
Abstract
Background:
Professional burnout is a growing problem among physicians. Neurology has been found to be one of the specialties with the highest prevalence for burnout. However, little is known about gender-specific risk factors. The objectives of this study were (1) to determine the prevalence of burnout among a sample of women neurologists in the United States and (2) to identify predictive factors leading to burnout.
Materials and Methods:
An online survey was distributed to 798 U.S. women neurologists through the closed Facebook group Women Neurologists Group. Burnout was assessed with the Mini-Z survey. Additional questions assessed current practice settings, family and childcare responsibilities, work–life balance, gender discrimination experiences, career satisfaction, and plans for career changes.
Results:
The survey received 181 responses, yielding a 22.7% response rate. Most respondents were 1–10 years post-training and 35.4% indicated they felt neutral or dissatisfied toward their current job; 42.6% of respondents reported symptoms of burnout. Working in a high stress environment, lack of control over the work schedule, a higher number of hours at work, and self-reported gender discrimination were each independent predictive factors for burnout. Having more children was associated with decreased likelihood of becoming a physician again, and less than a third of respondents with three or more children indicated they would become a physician again. While 91.1% of respondents considered themselves effective with electronic health record use, 56.9% indicated insufficient time for documentation.
Conclusions:
Professional burnout and career dissatisfaction have high prevalence in women neurologists and threaten the future of the neurology workforce. There is an urgent need for interventions to alleviate stressors associated with burnout and measures to reduce gender discrimination.
Introduction
Physician burnout is increasingly being recognized as an alarming crisis for the health care system in the United States. A recent study found symptoms of professional burnout in over half of United States physicians, 1 which has a negative impact on physicians' personal lives as well as the quality of care provided to their patients. 1 –5 Prior studies have demonstrated increased medical errors, hospital-acquired infections, medical malpractice suits, and patient mortality associated with physician burnout. 4 Given the detriments to health care systems resulting from burnout, a better understanding of factors predictive of physician burnout is needed. Specialties with the highest risk for burnout are those at the frontline of patient care, including emergency medicine, family medicine, general internal medicine, and neurology. 4
A recent study found that 60.1% of neurologists experience at least one symptom of burnout (emotional exhaustion, depersonalization, or a sense of reduced personal accomplishment), and only one out of three neurologists indicated that their work schedule left enough time for personal and family activities. 6 Burnout and career dissatisfaction may lead physicians to reduce work hours or change careers, and is also associated with greater risk for depression and suicide. 2,3,6 –8 Burnout rates are higher among women physicians, 4,9 who face unique challenges such as harassment, gender discrimination, income inequity, increased prevalence of work–home conflicts, and difficulties advancing academically compared to their male counterparts. 10 In a study among Primary Care Physicians, women were almost twice as likely than men to report burnout. 11 Women physicians are also more likely to experience symptoms of anxiety and depression than the general population, 4,12 and more often report suffering from chronic diseases. 12
According to data from the American Medical Association in 2012, there are approximately 11,687 male and 5,123 women neurologists in the United States. 13 There is a predicted shortage of neurologists due to the projected increase in neurological diseases such as dementia and Parkinson's disease as the population ages. 14,15 The expected physician shortage will likely be worsened by physicians planning to reduce clinical work hours or leaving medicine in pursuit of another career. 16 It is therefore important for neurology to be an attractive specialty for medical trainees. There is a need for better understanding of predictive factors for burnout and an evaluation of strategies to mitigate these factors among neurologists.
The purpose of this study was to evaluate prevalence of burnout among a sample population of women neurologists in the United States and to examine career satisfaction, work–life balance, and predictive factors of burnout. We hypothesized that working a greater number of hours, having more children, experiencing greater family responsibilities, and perceiving higher stress levels would each be predictive factors for burnout in women neurologists.
Materials and Methods
We developed a survey using REDCap 17 and distributed it to 798 members of the closed Facebook group “WNG” (Women Neurologists Group). WNG is a group for women neurologists for professional networking and support. Members get only added by administrators after their status as neurologists has been verified. The study was approved by the IRB at the University of Louisville. Survey responses were collected over four consecutive weeks in June and July 2016. The survey consisted of several components, including demographics, the 11-item Mini-Z survey 18 to assess burnout (developed by Mark Linzer at Hennepin County Medical Center, Minneapolis), and questions regarding career and family life characteristics. Respondents were given the option to be entered in a gift card drawing for $100 as incentive for completing the survey.
Career characteristics
To evaluate differences in burnout among professionals with different career styles in a similar manner to previous studies, 2 we asked about medical training, fellowship involvement, subspecialty, career stage, adult versus pediatric neurology, community size, current practice setting, rank, employment status, and full-time versus part-time work. In addition, clinical time spent in inpatient versus outpatient setting, percentage of time allocated for clinical duties, hours worked per week, average nights on call per month, and method of compensation were captured in methods similar to other studies. 9,19
Family life and work–life balance
We drew from methods of prior studies to assess family life and work–life balance. 1,20 To determine effects of family time on burnout, we asked about the number of children and the age of the youngest child. Respondents were asked to rate their average daily stress level at home on a scale from 0 to 100 and were asked, “how satisfied are you with your current work–life balance?” (very satisfied, mostly satisfied, neither satisfied nor unsatisfied, mostly unsatisfied, or very unsatisfied). We inquired about maternity leave options and childcare arrangements and satisfaction with these arrangements. Because women may be affected by disruptions from work due to childcare emergencies, 21 we asked, “When your children are ill, or when other disruptions in your childcare arrangements occur, who usually stays with the children?” Similar to prior studies, 22 respondents were asked whether they followed a regular exercise routine and how many minutes of exercise they got in an average week.
Discrimination
To assess the effects of perceived gender discrimination and/or harassment on women neurologist burnout, participants were asked, “Are you experiencing gender-based discrimination at your current workplace?” (very frequently, frequently, occasionally, rarely, and never). This self-reported index of gender-based discrimination is similar to methods used in prior studies. 23 Similar to other studies, 24 we also asked who the sources of the discrimination were (administrative staff, physician at higher rank, physician at same or lower rank, other health care providers, patients, other, or not applicable). There was an additional free-response question prompting respondents to write about their experiences with discrimination at their current workplace.
Career satisfaction, stress, and burnout
Similar to other studies, 18,25 the Mini Z survey was used to evaluate burnout and job satisfaction, control over workload, time for documentation, work atmosphere, alignment of professional values with leadership, teamwork, and electronic health record (EHR) use. 18 Within this instrument, burnout is self-rated on a five-point Likert Scale ranging from “I enjoy my work. I have no symptoms of burnout” to “I feel completely burned out. I am at the point where I may need to seek help.” The Mini Z survey has been annually validated for reliability and validity. 26 Abbreviated burnout assessment through self-reported burnout experience has been shown to effectively correlate with burnout results from a full Maslach Burnout Inventory assessment among multiple large samples of medical professionals. 9,27 The Mini Z survey not only includes these single-item self-reported burnout measures but also explores work characteristics that likely contribute to burnout. In the same manner as previous studies, 2,9 the likelihood and reasoning for reducing clinical work hours in the next 12 months and likelihood for leaving the current position were assessed as measures of job satisfaction. To assess career satisfaction, participants were asked to rate their likelihood of becoming a physician again and likelihood of changing specialty similar to prior studies. 10,28,29 A free-response question was included, prompting respondents to elaborate on their stresses and provide ideas for minimizing them (“Please tell us more about your stress factors at work and what can be done to minimize them”).
An optional question asked participants to rank the relative importance of work-place policies that employers should institute to improve work–life balance for women in neurology. Choices included flexible work schedules, option to work part time, option to not take night calls, option to not take weekend calls, paid maternity leave, emergency childcare on site available, and support for breastfeeding.
Data analysis
SPSS version 22.0 was used to analyze the quantitative data. Descriptive statistics such as frequency and percentages, along with means and standard deviations were used to summarize much of the survey instrument. Kendall's tau-b was used to assess if an association existed between the two Likert response format items of burnout and discrimination.
Standard multiple logistic regression was used to assess the association of several predictive variables on burnout. First, frequencies and percentages were calculated, along with the chi-square tests, to assess independent associations. For the multiple logistic regression model, we present adjusted odds ratios (ORs) with 95% confidence intervals, along with the Nagelkerke R2. The outcome variable consisted of whether the respondent was burnt out or not as recommended by the authors of the Mini Z questionnaire. One predictor variable included stress level at home, which was a score ranging from 0 to 100. Quartiles from the stress scores were used as follows: (i) ≤33, (ii) 34–52, (iii) 53–67, and (iv) 68+. Other predictor variables included the neurologists' stage in their careers (residents/fellows, 1–10 years post-training, or 11+ years post-training), practice setting (nonacademic hospital/medical center, private practice, Veterans Affairs Medical Center/Other, or academic), number of hours worked per week (≤40 hours, 41–60 hours, or ≥61 hours), number of children, control over the workload (poor/marginal or satisfactory/good, or optimal), and the time spent on EHR at home (excessive/moderately high or satisfactory/modest/minimal). For the inferential statistics, statistical significance was set by convention at p < 0.05.
A qualitative analysis of free text comments was performed by two raters (K.L. and one independent rater not associated with the study design) according to methods described by Creswell. 30 Inductive analysis was used to develop a codebook for themes identified in free-text comments, and coding was performed after the codebook was validated for interrater agreement of K > 0.85.
Results
We received 181 responses from 798 U.S. members of the group for a response rate of 22.7%. The average age of respondents was 38.9 (standard deviation [SD] = 6.3) years and 80.5% were located in a metropolitan area (Table 1).
Demographics
SD, standard deviation.
Career characteristics
Survey respondents were in-training and practicing adult (79.4%) and pediatric (20.6%) neurologists (Table 2). The majority of respondents were working 41–60 hours per week (61.1%) and were 1–10 years post-training (77.4%) in their career stage; 49.7% of respondents were employed in an academic work environment. The average percentage of time allocated for clinical duties was 77.4%. The majority of respondents spent most of their clinical time in an outpatient setting (75.9%) and had an average of 4.6 call nights per month.
Career Characteristics
Family life
The majority of respondents (94.9%) were married or in a committed relationship; 88.4% of the respondents had children: 27.5% had one child, 45.0% had two children, and 15.9% had three or more children; and 72.5% of respondents had at least one child younger than five years. Only 20.2% had paid maternity leave available to them. The majority of respondents were either very satisfied (34.4%) or mostly satisfied (55.0%) with their current childcare arrangements and daycare was the more frequently utilized childcare arrangement in 40.0% (Table 3). Spouses/partners were most likely to provide emergency childcare backup. On a scale from 1 to 100, the average self-rated daily stress level at home was 51.1. The majority of respondents (59.3%) did not follow a regular exercise routine. Those exercising on a regular basis did so for an average of 124.9 (SD 76.2) minutes per week. In terms of satisfaction with work–life balance, 8.5% of respondents indicated being “very satisfied,” 38.3% were “mostly satisfied,” 18.1% were “neither satisfied nor unsatisfied,” 29.3% were “mostly unsatisfied,” and 5.9% were “very unsatisfied.”
Family Life
FMLA, Family and Medical Leave Act.
Discrimination
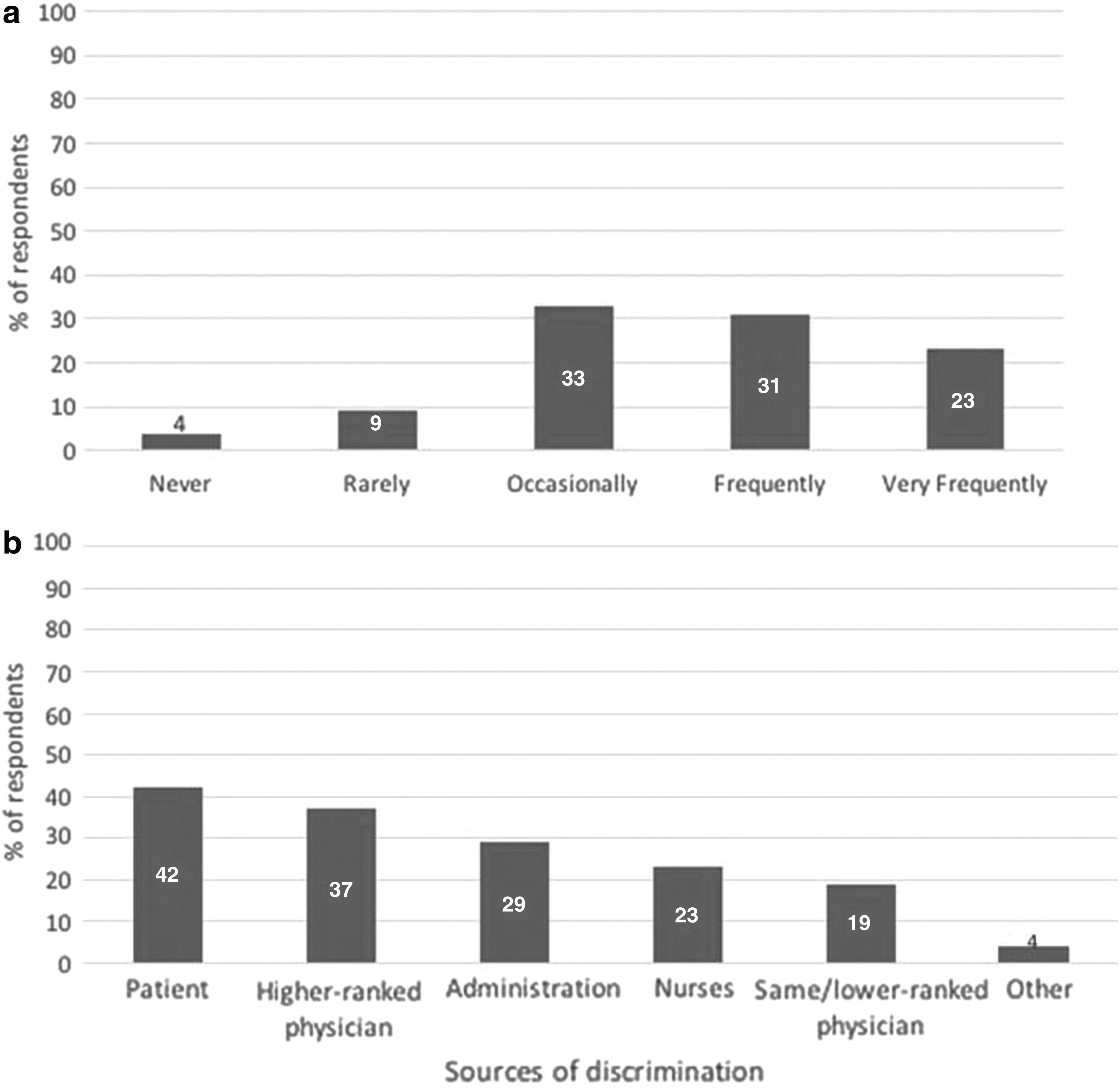
Perceived gender-based discrimination at their current workplace was reported by 76.6% of respondents (Fig. 1a), and the most common sources of perceived discrimination were patients, followed by physicians at a higher rank (Fig. 1b). In free-text responses, most frequent themes mentioned by survey respondents were discrimination related to medical expertise/professionalism (n = 19), differences in work expectations and administrative support (n = 18), and pay inequality (n = 17). Furthermore, a lack of support for advancement to leadership positions (n = 8) and discrimination in relationship to pregnancy and maternity leave (n = 9) were reported. Please refer to Supplementary Table S1 for representative quotes.
Burnout and career satisfaction
Around 35.4% of respondents felt neutral or dissatisfied toward their current job and 42.6% considered themselves to be experiencing burnout; and 43.1% of respondents had poor or marginal control over their workload (Table 4). Responses to career satisfaction questions (Table 5) indicated that most women neurologists were not considering reducing their clinical work hours in the near future, but those who were planning to do so were motivated by wanting to spend more time with their families. Respondents indicating a moderate to high likelihood of leaving their current job within the next 2 years (32.0%) were most likely looking to pursue a different practice opportunity. In terms of career choice, 59.6% would “definitely” or “probably” elect to become a physician again, and a similar percentage (61.9%) was satisfied with their specialty choice, answering “definitely not” or “probably not” to the question, “if you were to do it over again, would you change your specialty?” (Table 6) This varied by the number of children, with intent to become a physician again decreasing as the number of children increased (Fig. 2). Sixty-eight percent of respondents without children indicated they would become a physician compared to 42% with one child, 36% with two children, and only 32% with three or more children.
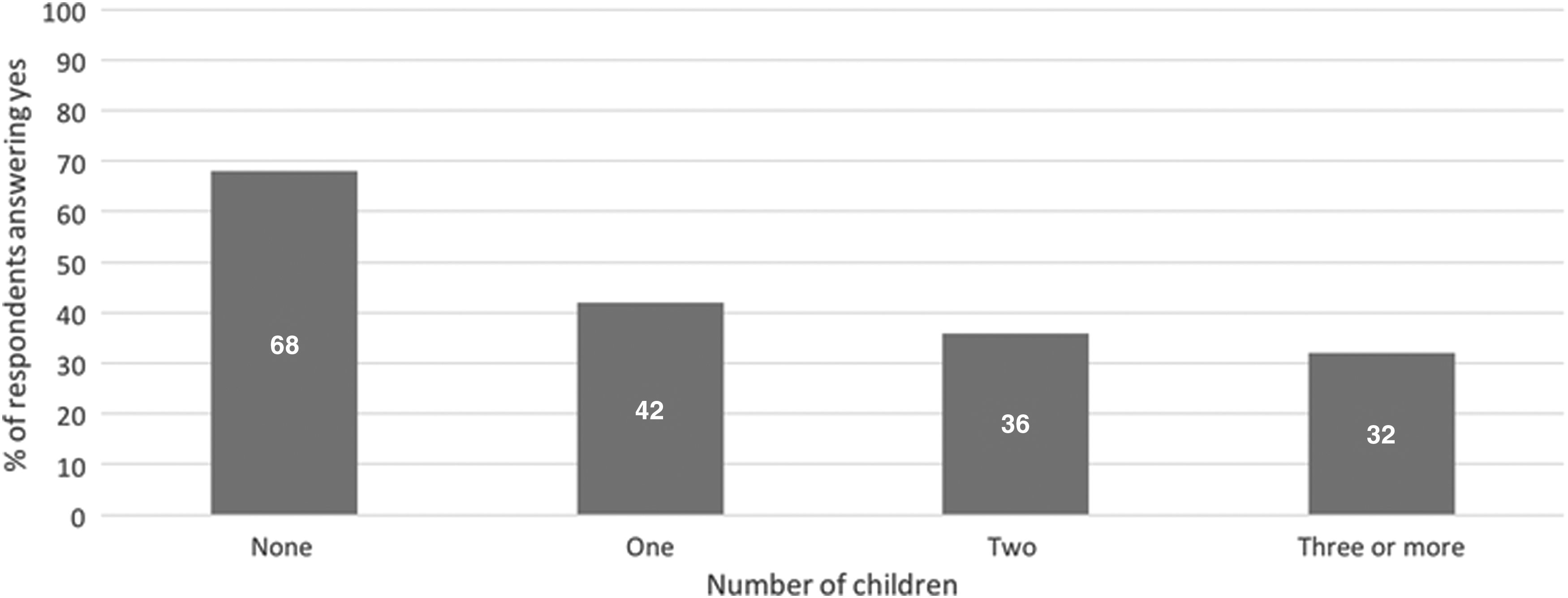
Relationship between number of children and response to the question, “If you were to do it over again, would you become a physician?”
Burnout (Mini Z Survey)
Burnout answer options were as follows: 1. I enjoy my work. I have no symptoms of burnout. 2. I am under stress and I do not always have as much energy as I did, but I do not feel burned out. 3. I am definitely burning out and I have one or more symptoms of burnout, for example, emotional exhaustion. 4. The symptoms of burnout I'm experiencing will not go away. I think about work frustrations a lot. 5. I feel completely burned out. I am at the point where I may need to seek help. Answers 1–2 were rated as “no burnout symptoms,” and answers 3–5 were rated as “burnout symptoms present.”
Self-Reported Gender Discrimination
Career Satisfaction
In response to the free-text question, “Please tell us more about your stress factors at work and what can be done to minimize them,” a total of 81 comments were analyzed and grouped into four themes. The majority of responses (n = 45) were related to workload. This category included demands for adequate support by administrative and clinic staff, protected administrative time, and appropriate patient volumes. The second theme (n = 22) was related to professionalism. In this category, respondents commented on the need for more gender equality in the workplace, increased compensation, as well as greater physician appreciation and autonomy. A need for flexible workplace policies was mentioned by 13 respondents, including flexible work schedules, options to not take call, backup childcare, and paid leave. Only one survey respondent commented on issues related to healthy living and support with home duties. Please refer to Supplementary Table S2 for representative quotes.
Documentation and EHRs
Around 91.1% of respondents considered themselves proficient with EHR use, but only 43.1% agreed that time for EHR documentation was sufficient. In terms of spending time with EHR after office hours, 16.0% reported excessive at-home use, 27.1% reported moderately high use, 13.8% reported satisfactory use, 21.0% reported modest use, and 22.1% reported minimal to no use.
Teamwork
Around 50.9% of respondents considered their professional values poorly aligned with those of their department leaders. The majority of respondents (85.7%) reported that their care team worked efficiently together.
Predictive factors for burnout
Based on a multiple logistic regression model (Table 7), higher levels of perceived stress were highly associated with burnout (OR = 3.29 for physicians in the highest quartile of stress). Burnout was significantly higher for physicians who worked greater than 61 hours per week (OR = 4.7) compared with physicians who worked less than 40 hours per week. Burnout was also significantly higher with physicians who reported poor or marginal control over their workload (OR = 3.5) compared with those who reported satisfactory, good, or optimal control. There was a statistically significant association between burnout and experiencing discrimination, Kendall's tau-b = 0.21, p = 0.002. Other variables that did not achieve significance were training stage, practice setting, and number of children (Nagelkerke R2 = 0.32).
Association with Burnout in Univariate Analysis and Multiple Logistic Regression Analysis
Reflects referent categories versus nonreferent categories.
Reflects nonreferent categories versus referent categories.
p Value <0.05.
p Value <0.01.
p Value <0.001.
OR, odds ratio; CI, confidence interval.
Preventative measures to improve career satisfaction and prevent burnout
When asked to rank the importance of workplace policies that would improve work–life balance for women neurologists, most respondents (97.7%) ranked a flexible work schedule as the most important measure, followed by paid maternity leave (83.7%) and the option to work part time (83.2%). Common themes in qualitative survey comments on other measures to reduce burnout and enhance job satisfaction were demands for greater administrative support, more time during work to take care of nonbillable clerical burdens, and more time to see patients.
Discussion
Our results indicate that a high percentage of women neurologists are experiencing symptoms of burnout. The majority of survey respondents were either in training (10.8%) or early career stages (77.4%; 1–10 years post-training). Other studies have found that early-career physicians experience the lowest career satisfaction, and highest incidence of work–home conflicts. Mid-career physicians were found to be less satisfied with their specialty choice and experiencing highest rates of burnout. 2 Our findings are in keeping with prior studies and indicate that burnout and career dissatisfaction are significant threats to the future neurology workforce. Previous studies have found that lack of schedule control, younger age, high work stress, and history of harassment are predictive factors for career dissatisfaction. 10 Among neurologists in a recent U.S. survey, hours worked per week, nights on call per week, number of outpatients seen, and amount of clerical work were associated with higher rates of burnout. 6 Our study found associations between high self-rated stress, perceived discrimination, greater number of weekly hours at work, and lack of schedule control and burnout.
The pressures to have high patient turnover and limited time for patient visits are particularly burdensome to neurologists, since a detailed clinical history and a physical examination are of high importance in this specialty. 31 Previous studies have shown that women physicians tend to display more empathy and report especially high empathic concern for patients. 32 Moreover, women are more likely than male physicians to counsel their patients 29 and spend more time with each patient, 10 which could make time pressures during patient visits even more troubling to women neurologists as they commonly report a lack of schedule control. Previous studies have identified counseling, elimination of EHR hassles, removal of pressure to have quick patient turnover, and improvement in the culture of medicine as important strategies for reducing burnout. 7 Physicians in our study indicated that greater administrative support, more time during work to take care of nonbillable clerical burdens, and more time to see patients would help reduce their job stress and improve career satisfaction. Greater physician autonomy and control over work schedules are needed to mitigate career dissatisfaction and burnout.
Poor functioning of EHRs is one of the major sources of frustration for many physicians. 8 Studies have demonstrated higher rates of burnout among physicians who use EHRs and Computerized Physician Order Entry. 19 While the majority of our respondents indicated high proficiency with EHR use, sufficient time available for documentation was deemed to be lacking. EHR use and increasing clerical burdens may be main contributors to burnout in women neurologists and administrative help was ranked highly among suggested measures for burnout mitigation. In the future, assessment of burnout among women neurologists with scribes compared to those without scribes may be of interest.
In addition to increasing demands at work, family responsibilities and dissatisfaction with work–life balance play an important role in burnout and career satisfaction. 33 Family care pressures are often greater for women, 12 who spend 8.5 hours more per week on domestic duties than men and are more likely to experience work–home conflicts. 2,21 Moreover, in an academic setting, women who are on a tenure-track and have a child within the first 5 years of that track are less likely to receive tenure than a male counterpart, 33 indicating that child-rearing responsibilities can have a greater impact on women's careers. Previous studies have reported that having more children correlates with higher career satisfaction and less burnout among women physicians. 10 Our study showed lower career satisfaction in women neurologists with a higher number of children. Notably, over two-thirds of women neurologists with three or more children would not become a neurologist again if given the chance. Our finding that doubts about the choice to become a physician increased with the number of children suggests that the pressures of juggling multiple roles can be of particular burden to women neurologists with multiple children, although the majority of respondents indicated that they were satisfied with current childcare arrangements.
Our study also showed an association between perceived gender-based discrimination and burnout. There is a significant pay gap between men and women physicians, with neurology among the most significantly affected specialties. 34 In a recent study of physician mothers, 77.9% had experienced either gender-based or maternal discrimination, and this positively correlated with burnout. 25 Experiencing disrespect from nursing or other support staff was one of the most frequently cited sources of discrimination. Women neurologists in our study conveyed frustration at receiving lower pay and fewer opportunities for promotion than their male counterparts. Respondents reported receiving little support from administration and being criticized for taking maternity leave. Of note, survey respondents expressed that discrimination by patients, for example, by questioning their competence and credentials, was even more prevalent than discrimination by other health care providers and superiors. Respondents frequently experienced less support and respect by administrative and nursing staff compared to male physicians. An ongoing demographic shift is expected to lead to a narrower gap in the experience of men and women physicians, with 47.6% of women medical school graduates in the United States in 2015. 35 Implicit bias training for health care professionals may be helpful in starting to address gender-based discrimination. 36 Suggested measures to address pay inequity include bringing greater awareness to this issue, better mentoring and coaching of women physicians in salary negotiations, greater salary transparency, and nondepartmental oversight of compensation models for employed physicians. 37 Facilitated peer-connection groups have been shown to increase self-compassion and reduce rates of stress and depression in physician mothers, 38 and should be further explored as a way to foster resilience and reduce burnout. Regular exercise is often suggested as a way to prevent burnout 39 and was recently found to be associated with a lower risk for burnout and higher quality of life in U.S. medical students. 22 The majority of survey respondents (59.3%) were not following a regular exercise regimen, and emphasizing the benefits of exercise on mental health and wellness could be an opportunity for burnout prevention.
Physicians are increasingly engaged in social media platforms such as Facebook (Facebook, Inc., Menlo Park, CA) and Twitter (Twitter, Inc, San Francisco, CA),
40
and groups such as “PMG” (Physician Moms Group;
While previous studies have found that team-based, patient-centered medical care resulted in lower rates of burnout, 7 we found high degree of satisfaction with the efficiency of care teams and no correlation between dissatisfaction with care teams and burnout. However, 50.9% indicated that their professional values were not well aligned with their department's leadership and this could be a source of stress and frustration that needs to be addressed.
Respondents in our study ranked flexible work schedules, paid maternity leave, and the option to work part time highest in workplace measures to mitigate burnout and improving work–life balance. Poor control over workload was correlated with burnout, similar to findings in previous studies. 6 Greater involvement of women physicians in decision making, both at the level of individual practices and departments as well as in health care institutions and professional societies, will be necessary to incorporate meaningful changes. Reducing administrative burdens and implementing workplace policies important to women are expected to have a higher impact on burnout prevention than focusing on individual's coping strategies and resilience training alone. 5,41 Our study aimed to assess factors that are important to burnout developing in women neurologists and some of our findings are more gender specific than others. Factors associated with burnout that are more likely to affect women are gender-based discrimination, issues with work–life balance, and misalignment of personal and departmental values, whereas other factors are less gender specific such as control over work activity, greater number of hours worked per week, clerical burden, and care team efficiency.
Our study had several limitations. First, our sample was nonrandomly selected since the survey was distributed through a closed Facebook group. There was a high prevalence of physicians with children in our group, making this a disproportionately represented subpopulation. The overall number of respondents was relatively small, not allowing separate analysis by subspecialty choice. However, our respondents had many similarities with demographics and career characteristics for all neurologists according to the AAN inventory, 42 and women neurologists represented a greater proportion of U.S. neurologists younger than 50 years, correlating with our average respondents' age of 38.9 years. Another possible limitation was our use of the Mini Z survey to address burnout rather than the Maslach Burnout Inventory, the gold standard. The length of the Maslach Burnout Inventory can be prohibitive given that our study asked many other questions and the abbreviated Mini Z survey was used in effort to increase response rate; in addition, the Mini Z survey was developed for physicians and aims to investigate causes of burnout, making it a useful tool for our study. Important strengths of the study are representation of women neurologists in a variety of practice settings and the focus on gender-specific issues related to burnout. Future research should address the effect of burnout mitigation strategies, taking gender-specific factors such as pay inequity and discrimination into account. Finally, instituting policies to reduce gender inequality and promote work–life balance is expected to benefit neurologists of both genders and make neurology a specialty attractive to medical students.
Conclusions
Burnout among women neurologists is an important issue leading to personal dissatisfaction, suboptimal patient care, and threats to the future neurology workforce. There is an unmet need to address gender-specific factors leading to burnout, particularly in early career stages, when low control over work schedules, difficulties in meeting family responsibilities, and perceived gender-based discrimination are culminating. Our study confirmed our hypothesis that working greater hours per week, reporting higher stress levels, experiencing more gender-based discrimination, and having less control over scheduling were each factors that were associated with higher rates of burnout in women neurologists. We also found lower career satisfaction and greater career doubts in women neurologists with more children. In addition to interventions previously investigated, there is likely particular benefit for women neurologists in reducing gender-based discrimination, instituting flexible work hours and night call, and providing maternity leave benefits. Addressing these challenges will be paramount in reducing burnout, improving quality of life and career satisfaction in women neurologists.
Footnotes
Acknowledgment
The authors are grateful to all WNG members participating in the survey.
Author Disclosure Statement
L.R.M., C.Z., A.H., and D.S. have nothing to disclose. K.L. has received speaker's honoraria from TEVA.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.