
Abstract
The risks and benefits of menopausal hormonal therapy (HT) have been evaluated extensively over the past three decades. While the efficacy of HT for management of menopausal symptoms, including vasomotor symptoms and vaginal dryness is well established, its relationship to cardiovascular outcomes is complex. The timing hypothesis, which posits that the cardiovascular effects of HT depend on the timing of initiation of HT in relation to menopause, has helped shape our understanding of the cardiovascular outcomes related to HT. Based on results from female monkey studies, the timing hypothesis provides a framework to explain discrepancies in results between multiple observation studies and the Women's Health Initiative (WHI) hormone therapy trials. The WHI trials closed early in 2002 in part because of increased cardiovascular events seen in women on treatment. Subanalysis of the WHI results by age group, and more recent randomized control studies, including the Kronos Early Estrogen and Prevention Study (KEEPS) and Early Versus Late Intervention Trial (ELITE), demonstrate that the risk of adverse cardiovascular events for HT are low for women <60 years of age or within 10 year from menopause. Although current data does not support using HT for primary prevention of cardiovascular disease, it does suggest that HT can be safely used to treat symptoms in appropriately selected women close to menopause.
Introduction
B
Multiple society guidelines, including the North American Menopause Society (NAMS), the Endocrine Society, and the American College of Obstetricians and Gynecology (ACOG) support use of HT in symptomatic women under age 60. Despite these recommendations, women are being underevaluated and undertreated. 2,6,16,17 Decreased medical school and residency training in menopause management has left many primary care providers unequipped to treat menopausal symptoms. 6,18 Women report that their clinicians are reluctant to prescribe HT and may not recognize the significant lifestyle impact of menopausal symptoms. 19 This is important considering the improved quality-of-life benefits experienced by many women on HT, and for controlling health care spending as untreated VMS is costly with close to $400 million health care dollars being spent directly or indirectly. 1 A study in 2015 showed that only 5.9% of symptomatic women with moderate-to-severe VMS were using HT, and less than 1% was using nonhormonal treatments. 20 Without appropriate treatment and acknowledgement of symptoms by clinicians, alternate treatments untested and unregulated by the Food and Drug Administration (FDA) have become increasingly popular, such as custom-compounded hormone therapy. A survey done by the NAMS found 35% of women take custom-compounded hormone therapy, which may be harmful. 21
The following review summarizes current knowledge of the relationship between HT and CVD utilizing the timing hypothesis as a framework. This information is important in understanding the risk/benefit ratio of HT use in symptomatic menopausal women, and should help reassure clinicians about prescribing HT to appropriately selected younger women close to menopause since the benefit largely outweighs the risk for symptomatic women.
The Timing Hypothesis
The timing hypothesis was first described in the 1990s by Clarkson and colleagues based on nonhuman primate studies. 15 They showed that initiation of estrogen therapy, usually 17β-estradiol, at the time of oophorectomy reduced coronary artery atherosclerosis by 50%–70%, whereas when hormone therapy was started 2 years (equivalent to about 6 years in humans) after oophorectomy in estrogen-deprived monkeys, there was no benefit. The studies showed that overall estrogen therapy reduced progression of atherosclerosis but did not affect regression of atherosclerotic plaques once formed. Women who are older and further from menopause likely have more atherosclerotic plaque burden and thus do not see the same benefits of estrogen therapy on younger women closer to menopause. 22,23 The timing hypothesis comments on initiation of HT only.
Subsequently, results of 16 prospective cohort studies, showed favorable cardiovascular health outcomes in symptomatic menopausal women treated with HT within 2–3 years of menopause consistent with the timing hypothesis. In a cohort of 2,270 Caucasian women between the ages of 48 and 69 years followed for an average of 8.5 years, Bush et al. found that those who received estrogen therapy had a reduced risk of CVD-related deaths when compared with nonestrogen users (relative risk [RR]: 0.34, confidence interval [95% CI] 0.12–0.81). 9 Similarly, the Nurses' Health Study followed nurses ages 30–55; those on estrogen therapy had a decreased risk of fatal and nonfatal myocardial infarction (MI) even when controlling for other risk factors (RR: 0.5, 95% CI 0.3–0.8) compared with those who were not on estrogen therapy. 10 Ten-year follow-up from the study showed a continual benefit on prevention of coronary disease (RR: 0.56, 95% CI 0.4–0.8) and mortality from CVD (RR: 0.72, 95% CI 0.55–0.95) in women who were former and current users of estrogen. 24 Results from multiple large cohort studies identified that increased duration of estrogen use was associated with decreased mortality, with only one showing increased risk of CVD in menopausal women among all age cohorts from 50 to 83 years. 11,12,25,26
Women's Health Initiative
The WHI randomized hormone therapy clinical trial was the first and largest randomized control trial that evaluated the risks and benefits of HT for primary prevention of heart disease. One main aim was to evaluate the effect of HT on coronary heart disease (CHD), defined as nonfatal MI or coronary death. 27,28 In total, 10,739 women 50 to 79 years of age with a uterus were enrolled and randomized to 0.625 mg/day of conjugated equine estrogen (CEE) +2.5 mg/day of medroxyprogesterone acetate (MPA), in the CEE+MPA trial. In the CEE alone trial of women without a uterus, 8,506 were enrolled. The placebo arm was made up of 8,102 women. The intervention phase of the CEE+MPA trial was stopped early by the data and safety monitoring board for the WHI after a median of 5.6 years due to increased risks of breast cancer, stroke, and CHD. 28 In women receiving CEE+MPA, there was an increased risk of all cardiovascular event (CVE) (Hazard Ratio [HR]: 1.13, 95% CI 1.02–1.25, p = 0.02), and total MI (HR 1.24, 95% CI 0.98–1.56, p = 0.07) (Fig. 1). Women receiving CEE-only similarly experienced an increase in CHD (HR 1.11, 95% CI 1.01–1.22, p = 0.03). Findings of increased risk for CHD and total MI from the intervention phase persisted into the extended follow-up phase (Fig. 2).
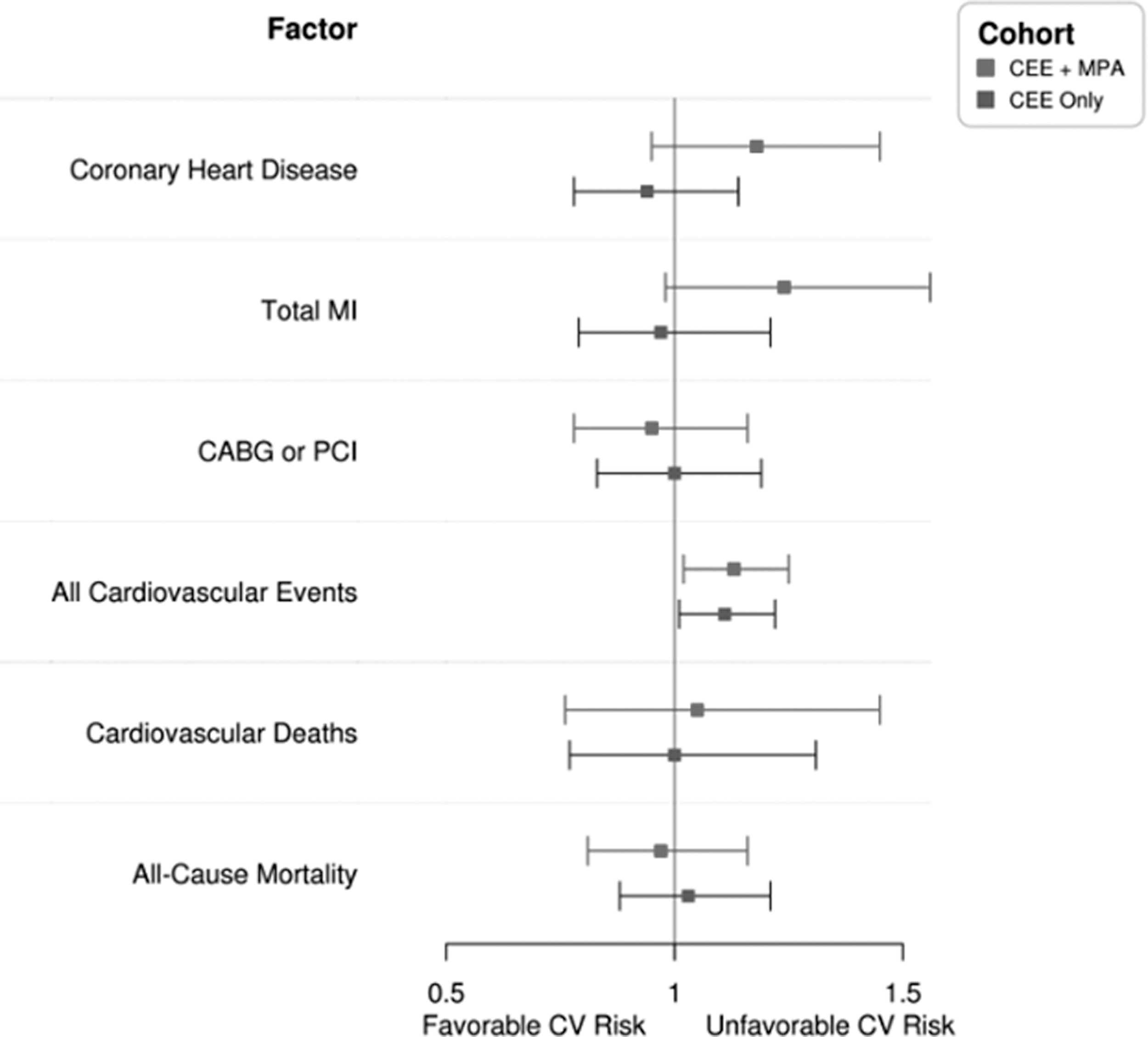
Cardiovascular outcomes in the women's health initiative hormone therapy trials during the intervention phase. CABG, coronary artery bypass grafting; CEE, conjugated equine estrogen; MI, myocardial infarction; MPA, medroxyprogesterone acetate; PCI, percutaneous coronary intervention.
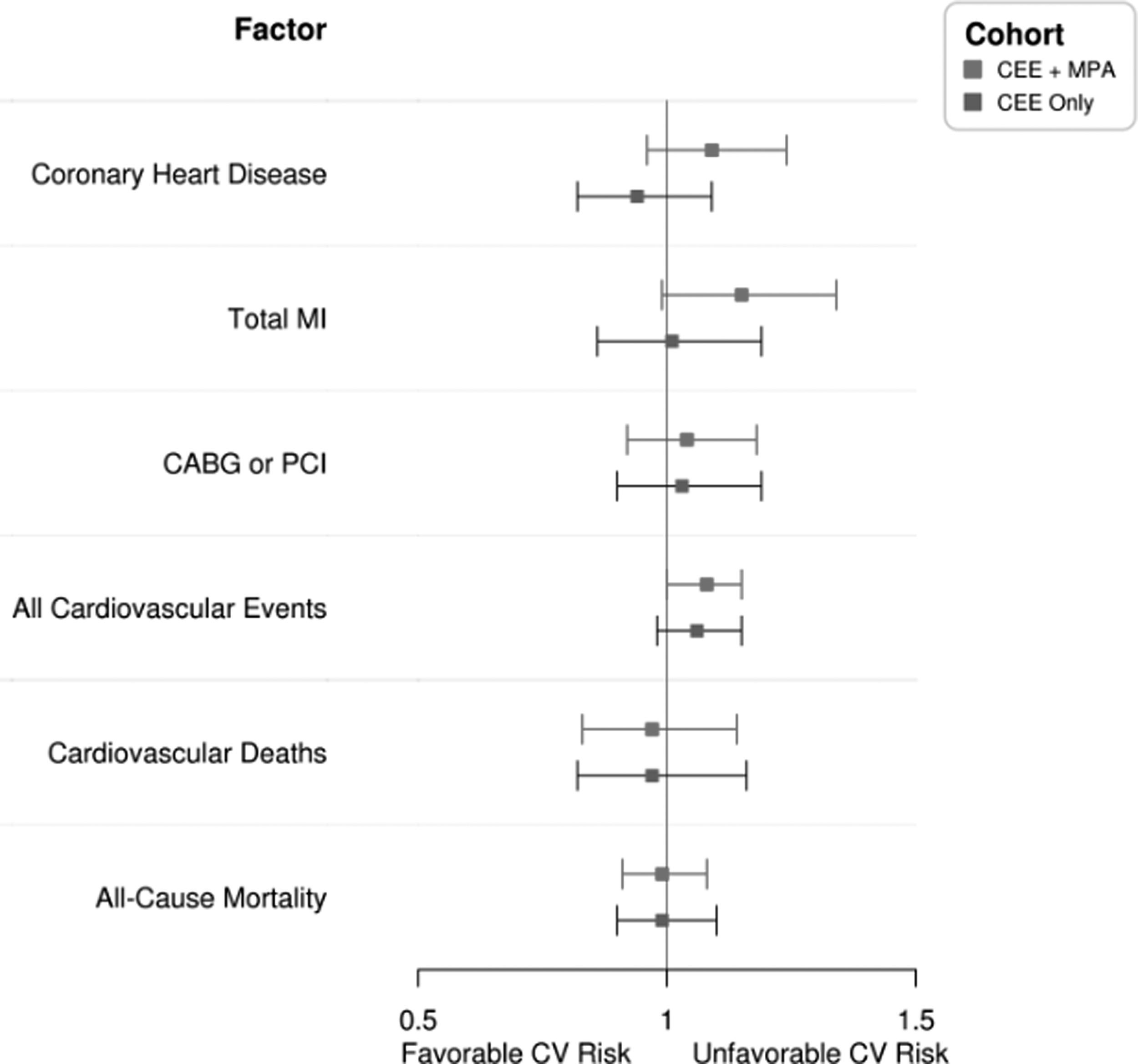
Cardiovascular outcomes in the women's health initiative hormone therapy trials during the extended follow-up phase.
The increased risk of CHD was an unexpected finding in light of the multiple observational and animal study results preceding the WHI, as well as our understanding of the favorable effects of estrogen on cardiovascular risk factors, such as lipids. 29 Evaluation of the design of the WHI showed that women enrolled in the WHI trial were markedly older (average age: 63 years) than the average age of menopause in North America, 51 years of age. 30 This is in contrast to the preceding observational studies in which patients were younger, more symptomatic, and closer to menopause. Subanalysis from the WHI trials showed that stratification by age is important in describing CV risk in women treated with HT. 3,31 In the CEE-only arm, women 50–59 years of age compared with women 70–79 years of age trended toward decreased risk of CHD (HR 0.60, 95% CI 0.35–1.04 vs. HR 1.09, 95% CI 0.80–1.49, p = 0.08), MI (HR 0.55, 95% CI 0.31–1.00, vs. HR 1.24, 95% CI 0.88–1.75, p = 0.02), and coronary artery bypass grafting or percutaneous coronary intervention (HR 0.56, 95% CI 0.35–0.88, vs. HR 1.07, 95% CI 0.79–1.43, p = 0.06). In the CEE+MPA and CEE-only arms, younger women had lower all-cause mortality compared with older women (Fig. 3). In women 50 to 59 years of age on HT, total mortality decreased by 30%; interestingly, women in the same age cohort do not show reduced mortality with aspirin and statin use. 32 Furthermore, postintervention follow-up of 13 years from WHI data found that younger age at the time of HT administration was associated with less CVD risk, a finding that supports that the timing of HT may influence cardiovascular risk (Fig. 2). 28 These data align with the timing hypothesis, demonstrating that younger women (age <60 years) closer to menopause (<10 years) had lower risk of CVD when started HT when compared with older women further from menopause.

Cardiovascular outcomes in the women's health initiative hormone therapy trials during the intervention phase stratified by age. CHD, coronary heart disease.
The DOPS, a large open-label study with no placebo control arm, started at the same time as the WHI; however, its study sample included 1006 younger women between ages 45 and 58 years. Women were randomized to HT with either oral or transdermal triphasic estradiol and norethisterone acetate (those with a uterus) or 2 mg estradiol per day (those without a uterus) or no treatment. 33 The study's main outcome was evaluating effects of HT on osteoporosis. CVD was not a prespecified outcome; however, events, including MI and heart failure, were recorded. Participants receiving HT had a significantly reduced risk of death, MI, and heart failure (as a composite outcome) compared with placebo (HR: 0.48, 95% CI 0.26–0.87, p = 0.015) at 11-year follow-up. 34 Further subgroup analysis found fewer cardiovascular events in those 50–59 years in HT groups compared with placebo. 7,30
RCT and Observational Data Supporting the Cardiovascular Safety of Hormone Therapy
In part, to help rectify the discrepant findings between the WHI and prior observational data, several RCTs have evaluated CVD effects of HT in women closer to menopause. The KEEPS trial was a prospective, randomized controlled trial designed to evaluate the effect of HT on the progression of atherosclerosis measured by carotid intima-media thickness (CIMT) and coronary arterial calcification (CAC) over 4 years. Seven hundred twenty-seven healthy young women (42–58 years) within 6 to 36 months of menopause were enrolled. 3 Exclusion criteria included women with history of MI, angina, congestive heart failure, thromboembolic disease, heavy smoking, morbid obesity, dyslipidemia, hypertriglyceridemia, uncontrolled hypertension, and glucose >126 mg/dL, or CAC score >50 Agatston units. Those who met inclusion criteria were randomized to (1) daily placebo (2) daily oral CEE (0.45 mg/day), or (3) transdermal 17β-estradiol (50 μg/day) with placebo or pulsed progesterone for 12 days/month. 3
In KEEPS, young women within 6 to 36 months of menopause did not develop significant atherosclerotic heart disease during 4 years of treatment with HT. The primary outcome of CIMT measurement was obtained at baseline and at follow-up. The secondary outcome was CAC score obtained at baseline and in follow-up. There was minimal change in CIMT thickness in the follow-up period (0.0072 mm/year in the placebo group [95% CI 0.0058–0.0085], 0.008 mm/year in the CEE group [95% CI 0.0065–0.0095], and 0.0077 mm/year in the transdermal estrogen group [95% CI 0.0061–0.0092]) 13 (Fig. 4). The mean difference in rate of CIMT change between placebo and treatment groups were nonsignificant (CEE compared with placebo 0.0008 mm/year [95% CI −0.0012 to 0.0029, p = 0.43], transdermal estrogen compared with placebo 0.0005 mm/year [95%CI −0.0016 to 0.0026, p = 0.64]) suggesting that HT was not associated with a significant progression of subclinical atherosclerosis compared with placebo. 13 Baseline CAC scores were remarkably low, with >86% of participants in each group having a CAC score of 0 Agatston units, a level associated with a 1% risk of MI, stroke, or cardiovascular death in 10 years. 35 Participants experienced increases in CAC score (defined as any increase in score if initial score is 0, and an increase of >5 Agatston units if initial score was >0), but these increases were not significant between groups (21% of participants in the placebo group, 17.4% in the CEE only group [p = 0.36 when compared with placebo], and 18.9% in the transdermal estrogen group [p = 0.59 when compared with placebo]). 13 Additional findings include a favorable change in lipid profile with an increase in high-density lipoprotein and decrease in low-density lipoprotein in women treated with CEE only, and a neutral effect on blood pressure in both groups. 30,34
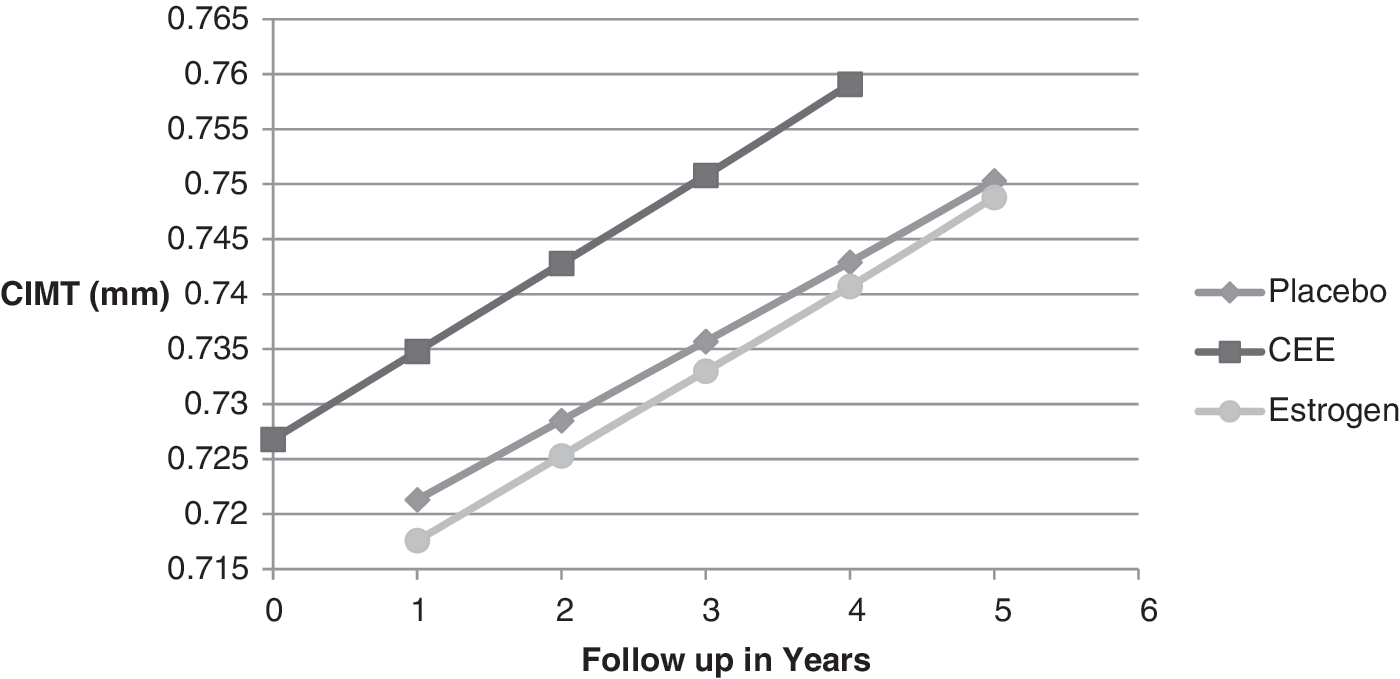
Carotid intima-media thickness (CIMT) measurement over time: KEEPS Trial.
The ELITE trial was designed to test the timing hypothesis by enrolling women in early menopause as well as those later in menopause to evaluate HT effects on CV risk. Six-hundred forty-three women <6 and ≥10 years from menopause and without pre-existing CVD were enrolled in a randomized, double-blind, placebo-controlled trial. The mean age was 55 years in the early postmenopause group, and 65 years in the late postmenopause group. Women were randomized to receive oral 17β-estradiol (1 mg/day) with pulsed vaginal progesterone (45 mg vaginal gel once daily for 10 days in women with a uterus) or placebo for 5 years. Primary outcomes included changes in CIMT measured every 6 months and the secondary outcome included change in CAC. 34
The ELITE trial found that, similar to the KEEPS trial, treatment with HT was not associated with significant progression of subclinical atherosclerosis in women early postmenopause (Fig. 5). The population enrolled in the ELITE trial had greater CV risk factors than in the KEEPS trial. Women in the late menopause group were more likely to be treated with antihypertensives and cholesterol-lowering medications, and had higher baseline CIMT and more CAC present. Women in the late postmenopause had a greater increase in CIMT measurements compared with early postmenopause, and importantly, the early postmenopause participants treated with estradiol had the lowest rate of change in the study population (0.0044 mm/year [95% CI 0.0026–0.0061] in the estradiol group versus 0.0078 [95% CI 0.0060–0.0096, p = 0.008]).
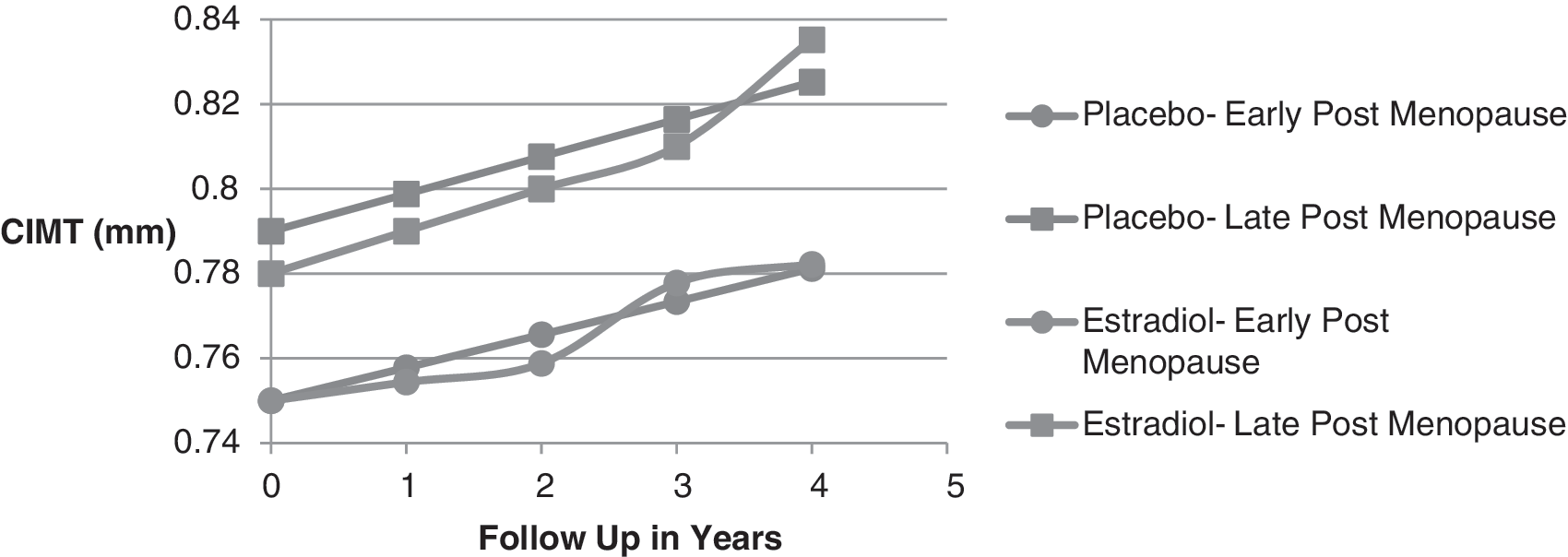
CIMT measurement over time: ELITE Trial.
The outcome of CIMT and CAC progression used in the KEEPs and ELITE trials are intermediate measures of subclinical atherosclerosis. CIMT studies have shown conflicting results in its ability to predict hard cardiovascular events. 36,37 On the other hand, CAC progression has been associated with increased risk of hard cardiovascular events, including MI. 38 The KEEPS and ELITE trials showed minimal progression of subclinical atherosclerosis, which does provide reassurance that HT may be safe in appropriately selected women. Also reassuring was a Cochrane review of 19 RCTs by Boardman and colleagues who concluded that HT started within 10 years of menopause onset lowered CHD in menopausal women (RR: 0.52, 95% CI 0.29–0.96). 39 Overall, the data supporting HT as safe in terms of future cardiovascular risk is of moderate quality such that further research may impact confidence in these findings. Decisions to treat must be weighed with the individual woman's menopausal symptoms and personal risk for CVD, stroke, and venous thromboembolism. Additionally, it is important to understand a difference exists between formulations and types of HT (transdermal vs. oral, CEE vs. 17β-estradiol) and this needs to be incorporated into conversations regarding individualized treatment. Future research to clarify how route and administration impact HT-associated risk is also warranted.
Guideline Recommendations
Current menopause guidelines highlight the evolving understanding of the low risk of CVD with HT early in menopause, and embrace treatment for symptomatic menopausal women given the favorable benefit versus risk profile. The NAMS 2017 hormone therapy position statement changed from previously endorsing “[using] the smallest dose [of HT] possible for the shortest period of time” to “For women aged younger than 60 years or who are within 10 years of menopause onset and have no contraindications, the benefit–risk ratio is most favorable for treatment of bothersome [vasomotor symptoms] and for those at elevated risk for bone loss or fracture.”2 The American Association of Clinical Endocrinologist, The Endocrine Society, and ACOG recommend consideration of hormone therapy for the symptomatic treatment of menopause. 16,17,40
The United States Preventive Services Task Force (USPSTF) recommends against the use of combined estrogen and progestin in postmenopausal women and against the use of estrogen alone in postmenopausal women who have had a hysterectomy for the primary prevention of chronic conditions. 41 However, this guideline is specifically aimed at clinical preventive services in asymptomatic patients considering HT for primary prevention of chronic medical conditions. It does not pertain to those using HT for treatment of menopausal symptoms (i.e., VMSs and vaginal dryness), and those with premature menopause or surgical menopause. 41 While the USPSTF guideline acknowledges the timing hypothesis and comments on the post hoc analysis of the WHI data, it reports that not enough data or trials have tested this hypothesis in relation to benefits and harms in the context of primary prevention.
Conclusion
While updated recommendations do not endorse HT for primary prevention of chronic conditions, it is encouraging that recent data support the timing hypothesis and that initiation of HT within 10 years of menopause onset and in women <60 years of age does not appear to increase CV risk. Furthermore, it is well established that HT significantly reduces the VMS associated with menopause, thus improving quality of life. Current evidence suggests that in appropriately selected symptomatic women, HT could be considered. Still, it is important to weigh the benefits against the risks, including the rare risk of breast cancer, venous thromboembolism, and stroke. Understanding the safety profile of HT will lead to providers who are better equipped to address the important concerns, symptoms, and quality-of-life issues of their menopausal patients.
Footnotes
Author Disclosure Statement:
No competing financial interests exist.