ethnicity, marital status, poor prior outcome, prior preterm birth, obstetricians/gynecologists per 10,000 women (aged 15–44 years), Ohio regional code, and seasonality.
Observations with LMP in quarters 2, 3, and 4 of 2013 excluded.
Linear regression.
Source: Authors' analysis of 2011–2016 electronic Medicaid enrollment and encounter records and birth certificate records from the Ohio Department of Medicaid and the Ohio Department of Health.
Based on the interrupted time-series analysis, the marginal effects for first-time mothers with Medicaid-paid births in Ohio are given in Table 3. The marginal effects represent percentage point changes in the probability of each outcome. The increase in the probability that first-time mothers were enrolled prepregnancy equaled almost 12 percentage points by 2015 compared with almost 6 percentage points for those with prior births as given in Table 4. Important to the receipt of early prenatal care, the probability of being enrolled in the first trimester also increased for both groups of mothers. Being enrolled the entire pregnancy increases access to providers and, perhaps, continuity of care. As given in Tables 3 and 4, the probability of being enrolled the full pregnancy increased for both groups, but, again, was larger for first-time mothers. For these women, the probability of being enrolled in Medicaid continuously through their pregnancy increased by 6.3 percentage points by 2015, whereas for those with prior births, this increase was 2.2 percentage points.
Enrollment prepregnancy or earlier in pregnancy would mean women have better access to prenatal care providers. These findings suggest that the probabilities of the guideline-concordant prenatal care will increase. Overall, the results given in Tables 3 and 4 indicate significant increases in the receipt of all the guideline-concordant prenatal care (and vitamins) in both 2014 and 2015 post-ACA periods. This held for first-time mothers, as well as for those with prior births. For first-time mothers, the receipt of TORCH panel screening ≤16 weeks increased by 8 percentage points, and screening for chlamydia by almost 6 percentage points, both larger effects than for women with prior births. For those with prior births, the increases in these screens were 5 and ∼3 percentage points, respectively (Table 4).
Increases in screening for anemia ≤16 weeks were more comparable for the two groups of women. The increase in the receipt of prenatal vitamins among first-time mothers was markedly higher, equal to almost 14 percentage points by 2015, compared with an increase of 4 percentage points for those with prior births. We note that there was an increase in the probability of HIV screening for both groups of women in 2014 and 2015 relative to the pre-ACA period, but the increase in 2015 was smaller than that for 2014 for first-time mothers and flat for parous women.
Limitations
This study is not without limitations. As the health services utilization data are based on claims data, there is the possibility of misclassifying the utilization and/or receipt of particular types of services, with some variation in the use of particular codes according to the provider expectation of payment and setting of care. Provider trainings and interventions that focus on quality of care could also influence receipt of care, and although this is a topic of interest, it is beyond the scope of our research question. Although interrupted time-series analysis is valuable for evaluating the effectiveness of population-level health interventions and is increasingly used to evaluate policy interventions, it is most appropriate when there is a clear differentiation between the pre- and postintervention periods and when studying short-term outcomes that are expected to change quickly or after a clearly defined lag. We allowed for differentiation of the post-ACA effects by 2014 and 2015.
Interrupted time-series analysis can also be affected by time-varying confounders that change rapidly. We attempted to account for this limitation by incorporating seasonality into our models. Another limitation is the lack of data on changes in access and use of contraceptives pre- or postpregnancy and intendedness of births. Analysis of postpartum visits and contraception use among those with Ohio Medicaid-paid deliveries is being conducted for inclusion in a future article. We earlier noted that we imputed LMP for ∼10% of observations; we tested the analysis after omitting these observations and found the results to be robust in terms of the patterns and only small changes in the magnitude of effects. Finally, Ohio is just one of the states expanding Medicaid under the ACA. The findings of this study cannot be generalized to other states given the number of other contextual factors that can drive Medicaid enrollment and service utilization at the state level.
Discussion
Under the ACA, states could extend Medicaid eligibility to low-income women regardless of their parental or pregnancy status in the hope of addressing the persistent instability in insurance coverage before and after pregnancy seen among low-income women in the United States. 20,21,23 Once insured, providers and patients are better able to detect and address problems before, between, and earlier in pregnancy. Preconception care, or the improvement in women's health status before pregnancy, and interconception care, which focuses on improving women's health status between pregnancies, are increasingly seen as strategies for improving U.S. maternal and infant outcomes. 15,39 –41 The results shown here for Ohio provide early evidence that the expansion resulted in significant increases in Medicaid coverage prepregnancy and enrollment in Medicaid throughout pregnancy.
The results also indicate significant increases in those who received guideline-concordant screenings and prenatal vitamins early in pregnancy. The expectation is that these changes will lead to improved outcomes; we note that this analysis is part of a broader study of the Ohio expansion that will assess postpartum enrollment and utilization of services and, as more data become available, both maternal and infant outcomes.
Although these positive trends for Ohio are encouraging, there is room for improvement. In particular, the percentage of women receiving the guideline-concordant screens in the post-ACA period (Fig. 3) ranges from 46.7% to 62.4%, well below the 80.5%–89.5% of our study populations enrolled in Ohio Medicaid in their first trimester. This suggests that although the Ohio prenatal care provider system did respond to the newly enrolled pregnant women through improved rates of screening, other obstacles to the receipt of timely screens by Medicaid-insured women may present and warrant further investigation.
We note that the improvement in timely screenings was less pronounced for HIV screening than for the other prenatal screenings, which may be attributable to several factors. First, the baseline rate (in the pre-ACA period) was lower than the other screenings. Second, despite the USPSTF recommendation for the screening of all pregnant women for HIV as part of prenatal care, many providers may be unaware of that recommendation and still practice HIV screening based on a risk-based approach, which is supported in the literature. 42 In addition, providers may ask women whether they want to be screened for HIV, and women who believe they are at low risk may elect not to be screened. Related to this, the content of the standard obstetrical panel before 2016 did not include HIV testing, but rather HIV testing had to be ordered separately; some providers may not have been aware of the need to order the HIV testing separately from the obstetrical panel. Although it is difficult to understand why timely HIV screening would decline from 2014 to 2015, in mid-2013, the USPSTF did issue recommendations that everyone aged between 15 and 65 years get tested for HIV at least once as part of routine healthcare. 43 Thus, it is possible that from 2014 to 2015 more women may have been tested before pregnancy and providers may have chosen not to retest in pregnancy.
The analysis completed here for Ohio was possible due to the state's linkage of Medicaid administrative data (claims/encounters and enrollment data) to birth/death vital records over multiple years, data often not available in other states. Mothers and infants remain a priority population regardless of their state of residence. Support for ongoing data linkage efforts and data collection is needed to understand how Medicaid policy changes across states affect mothers and their infants. Having robust data may become more of an issue if changes to the financing of Medicaid lead to cuts in eligibility, benefits, provider reimbursements, or some combination of these in Ohio and other states. There is the potential for many women to return to instability of insurance coverage preconception, during pregnancy, and postpartum.
Finally, although it is notable that the ACA Medicaid expansion appears to address some of the critical issues related to historical Medicaid policy for women ≤138% FPL, the ACA and the Medicaid program still leave pregnant women in the next income strata, from 139% to <200% FPL, at risk of “churning” pre- and postpregnancy. Although states may be working with their exchanges to encourage women in this income range to take up private coverage through subsidies, it is unclear how successful this approach will be over time due to uncertainty about the subsidies, insurance markets, and even Medicaid itself. Thus, further investigation of the impact of policies on “churn,” insurance coverage prepregnancy, and utilization of care among pregnant women is warranted.
Conclusion
Many elements of the ACA could positively affect women of reproductive age. Expansion of Medicaid to low-income women regardless of whether they were already parents or currently pregnant was a key element in that it could reduce the persistent instability in insurance coverage before and after pregnancy experienced by many low-income women in the United States. Using Medicaid enrollment and claims data for years before and after the implementation of the Medicaid expansion in Ohio, we found that many more first-time mothers had enrolled in Medicaid before their conception and, in turn, were far more likely to receive guideline-concordant prenatal care in their first 16 weeks of pregnancy and to receive prenatal vitamins. These results cannot be generalized beyond our study state. Future study should consider the effects of Medicaid expansion on women of reproductive age and, in particular, those experiencing pregnancy in other states that expanded. In Ohio, as well as across the nation, future work should assess whether the positive findings here can be associated with improved maternal and infant outcomes among low-income women who deliver on Medicaid.
Footnotes
Acknowledgments
The Examining the Impact of Ohio's Medicaid Expansion – Health Improvement for Ohio's Women and Children project is funded by the Ohio Department of Medicaid (ODM) and administered by the Ohio Colleges of Medicine Government Resource Center (GRC). The views expressed in this manuscript are solely those of the authors and do not represent the views of the state of Ohio or federal Medicaid programs. This study includes data provided by ODM and the Ohio Department of Health, which should not be considered an endorsement of this study or its conclusions.
Author Disclosure Statement
No competing financial interests exist.