
Abstract
Background:
Research shows that individuals can improve mental health by increasing experiences of positive emotions. However, the role of positive emotions in perinatal mental health has not been investigated. This study explored the extent to which positive emotions during infant feeding are associated with maternal depression and anxiety during the first year postpartum.
Materials and Methods:
One hundred and sixty-four women drawn from a longitudinal cohort of mother–infant dyads were followed from the third trimester through 12 months postpartum. We measured positive emotions during infant feeding at 2 months using the mean subscale score of the modified Differential Emotions Scale. Depression and anxiety symptoms were assessed with the Beck Depression Inventory-II and State Trait Anxiety Inventory-State subscale at months 2, 6, and 12. Generalized linear mixed models were used to estimate crude and multivariable associations.
Results:
Among women with no clinical depression during pregnancy, higher positive emotions during infant feeding at 2 months were associated with significantly fewer depression symptoms at 2, 6, and 12 months and with lower odds of clinically significant depression symptoms at 2 and 6 months. In contrast to depression outcomes, women with clinical anxiety during pregnancy who experienced higher positive emotions had significantly fewer anxiety symptoms at 2, 6, and 12 months and lower odds of clinically significant anxiety at 2 and 6 months.
Conclusions:
Positive emotions during infant feeding are associated with depression and anxiety outcomes during the first year postpartum and may be a modifiable protective factor for maternal mental health.
Introduction
P
One promising target for intervention is positive emotionality. Positive emotions are pleasantly-valenced discrete responses to one's appraisal of circumstances as favorable, 10 with biobehavioral features that are empirically distinguishable from negative emotions. 11 Positive psychology interventions that increase experiences of positive emotions have been shown to experimentally reduce depression and anxiety symptoms 12 –14 and to improve resilience to future stressors through resources such as social support 15 and coping skills. 16,17 The broaden-and-build theory of positive emotions 18 posits that these durable psychological and social resources result from the broadened cognitive and creative context associated with experiences of positive emotions. 19,20
Preliminary evidence suggests an association between positive emotions and postpartum mental health. Among 344 Norwegian mothers followed up for 6 months postpartum, those using positive reappraisal as a coping strategy reported fewer depression symptoms. 21 An observational study of 195 Greek women found an inverse association between positive emotions in the third trimester and depression symptoms at 1 week postpartum. 22 However, neither of the above studies controlled for women's baseline mental health status, calling the causal direction of this association into question. In a sample of breastfeeding mothers, those with fewer postpartum depression and anxiety symptoms reported higher positive affect during observed feeding sessions at 2 and 8 weeks. 23 Positive emotions experienced during regular mother–infant interactions such as infant feeding may broaden their associated benefits by increasing maternal sensitivity and attachment. 24,25 Mothers who describe breastfeeding as a positive activity express feeling connected to their infant, self-confident as a parent, and supported to face new challenges. 25 To our knowledge, no study has explored the association between positive emotions experienced during infant feeding and prospective maternal mental health outcomes.
To better understand the role of positive emotions in perinatal mental health, we estimated the association between positive emotions during infant feeding and maternal depression and anxiety symptoms across the first year postpartum. Grounded in the broaden-and-build theory, we hypothesized that women reporting more positive emotions during infant feeding at 2 months would have fewer postpartum depression and anxiety symptoms at 2, 6, and 12 months. We also explored the extent to which associations between positive emotions and depression and anxiety symptoms differed by women's baseline psychopathology.
Materials and Methods
Sample
Our sample was drawn from 220 pregnant women who were enrolled to the longitudinal cohort study Mood, Mother and Infant: The Psychobiology of Impaired Dyadic Development (MMI) and followed up from the third trimester until 12 months postpartum. The MMI cohort comprised women living near Chapel Hill, North Carolina, recruited through study fliers and obstetric or psychiatric visits. We oversampled women at elevated risk for postpartum depression and anxiety based on a history of depression/anxiety or an active depressive/anxiety disorder in the third trimester of pregnancy using a Structured Clinical Interview for DSM-IV (SCID). Eligible participants were 18–45 years old; 34–37 weeks' gestation of a singleton pregnancy; able to communicate in English; and intending to breastfeed for more than 2 months. Women were excluded from the study if they met any of the following criteria: history or current diagnosis of psychiatric disorders other than depression/anxiety; substance use disorder; neonatal intensive care unit admission >48 hours; major congenital anomaly, or neonatal death; use of tricyclic antidepressants; or contraindication for breastfeeding. A full description of the study can be found at
For this analysis, we restricted to participants completing their 12-month visit by May 2017 (n = 177). We excluded women missing exposure data (n = 12) and one influential outlier based upon a priori criteria. The remaining 164 women comprise our analytic sample.
Measures
Baseline data were collected through questionnaires and interviews with study staff at the third-trimester laboratory visit, and follow-up contacts occurred through monthly phone interviews and laboratory visits at 2, 6, and 12 months postpartum.
Positive emotions during infant feeding
At 2 months postpartum, participants completed the modified Differential Emotions Scale (mDES), 26 rating the “greatest amount” they experienced 20 positive and negative emotions during infant feeding over the past week using a five-point Likert scale (0 = not at all; 4 = extremely). The mDES was adapted from Izard's Differential Emotions Scale 27 and has a high internal reliability ranging from 0.82 to 0.94. 15,28 Our exposure uses the positive emotions subscale of the mDES, which provides a mean score across 10 discrete emotions: amusement, awe, contentment, gratitude, hope, joy, interest, love, pride, and inspiration. The experience of positive emotions during infant feeding at 2 months was analyzed as a continuous exposure and compared for consistency with alternate categorizations, such as binary (at the mean, median, and cutpoints between 2 and 3), tertiles, quartiles, and splines, based on distributions observed in the data. Using the criteria of model fit and interpretability, we chose a dichotomous exposure to compare high (≥2.5) versus low (≤2.5) positive emotions during infant feeding.
Postpartum depression and anxiety symptoms
At 2, 6, and 12 months, depression symptoms were measured using the Beck Depression Inventory-II (BDI-II), 29 and anxiety symptoms were measured using the State Trait Anxiety Inventory-State (STAI-S) subscale. 30 Both instruments have been validated in perinatal populations. 31,32 Outcomes were assessed as both continuous symptoms and binary thresholds for meeting clinically significant cutoffs for depression or anxiety. A BDI-II cutoff of ≥14 has been shown to have a 92% sensitivity and 83% specificity for major depression based on a Mini International Neuropsychiatric Interview in a postpartum outpatient sample, 33 and a STAI-S >40 administered at 1 week postpartum had a 67.5% sensitivity and 87.1% specificity in identifying anxious mothers at 8 weeks. 34
Potential covariates
We used a directed acyclic graph
35
to identify potential confounding and effect measure modification (Supplementary Fig. S1; Supplementary Data are available online at
Statistical analyses
Generalized linear mixed models were used to estimate the crude and multivariable associations between experiences of positive emotions during infant feeding at 2 months and depression and anxiety scores at 2, 6, and 12 months. Mixed models are appropriate for longitudinal data with correlated error terms and both population-specific parameters (fixed effects) and subject-specific parameters (random effects). Based on Akaike Information Criteria (AIC) and Bayesian Information Criteria (BIC), the best fitting model for continuous outcomes included a random intercept to allow 2-month depression/anxiety scores to differ among participants, a random effect for time to account for interpersonal differences in linear change in scores over time, and a variance components covariance structure. For binary outcomes, the best fitting models included a random intercept only.
Confounders were included where they (1) were identified as important to adjust for based on subject matter knowledge as represented in the directed acyclic graph and (2) resulted in a change in the exposure–outcome effect estimate by >10% using backward elimination from the full model. Crude and adjusted estimates and their associated 95% confidence intervals (CIs) are presented for overall models. Effect measure modification was considered to be present where Likelihood Ratio Test (LRT) p values were <0.05 comparing models with and without an interaction term. Analyses were performed using SAS 9.4 (SAS Institute, Cary, NC).
Sensitivity analyses repeated the above analyses removing (1) exclusive formula feeders at 2 months, as these women may have a different emotional experience of infant feeding, and (2) women taking psychotropic medications, as their depression/anxiety symptoms may be low due to treatment despite their elevated baseline risk.
Results
Study sample characteristics
Descriptive characteristics are presented for the 164 women in the study sample by high (≥2.5 to 4) versus low (0–2.5) positive emotions scores (Table 1). The mean positive emotions score was 2.8 (standard deviation [SD], 0.8), with 64.6% of the sample classified as experiencing high positive emotions. Based on the third-trimester SCID, 23.8% of the sample had a depressive disorder during pregnancy (Major Depressive Disorder, Dysthymic Disorder, Depressive Disorder Not Otherwise Specified, or Postpartum Depression) and 26.2% had an anxiety disorder (Panic Disorder, Agoraphobia without History of Panic, Social Phobia, Obsessive Compulsive Disorder, Posttraumatic Stress Disorder, or Generalized Anxiety Disorder), with no significant differences by high versus low positive emotions. Approximately 76% of the sample was non-Hispanic White, almost half reported a postgraduate level of education, and about 90% were married/partnered, with no significant differences in positive emotions by sociodemographic characteristics. Approximately 27% of the sample was taking a psychotropic medication or participating in psychotherapy between baseline and exposure. Nearly one-third of the sample had not met their prenatal breastfeeding intention for any or exclusive breastfeeding by 2 months, with a higher percentage of these women reporting low positive emotions. Almost 30% had returned to work by 2 months postpartum, and 25% reported moderate/severe childhood trauma. Women who reported high positive emotions during infant feeding at 2 months had fewer concurrent negative emotions or early breastfeeding problems and were more likely to have liked breastfeeding in the first week postpartum (Table 1).
Modified Differential Emotions Scale scores range from 0 to 4, with higher scores indicating more emotions; descriptive statistics are presented by high positive emotions (score >2.5 to 4) and low positive emotions (0–2.5).
Independent samples t-test for continuous variables; chi-square test and Fisher's exact test for categorical variables.
Based on Structured Clinical Interview for DSM-IV criteria for active depression (including Major Depressive Disorder, Dysthymic Disorder, Depressive Disorder Not Otherwise Specified, or Postpartum Depression); a history of depressive disorder and current treatment with antidepressants or psychotherapy for more than once per month; active anxiety (including Panic Disorder, Agoraphobia, Social Phobia, Obsessive Compulsive Disorder, Generalized Anxiety Disorder, or Posttraumatic Stress Disorder); or a history of anxiety disorder and current treatment with antidepressants, benzodiazepines, or psychotherapy for more than once per month.
Includes self-reported psychotherapy or any of the following medications: antidepressants, benzodiazepines, antipsychotics, and hypnotics.
Defined as meeting prenatal intention for any and exclusive breastfeeding.
Defined as meeting the threshold for moderate/severe emotional abuse, physical abuse, sexual abuse, emotional neglect, or physical neglect on the 28-item Childhood Trauma Questionnaire.
Carey Early Infancy Temperament Questionnaire comprises nine categories of temperament, with higher scores indicating more difficult/negative qualities.
Medical Outcomes Study Social Support Survey scores range from 0 to 4, with higher scores indicating more support.
Early breastfeeding problem scores range from 0 to 18, with higher scores indicating more problems.
Likert scale from “1: Disliked very much” to “5: Liked very much.”
Bolded results are significant at p < 0.05.
Positive emotions during feeding and depression outcomes
In the overall sample, the mean BDI-II score was 8.0 (SD, 5.4) at 2 months, 7.2 (SD, 5.5) at 6 months, and 7.5 (SD, 7.0) at 12 months, with significant between-person trajectories of change over time. Approximately 16.5% of the sample met the criteria for clinically significant depression (BDI-II ≥14) at 2 months, 15.2% at 6 months, and 16.5% at 12 months. In crude models, high positive emotions during feeding were associated with a 2.85 (95% CI, 1.28–4.41) point decrease in BDI-II score at 2 months, a 2.90 (95% CI, 1.35–4.44) point decrease at 6 months, and a 2.98 (95% CI, 0.29–4.72) point decrease at 12 months (Table 2). These results remained significant but attenuated by month 12 after adjustment for prenatal depression scores, social support, and concurrent negative emotions during feeding: high positive emotions were associated with an adjusted 1.53 (95% CI, 0.20–2.87) point decrease in BDI-II score at 2 months, a 1.59 (95% CI, 0.32–2.86) point decrease at 6 months, and a 1.67 (95% CI, −0.26 to 3.60) point decrease at 12 months (Table 2). Our results remained robust to sensitivity analyses testing both the exclusion of exclusive formula feeders and women taking psychotropic medications (Supplementary Table S1).
Mixed models were used to estimate the crude and multivariable associations. Linear mixed models for continuous depression/anxiety outcomes included a random intercept to allow baseline depression/anxiety scores to differ among participants, a random effect for time to account for interpersonal differences in scores over time, and a variance components covariance structure to account for intrapersonal correlations across repeat measures. For binary outcomes, generalized linear mixed models included a random intercept and unstructured covariance structure. All adjusted models controlled for prenatal depression (BDI-II) or anxiety (STAI-S) scores, social support at 2 months, and concurrent negative emotions during infant feeding at 2 months. Bolded results are significant at p < 0.05.
BDI-II scores range from 0 to 63, with higher scores indicating more depression symptoms.
Baseline psychopathology was determined using SCID in the third trimester of pregnancy. The “no diagnosis” group includes those with no history and those with a history of depression/anxiety, whereas the “prenatal diagnosis” group met criteria for an active disorder during pregnancy.
Spielberger STAI-S scores range from 20 to 80, with higher scores indicating more anxiety symptoms.
BDI-II, Beck Depression Inventory-II; CI, confidence interval; STAI-S, State Trait Anxiety Inventory-State.
Baseline diagnosis of clinical depression significantly modified the association between positive emotions and depression scores (LRT, 14.6; p ≤ 0.001). Among women with no clinical depression during pregnancy, positive emotions during feeding were associated with significantly lower BDI-II scores at 2, 6, and 12 months. No significant association was observed among women with a depression diagnosis during pregnancy (Fig. 1).
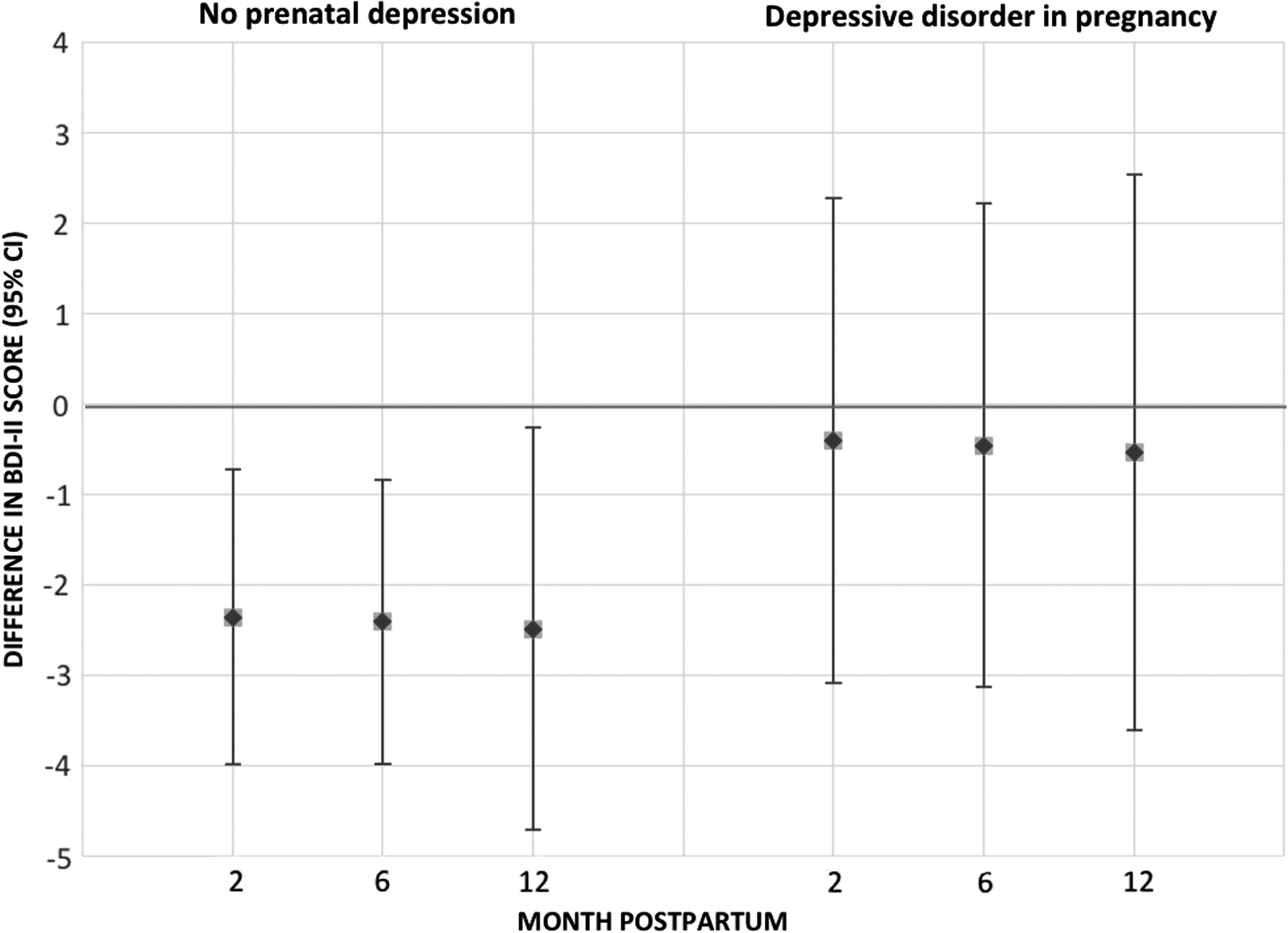
The association between high versus low positive emotions during infant feeding and depression scores (BDI-II) at 2, 6, and 12 months, by baseline depression status. Point estimates show the association between high versus low positive emotions and BDI-II scores at 2, 6, and 12 months postpartum. The error bars indicate 95% confidence intervals; error bars that include 0 are not statistically significant. BDI-II, Beck Depression Inventory-II.
Similar patterns were observed for the clinically significant depression outcome. Stronger effects of positive emotions during feeding were observed for women without a prenatal diagnosis of depression: high positive emotions were associated with significantly lower odds of clinically significant depression symptoms (BDI ≥14) at 2 and 6 months among women with no diagnosis of prenatal depression (Table 2).
Positive emotions during feeding and anxiety outcomes
The mean STAI-S anxiety score in the sample was 28.6 (SD, 7.4) at 2 months, 28.2 (SD, 6.5) at 6 months, and 29.7 (SD, 8.0) at 12 months. Approximately 7.3% of the sample met the criteria for clinically significant anxiety (STAI-S > 40) at 2 months, 4.9% at 6 months, and 9.8% at 12 months. In crude models, high positive emotions during feeding were associated with a 3.15 (95% CI, 1.08–5.23) point decrease in STAI-S score at 2 months, a 2.94 (95% CI, 1.04–4.85) point decrease at 6 months, and a 2.63 (95% CI, 0.19–5.08) point decrease at 12 months (Table 2). These associations were attenuated and became nonsignificant after adjustment for baseline anxiety scores, social support, and concurrent negative emotions (Table 2).
The association between positive emotions and anxiety scores was significantly different by baseline anxiety disorder diagnosis (LRT, 9.6; p = 0.002); however, in contrast to depression, positive emotions and anxiety scores were more strongly inversely associated among women with an anxiety diagnosis during pregnancy (Fig. 2). Among women with clinical anxiety at baseline, positive emotions were associated with significantly lower postpartum anxiety at 2 and 6 months.
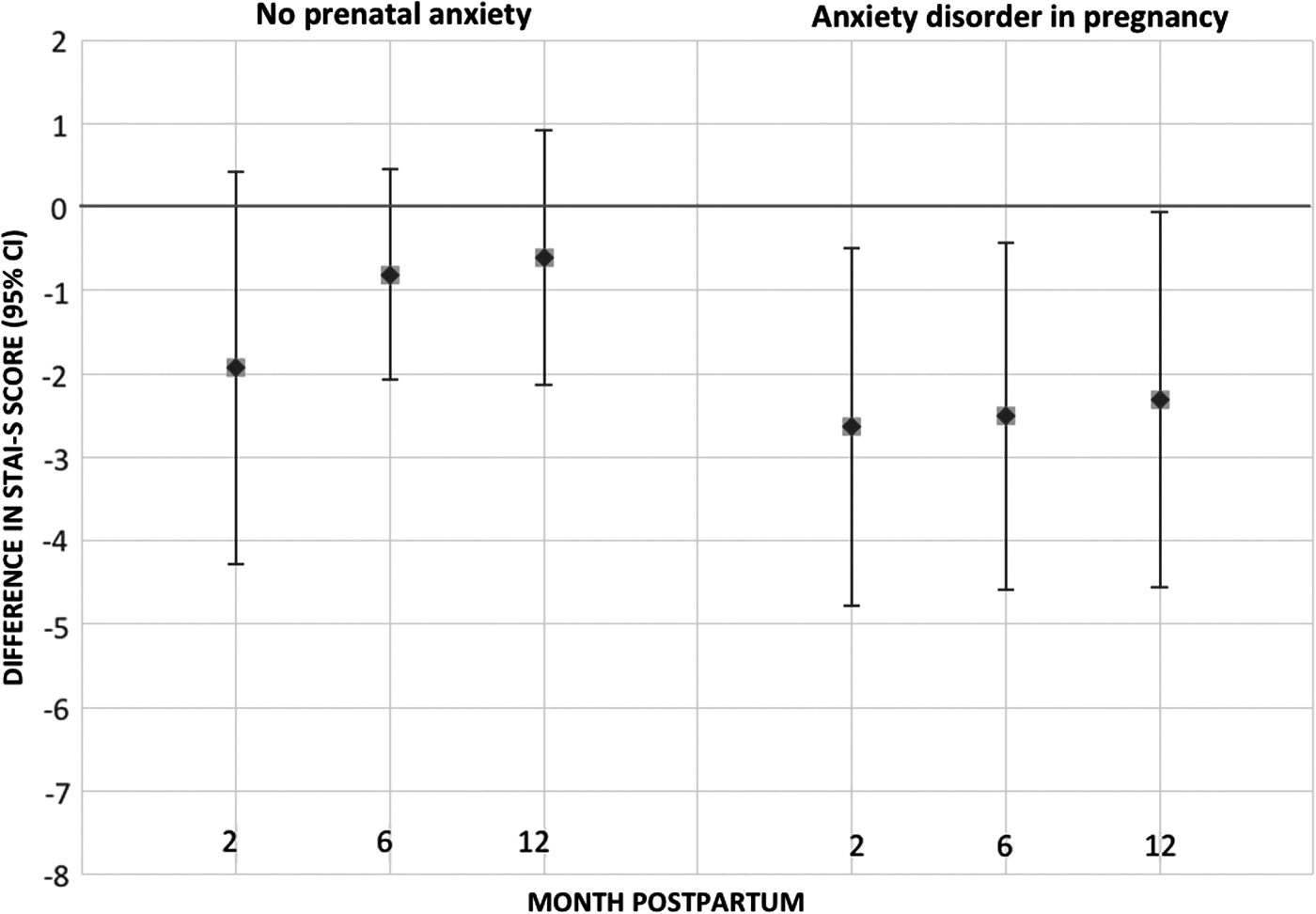
The association between high versus low positive emotions during infant feeding and anxiety scores (STAI-S) at 2, 6, and 12 months, by baseline anxiety status. Point estimates show the association between high versus low positive emotions and STAI-S scores at 2, 6, and 12 months postpartum. The error bars indicate 95% confidence intervals; error bars that include 0 are not statistically significant. STAI-S, State Trait Anxiety Inventory-State.
Positive emotions during feeding were not associated with clinically significant anxiety symptoms (STAI > 40) in the overall sample; however, as with continuous anxiety scores, stronger and significant associations were observed among women with prenatal anxiety. Among women with clinical anxiety during pregnancy, higher positive emotions were associated with 0.17 (0.01–0.56) times the odds of clinically significant anxiety at 2 months, 0.07 (0.01–0.63) times the odds at 6 months, and 0.12 (0.01–1.23) at 12 months (Table 2). Sensitivity analyses yielded similar results (Supplementary Table S1).
Discussion
Positive emotions during infant feeding at 2 months postpartum were associated with maternal mental health across the first year postpartum. Among women without a diagnosis of depression during pregnancy, high positive emotions during feeding were associated with significantly lower depression symptoms at 2, 6, and 12 months. This association strengthened over time, even after controlling for prenatal depression symptoms, concurrent negative emotions during feeding, and social support. High positive emotions were also associated with lower odds of clinically significant depression symptoms among women without depression during pregnancy. In contrast, high positive emotions were associated with lower anxiety symptoms among women with a diagnosis of anxiety disorder during pregnancy.
The association between positive emotions and depression outcomes was stronger among women who were not actively depressed during pregnancy. High negative affect has been shown to attenuate associations with positive emotions in other contexts; for example, an observational study of women with HIV has found that the association between positive emotions and viral load suppression weakened at elevated levels of negative affect. 41 Depressed individuals experienced disturbances in positive emotional functioning with attentional biases toward negative information, inability to sustain positive affect over time, and less activation of associated reward circuitry. 42,43 These cognitive distortions may reduce the potential benefits of positive emotions during infant feeding.
In contrast to depression outcomes, the protective association between positive emotions and anxiety was stronger among women with a prenatal diagnosis of anxiety disorder. We speculate that positive emotions during infant feeding may buffer against developing postpartum anxiety symptoms by improving psychological resilience to stress. 26,44 Women with prenatal anxiety who enjoy breastfeeding may benefit more from the anxiolytic effects of oxytocin during breastfeeding 45,46 compared to women with prenatal depression. 23
This is the first study to explore an association between positive emotions during infant feeding and postpartum mental health. Strengths of this investigation include the extensive longitudinal data on women's mental health, infant feeding, and descriptive characteristics, which address some limitations of previous correlational research. 47 We used a prenatal SCID to control for baseline mental health status, isolating the association between positive emotions during feeding and later mental health outcomes. Unmeasured confounding was reduced due to the breadth of data collected over time on study subjects and the minor amount of missingness. Finally, we applied Fredrickson's broaden-and-build theory to a new and understudied population, mother–infant dyads in the perinatal period. Our findings support the importance of examining mother–infant relational experience in the context of maternal mental health, given that few treatments for postpartum depression/anxiety address the mother–infant relationship. 48,49
Our findings should be interpreted in the context of study limitations. To be included in the study, subjects needed to intend to breastfeed for at least 2 months; as a result, study participants were more highly motivated to breastfeed than the general population. Moreover, it is likely that women with severe depression/anxiety were unable to participate in this intensive longitudinal study. Moreover, women with severe depression or anxiety symptoms may have been unwilling to enroll in this intensive year-old study. Our study sample was predominantly non-Hispanic White, partnered, and highly educated, limiting our ability to consider modification by race/ethnicity or socioeconomic status despite well-established associations between these social determinants of health and both infant feeding and mental health. Future research on positive emotions during infant feeding or while engaged in other bonding activities should be conducted among women of color and groups with lower breastfeeding intentions.
Self-report measures used in analyses may have led to reporting bias, especially where affective responses are influenced by concurrent depression/anxiety. While the mDES has not been previously used in the context of infant feeding, it has been validated across numerous contexts, 15,28 and we conducted a factor analysis that confirmed that the positive emotions subscale best represented one coherent construct in relation to infant feeding (Supplementary Fig. S2). Our study examined positive emotions during feeding at a single time point; future studies would benefit from exploring the emotional experience of infant feeding over time to quantify temporal dynamics of positive emotions and postpartum mental health. Finally, the relationship between positive emotions and depression/anxiety may be bidirectional. We reduced the likelihood of confounding by baseline psychopathology by using longitudinal data to support the temporality of our hypothesized associations and by controlling for prenatal depression/anxiety.
Conclusions
According to the broaden-and-build theory of positive emotions, experiences of positive emotions trigger upward spirals that improve mental health and well-being. 18 Our study provides preliminary evidence for an association between positive emotions during infant feeding and postpartum mental health. These results can inform future clinical interventions to target the positive affect system in the perinatal period, leveraging the nurturing relationship between mother and infant to improve postpartum mental health.
Footnotes
Acknowledgments
This work was supported by the National Institute of Child Health and Human Development (R01HD073220 and 4T32HD052468-09) and the National Institute on Drug Abuse (K01 DA035153). This article uses data collected by the extraordinary MMI research team, including Brenda Pearson, Pam Beiler, Mala Elam, and Hmellisa Mlo. Barbara Fredrickson, a Kenan Distinguished Professor at the University of North Carolina at Chapel Hill, provided substantive and methodological expertise for studying positive emotions in this novel context.
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.